


Abstract
This prospective study investigates the relationship between glucose transporter-1 (Glut-1) expression and PET images using 18F-FDG and its uptake and compares them with the tumor status (primary vs. recurrent or persistent), initial grade of histologic differentiation, and International Federation of Gynecologic Obstetrics (FIGO) staging for cervical cancer patients. Methods: A dual-phase 18F-FDG PET scan was performed on 51 participants within the 2 wk before surgery or biopsy. 18F-FDG uptake was quantified by calculating standardized uptake values (SUVs). After 18F-FDG PET scanning, 51 histologically proven squamous cell carcinoma specimens were examined to determine their degree of differentiation, using hematoxylin and eosin staining, and the expression of Glut-1 by an immunohistochemical stain. Twenty normal cervical and 20 cervical intraepithelial neoplasia (CIN) sets of tissue were also used to compare the results of Glut-1 expression in these tissues. The expression of Glut-1 was the product of (the intensity [with grades 0–3, defined qualitatively]) with (percentages of the lesion area that were positive). The results of Glut-1 expression were analyzed in combination with the SUVs (SUV1 was that at 40 min and SUV2 was that at 3 h), tumor status, initial cell differentiation, and FIGO staging. Results: Significant overexpression of Glut-1 was noted in 48 of the 51 (94.1%) cancer specimens. None or only minimal expression of Glut-1 was observed in basal layers of normal and CIN tissues. Significant positive correlation was observed between Glut-1 expression and the SUVs in cervical cancer specimens (r = 0.74, P < 0.000 for SUV1 and r = 0.65, P < 0.000 for SUV2). In recurrent or persistent tumor, tumor size was significantly associated with both Glut-1 expression (r = 0.508, P = 0.011) and SUV1 (r = 0. 456, P = 0.025). For recurrent or persistent tumor, only SUV1 reached statistical significance when compared with lymph node metastasis (P = 0.0226). Conclusion: Glut-1 expression was related to 18F-FDG uptake in cervical cancer patients. Recurrent or persistent cervical cancer tumor had significantly higher Glut-1 expression than metastatic lymph nodes. The values of SUV and the expression of Glut-1 did not correlate with the initial grade of histologic differentiation and FIGO staging.
Cancer cell growth is an energy-related process supported by increased glucose metabolism. This phenomenon was first demonstrated in cell culture by Isselbacher in 1972 (1). Since then, many kinds of malignant cells have shown increased glucose uptake both in vitro and in vivo. This uptake is believed to be mediated by glucose transporters (Gluts), which are membrane proteins responsible for the transport of glucose across cellular membranes (2–5). Human Gluts have a distinct tissue distribution and contribute to the disposal of glucose under various conditions (6). Among Gluts, Glut-1 and Glut-3 have been proven to show overexpression in both messenger RNA and protein in a variety of cancer cells (7–11). So, Glut-1 and Glut-3 may play an important role in glucose uptake by these cancers and could be a useful biomarker for malignant transformation.
PET using 18F-FDG has been shown to be a useful tool for imaging primary and recurrent cervical cancer (12–16). Although overexpression of Glut-1 was important for 18F-FDG uptake in cancer cells, other factors—such as overexpression of hexokinase II and underexpression of glucose-6-phosphatase (G-6-Pase)—were also observed in many tumor cells. Therefore, recent studies showed that the dual-phase 18F-FDG PET scan is valuable in detecting malignant lesions (10,16,17). Glut-1 was considered as an intrinsic marker of hypoxia that can be applied to the clinical setting. Also, in cervical cancer it can predict an improved metastasis-free survival in the absence of Glut-1 expression (18). However, the possible associations of Glut-1 expression with other clinicopathologic parameters and 18F-FDG PET findings have not yet been elucidated in human cervical cancer, although they have been studied in many other cancers, such as carcinoma of lung, pancreas, and breast (7,10,11,19). Therefore, we conducted a prospective study to determine the association between Glut-1 expression and the standard uptake values (SUVs) obtained from 18F-FDG PET scans. The relationship between Glut-1 and SUVs with disease or tumor characteristics and International Federation of Gynecologic Obstetrics (FIGO) staging or recurrent or persistent tumors of these cervical cancer patients was also investigated.
MATERIALS AND METHODS
Patients
The institutional review and ethics boards of our hospital approved this study. Written informed consent was obtained from all patients who participated. A patient was eligible if she satisfied criteria (a) and (f) plus 1 other criterion from (b) to (e). These criteria are as follows: (a) histologic diagnosis of squamous cell carcinoma of cervix (SCCC); (b) previously untreated and scheduled for radiotherapy of curative intent, with at least one enlarged pelvic lymph node (≥1.0 cm in its maximal dimension) or groups of small pelvic nodes (size, <1 cm) and without suspected paraaortic lymph node metastasis or any other extrapelvic lesion visualized with MRI; (c) suspicious paraaortic nodes on MRI or clinically palpable supraclavicular or inguinal nodes without other overt distant metastasis, for which treatment of curative intent is still feasible; (d) histologically proven recurrent or persistent cancer after definitive radiotherapy or surgery and willing to receive salvage therapy of curative intent; (e) unexplained squamous cell carcinoma antigen (SCC-Ag) or carcinoembryonic antigen (CEA) elevation (SCC-Ag > 2 ng/mL or CEA > 10 ng/mL on 2 tests 1 mo apart); and (f) willing to receive a CT- or ultrasound-guided biopsy or surgical exploration if indicated.
In this study, a 18F-FDG PET scan was performed on all participants in the 2 wk before surgery or biopsy. Designation of clinical stage was according the FIGO stage. After 18F-FDG PET scanning, 51 histologically proven SCCC specimens from 51 cervical cancer patients were examined for determination of the degree of differentiation by hematoxylin–eosin staining and the expression of Glut-1 by immunohistochemistry. Twenty normal cervical and 20 cervical intraepithelial neoplasia (CIN) sets of tissue were used to compare the results of Glut-1 expression in these tissues. The CIN cases were randomly picked and ranged from CIN-I to CIN-III.
PET Imaging, Image Analysis, Image Reconstruction, and Coregistration
Using 18F-FDG produced by the Institute of Nuclear Energy Research of Taiwan, 18F-FDG PET scans were performed (with a 4.5-mm full width at half maximum and a 15-cm transaxial field of view). The PET camera used was an ECAT EXACT HR+ (CTI). Patients fasted for at least 6 h before PET imaging. Data acquisition and reconstruction were according to our previous study (20).
For semiquantitative analysis, the SUVs were obtained by placing regions of interest (ROIs) around the lesions that had previously been identified as suspicious by visual analysis, according to our previous study (21). To minimize partial-volume effects, the maximum SUV within an ROI was used. SUV1 was defined as the SUV in the image acquired from 40–96 min after injection, whereas SUV2 was defined as the SUV from the later image (180–210 min after injection). Three nuclear physicians, who were unaware of other imaging results and clinical data, analyzed the 18F-FDG PET images on an interactive computer display, with at least 2 agreeing with each other. Any obvious foci of increased 18F-FDG uptake were evaluated using transaxial, sagittal, and coronal displays and compared between the 40-min and 3-h scans.
Coregistration was used for those situations where there were discrepant image findings between 18F-FDG PET and CT. PET images were reconstructed using segmentation and a standard iterative algorithm (ordered subsets expectation maximization, 2 iterative steps). Images were reformatted into axial, coronal, and sagittal views. Before coregistration of all images, CT data were resampled using the resolution of the PET scan (a 128 × 128 matrix) in the transaxial plane, although the original CT images were also available for viewing at all times. Coregistration of PET and CT images was done using Hermes software (version 4.2C; Nuclear Diagnostics Ltd.), which allows the registration of 2 sets of images with a simple rigid transformation based on anatomic landmarks.
CT-Guided Biopsy
All CT-guided biopsy procedures were performed by experienced radiologists. The patients were placed on the CT table in the prone position for paraaortic node biopsy or in the supine position for pelvic node biopsy. The CT images were scrutinized to plan the biopsy pathway to avoid injury of the adjacent visceral organs or vascular structures. After subcutaneous injection of local anesthesia (2% xylocaine), the coaxial introducer needle (17- or 19-gauge, Temno biopsy device; Allegiance Healthcare Corp.) was advanced percutaneously toward the target lesion. Repeated CT scans were performed during the interval of the needle advancement to ensure the optimal trajectory of the introducer needle. When the introducer needle reached the surface of the target lesion, a biopsy needle (18- or 20-gauge) was advanced through the introducer needle into the target lesion. Another CT scan was done to confirm that the biopsy needle tip was well located inside the lesion. Then, a cut biopsy was performed and a core of tissue was obtained after withdrawal of the biopsy needle. The introducer needle was left in place for 2 or 3 additional tissue samplings. All tissues were fixed in formalin for pathologic examination.
PET Probe
The PET probe used in this study contains a γ-detector probe and a β-sensitive probe. The γ-detector probe used in this study was the Neoprobe 1000 Instrument (Neoprobe Corp.). The β-sensitive probe used in this study was manufactured by Crystal GmbH and marketed by Nuclear Fields Technology. The probe (CSX-OPSZA) contains 90% collimation with internal shielding and is used with control unit SGO3 with the nuclide selector set for use with PET (511 keV).
The PET probe was applied for patients intraoperatively with discrepant image findings (positive for 18F-FDG PET scan, but negative for MRI or CT). Preoperatively, patients were given 18F-FDG mixed in normal saline via an intravenous infusion over a 5-min period. The amount injected depended on results from a previous 18F-FDG PET scan, the operative procedure underway, or body size. Patients were maintained in Fowler’s position until general anesthesia was induced 30–90 min later to facilitate excretion of the radiopharmaceutical. A bladder catheter was placed after induction of anesthesia and 10 mg of furosemide was given by intravenous push to facilitate excretion of unbound radiopharmaceutical. During laparotomy, the biodistribution of 18F-FDG was assessed with each probe to determine background activity in kidney, liver, aorta, and urinary bladder as well as in those areas noted to be 18F-FDG-avid on preoperative PET scans. The PET γ-detector probe was used to detect the 18F-FDG-avid lesion during operation. After removing the 18F-FDG-avid specimen(s), counts were taken over a 2-s period and recorded with both β- and γ-probes. For normal adjacent tissue, counts were also determined and compared for each probe. All resected specimens were confirmed histologically to be tumor tissue.
Immunohistochemical Examination
Preparation, examination, and estimation of Glut-1 expression of tumor tissues were according to the methods of Higashi et al. with some modifications (10,11). Tumor tissues were fixed in 10% neutral buffered formalin for 12 h, and standard dehydration and paraffin- or wax-embedding procedures were used on the fixed tissues. Serial sections from the paraffin-embedded tissues were stained for Glut-1 and with hematoxylin. The polyclonal rabbit antiglucose transporter antibody is reactive to human Glut-1 (brain or erythrocyte type) and was purchased from DAKO. Immunoreactions with Glut-1 were performed on human erythrocytes, normal cervical and CIN tissues, and a variety of human cancer cells. Anti-Glut-1 antibody was diluted 1:200 with 0.05 mol/L Tris-HCl buffer containing a carrier protein and 0.015 mol/L sodium azide (DAKO). Immunohistochemical analysis for anti-Glut-1 antibody was independently performed 3 times by 2 experienced pathologists who were unaware of the SUVs and clinical data. In each analysis, the percentages of strongly immunoreactive tumor cells among all tumor cells were visually analyzed using a minimal of 3 low-power fields (up to 30 fields) with a ×10 magnification. The percentage of the Glut-1–positive area was scored on a semiquantitative scale as 0%–100%. Less than 5% staining was categorized as zero. The average percentage of the positive area was calculated for 10 fields for each of the specimens. The levels of Glut-1 expression in this study were defined as (the intensity grade) × (the percentage of tumor area that is positive) (11).
Statistical Analysis
Descriptive statistics—including means, SDs, and scatter plots—were used. Pearson correlation coefficients (r) were computed to indicate the degree of linear relationship among continuous variables. The Wilcoxon rank sum test or the Kruskal–Wallis test was performed to compare either Glut-1 or SUVs with each of the degrees of differentiation level and clinical status. Multiple linear regression with forward selection was used to identify important variables predicting Glut-1 expression. Residual analysis was performed to confirm the statistical assumption that the conditions for multiple linear regression were being met. Cook’s distance was examined to avoid the regression model being excessively influenced by outliers (22,23). The importance of interaction between the selected variables was tested using the partial F test. All P values were 2-sided, and the significance level was 0.05.
RESULTS
Between March 2001 and November 2002, 51 SCCC specimens (27 moderately differentiated, 24 poorly differentiated) from 51 patients (age range, 28–87 y; mean age, 56.3 ± 13.2 y) were studied. Of the 51 patients, 25 had newly diagnosed cervical cancer (stage ≤ IIA in 8 and stage ≥ IIB in 17), and 26 had documented recurrent or persistent cervical cancer or unexplained elevation of tumor markers (interval time from the last treatment, 6.2–74.5 mo). Of the 25 primary cervical cancer patients, all 8 patients with FIGO stage ≤ IIA had radical surgery. For those with FIGO stage ≥ IIB (n = 17), 2 had radiation therapy alone and 15 had concurrent chemotherapy and irradiation therapy. Of the 26 patients with recurrent or persistent tumors, 10 had salvage therapy with exenterative surgery and 5 had laparotomy for tissue proof (including 2 with intraoperative PET probe [18F-FDG, 74 MBq (2 mCi) and 185 MBq (5 mCi)]). Of the 51 SCCC specimens, 35 were primary, recurrent, or persistent tumor; 15 were metastatic lymph nodes; and 1 was a colon metastatic lesion. Among them, 23 had had exploratory laparotomy (including 2 with use of the intraoperative probe, with tumor-to-normal tissue ratios of 1.78 and 1.53) and 28 had CT-guided biopsy. All of these lesions were detected by a preoperative PET scan. In 20 normal cervical specimens, most had Glut-1–positive cells only in the basal layer that measured <5% of the epithelial cell population (Fig. 1A). In 20 CIN tissues, the estimation was performed on the dysplastic cells. Only 3 (15%) had a minimal expression of Glut-1 in the dysplastic cells in basal layers (Fig. 1B). Of the 51 cervical cancer specimens, 48 (94.1%) showed overexpression of Glut-1 (Fig. 1C). However, the remaining 3 (5.9%) had minimal expression of Glut-1 (Fig. 1D). In comparison, the variations of Glut-1 expression between intraobserver and interobserver were low (4.47% ± 2.28% and 4.06% ± 2.17% for intraobserver variations for the 2 observers and 8.61% ± 6.65% for the interobserver variation).

(A) Normal cervical specimen from patient with uterine myoma, in which little Glut-1 was found in basal layer. (B) Patient with CIN-III and cervical specimen showed minimal expression of Glut-1 in its dysplastic cells. (C) Patient with stage IIB bulky cervical cancer. Overexpression of Glut-1 in cervical cancer tumor was observed, mainly in cervical cancer cell membrane. (D) Patient with cervical cancer who had previous radiation therapy and central recurrence. 18F-FDG PET scan was false-negative and only minimal Glut-1 expression was observed in specimen.
Relationship Between SUV1 and SUV2 Versus Glut-1 Expression
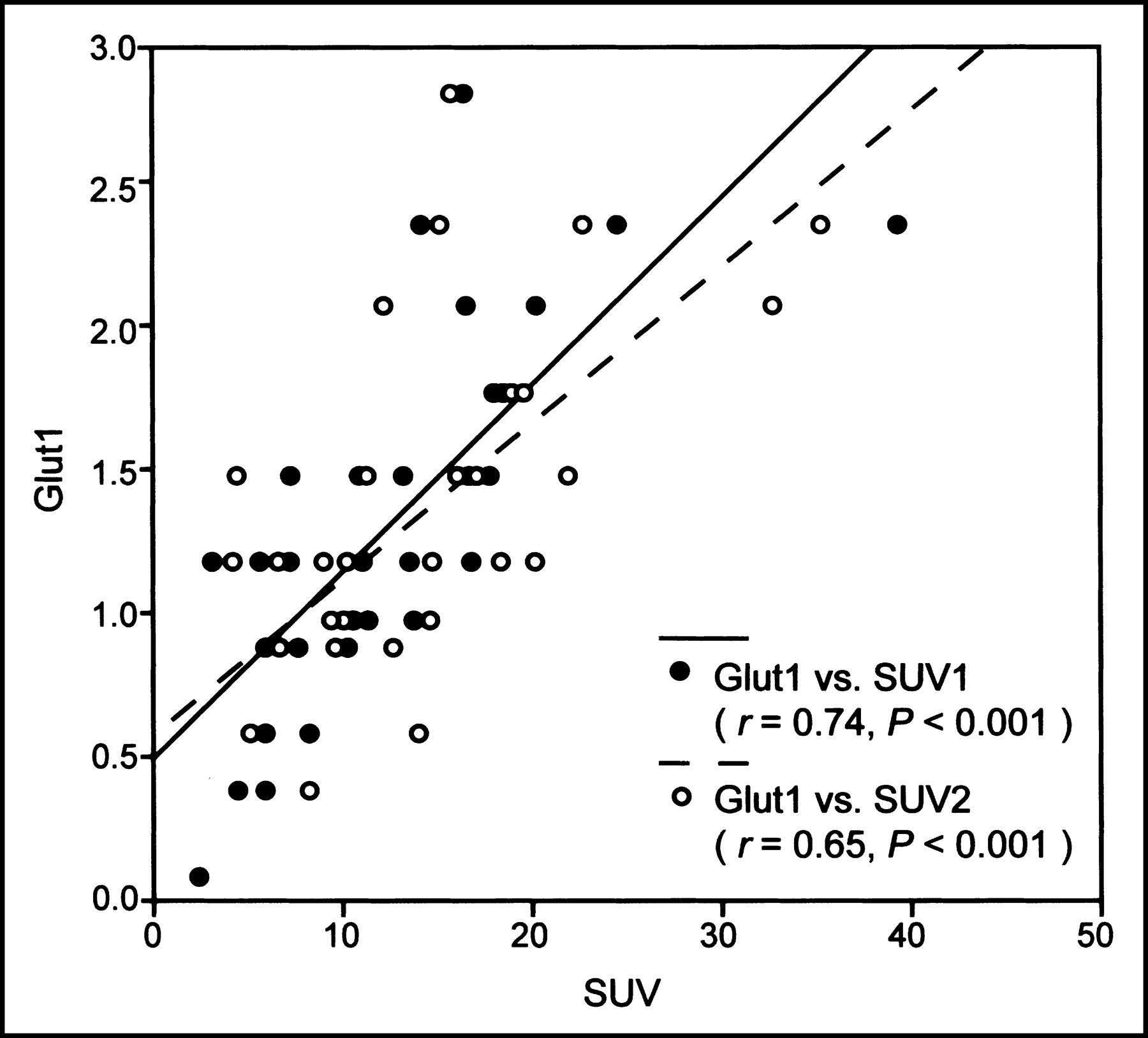
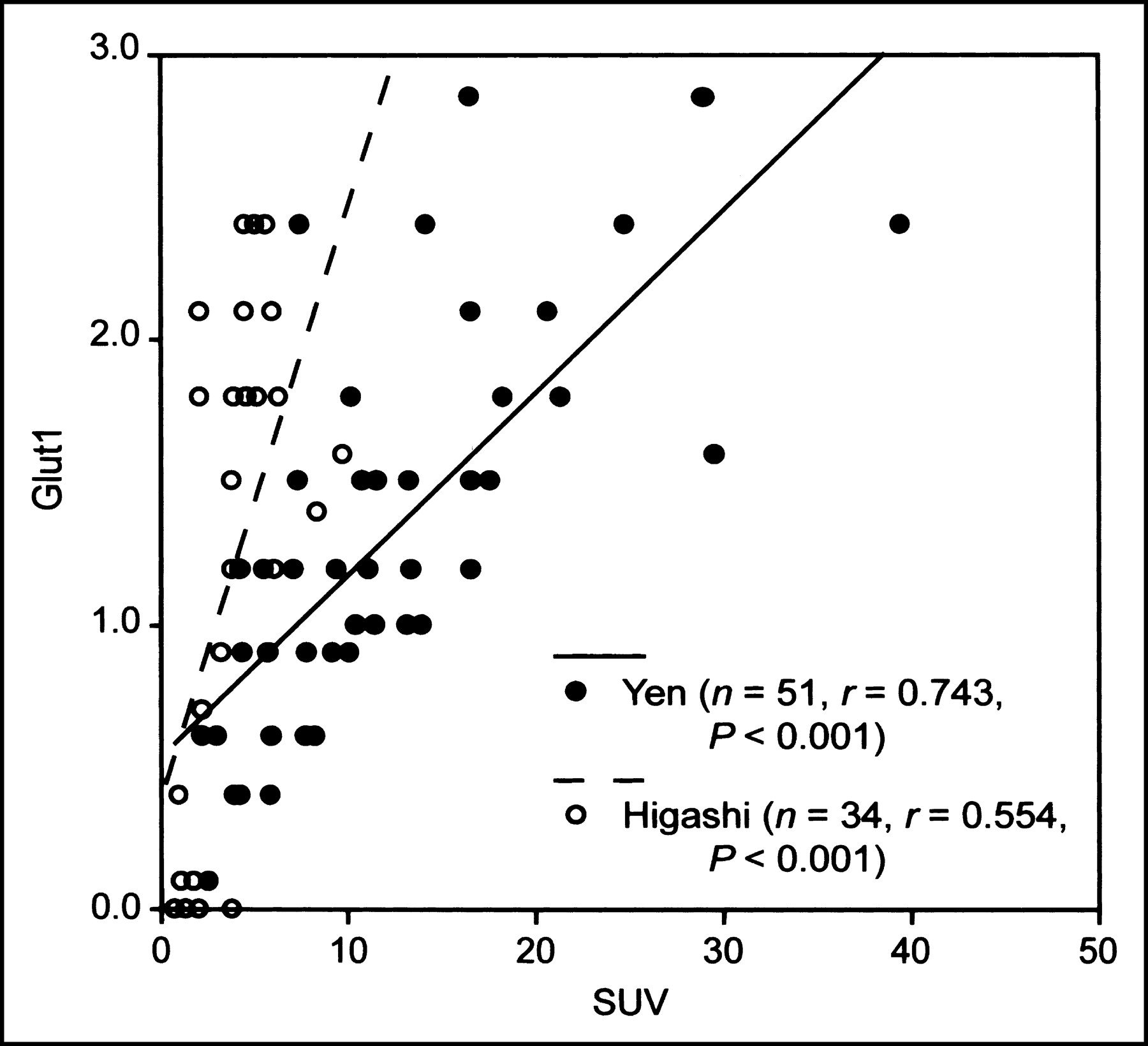
Totally, 32 patients had both early and delayed PET images and 19 patients had only early PET images; the SUV2 was available in 32 patients. SUV1 and SUV2 was highly and positively correlated for both primary (r = 0.832, P < 0.001) and recurrent or persistent tumor (r = 0.973, P < 0.001) (Fig. 2). Due to the close correlation of Glut-1 expression and 18F-FDG uptake in lung, pancreas, and breast cancer and the lack of availability of data for SCCC so far (7,10,11,19), in this study we compared the relationship between SUV1 and SUV2 versus Gut-1 expression. Figure 3 shows the scatter plot between immunohistochemical findings of Glut-1 and the parameters of dual-phase 18F-FDG PET (SUV1 and SUV2). A significant positive correlation was observed between the SUVs and Glut-1 expression (r = 0.74, P < 0.001 for SUV1 and r = 0.65, P < 0.001 for SUV2). For comparison with the data of both Higashi et al. (11) and Brown et al. (19) in lung cancer, we used SUV1 and SUV1 corrected for lean body mass (SUL) in this study. Our data showed a better correlation of Glut-1 expression with 18F-FDG uptake for cervical cancer than that shown for lung cancer (Figs. 3 and 4) (r = 0.74, P < 0.001 for this study vs. r = 0.55, P < 0.001 as reported by Higashi et al. using SUV and r = 0.504, P < 0.001 for this study, vs. r = 0.007, P < 0.976 for the data of Brown et al. using SUL) (Fig. 5) (11,19).

Results of comparative analysis of primary and recurrent or persistent tumor from dual-phase 18F-FDG PET scans. Highly positive correlation between SUV1 and SUV2 was observed for primary tumor (r = 0.832, P < 0.001) and recurrent or persistent tumor (r = 0.973, P < 0.001).
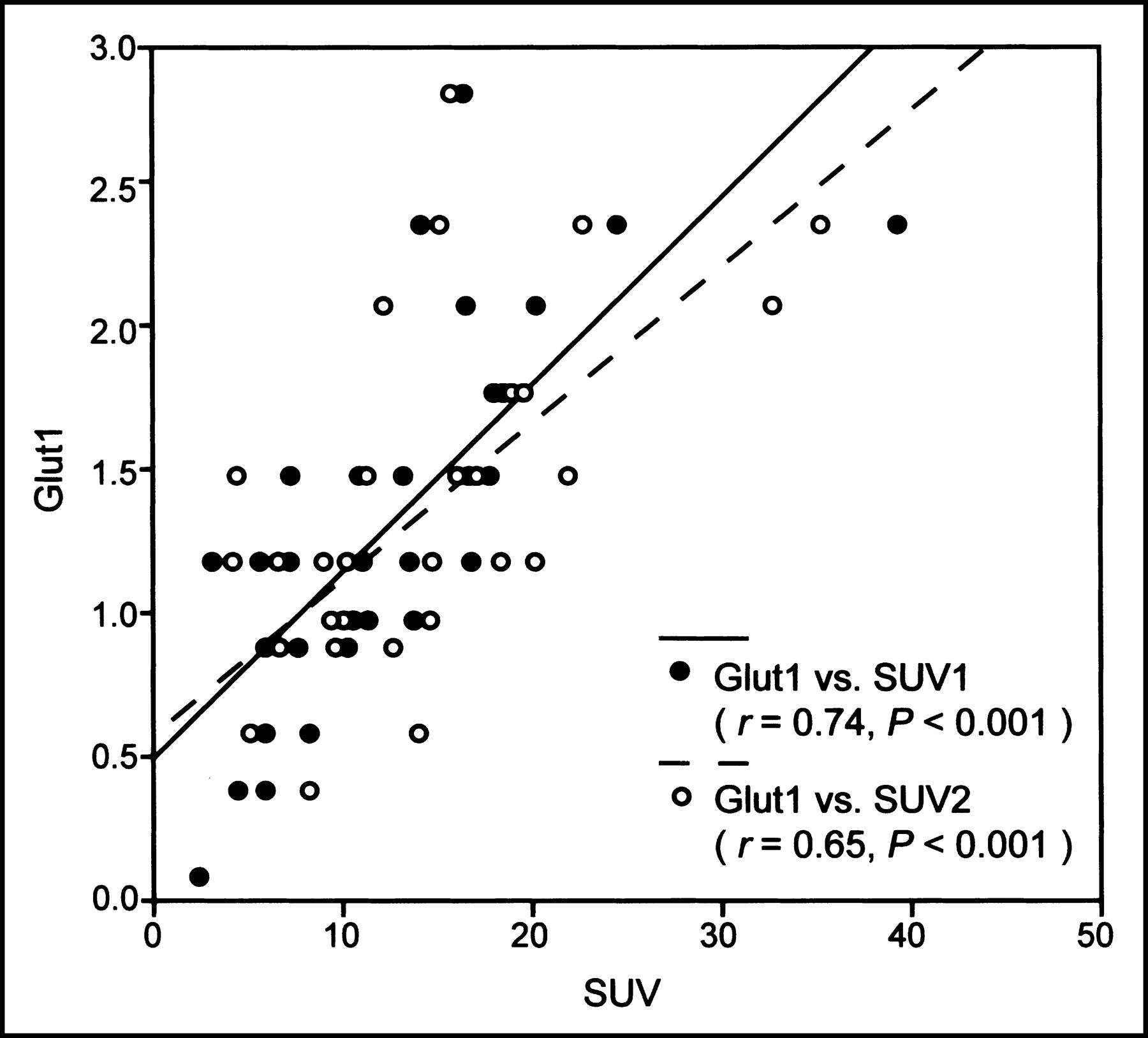
Results of comparative analysis of maximum SUV from dual-phase 18F-FDG PET scans and results of immunohistochemical staining. There is significant positive relationship of SUVs with Glut-1 expression (r = 0.74, P < 0.001 for SUV1; r = 0.65, P < 0.001 for SUV2).
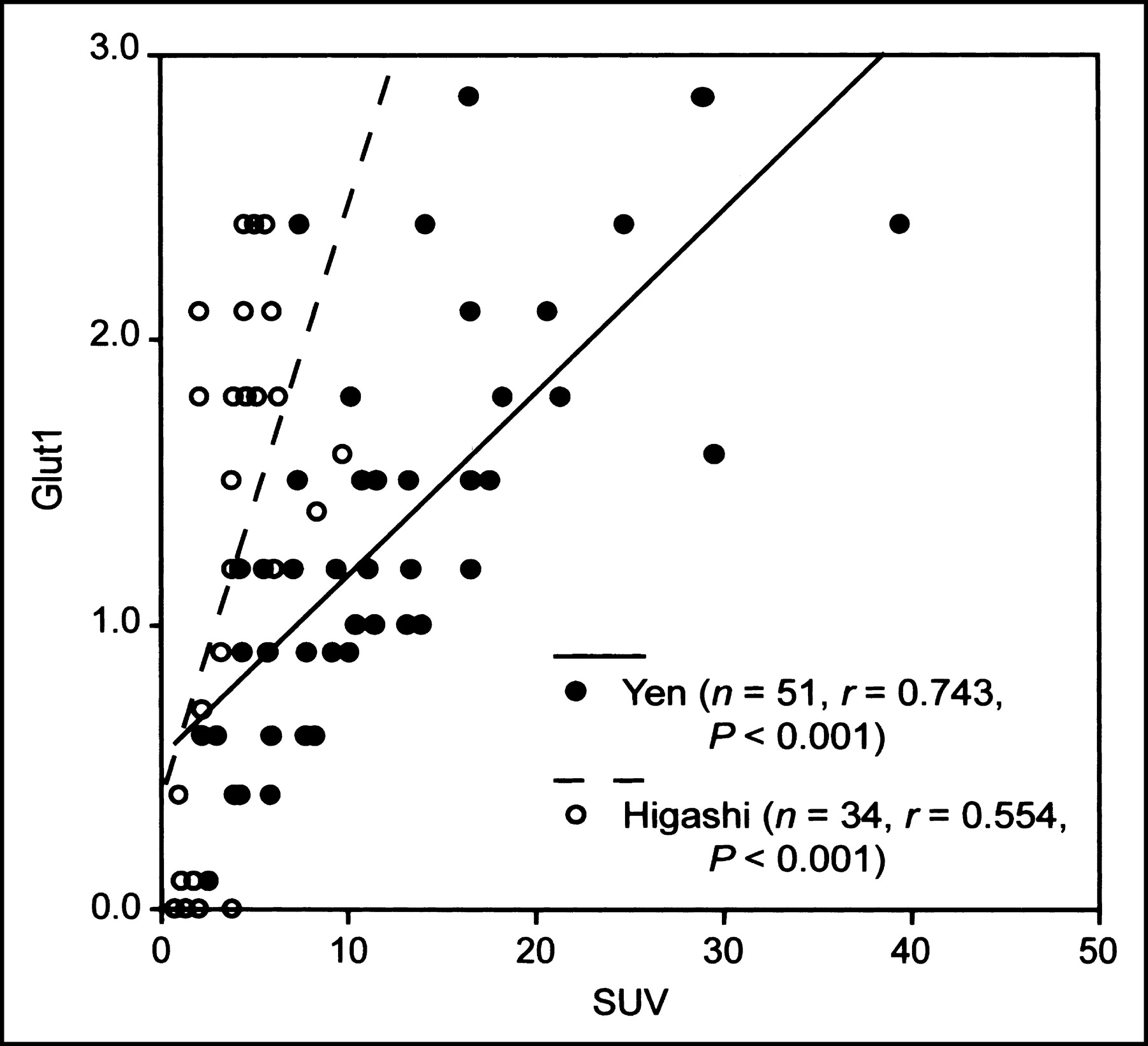
Comparison of results from work of Higashi et al. (○) and our data (•); slope of relation between Glut-1 expression and maximum SUV from dual-phase 18F-FDG PET scans is steeper for lung cancer than that for cervical cancer and correlation coefficients are larger (r = 0.74, P < 0.001 vs. r = 0.55, P < 0.001).
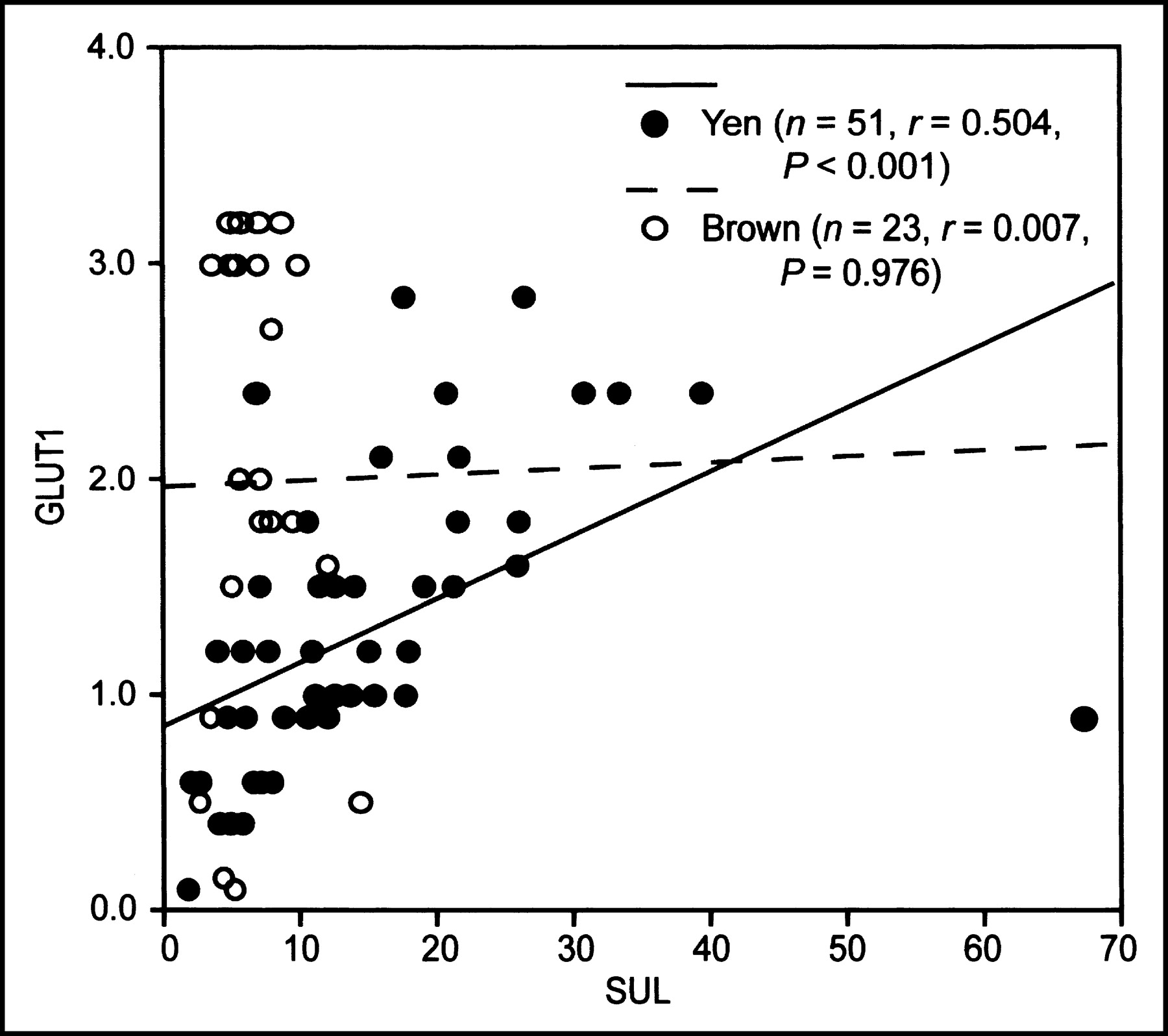
If results for SUL are used in place of maximum SUV, our data (•) for cervical cancer show more significant correlation than data of Brown et al. (○) for lung cancer (r = 0.504, P < 0.001 vs. r = 0.007, P < 0.976).
Univariate Analysis for Glut-1 Expression and SUVs
Glut-1 expression was marginally different between patients with primary tumor (1.44 ± 0.54) and those with recurrent or persistent tumor (1.19 ± 0.75) (P = 0.0612). SUV1 was significantly higher in patients with primary tumor (15.25 ± 6.56) than those with recurrent or persistent tumor (9.37 ± 7.79) (P = 0.005). Due to the substantial differences of tumor sites in patients with primary and recurrent or persistent tumors (tumor status), data were stratified by tumor status. For primary cervical cancer patients, there was no significant association of both Glut-1 expression and SUV1 with age, initial degree of cell differentiation, initial FIGO staging, tumor size, and tumor site (Table 1). For patients with recurrent or persistent tumors, the tumor size was statistically associated with Glut-1 expression (r = 0.508, P = 0.011) and SUV1 (r = 0.456, P = 0.025). Moreover, SUV1 was significantly higher in the main tumor (12.99 ± 10.40) than that in lymph node metastasis (6.03 ± 2.58) (P = 0.0226). Although Glut-1 expression was lower in lymph node metastases (0.91 ± 0.56) than recurrent or persistent tumor (1.39 ± 0.76), there was no significant difference (P = 0.121).
Univariate Analysis for Glut-1 or SUV1
Multivariate Analysis for Glut-1 Expression
Since SUV2 values were available in only 32 patients, it was not included in the multiple linear regression with forward selection to select important predictors for Glut-1 expression. For both primary and recurrent or persistent cancer, SUV1 was an important predictor selected (both P < 0.001). As the slope and intercept were not significantly different between 2 equations (1 for primary tumor [P = 0.9556] and 1 for recurrent or persistent cancer [P = 0.6365]), data were combined and a new equation was obtained. SUV1 explained 55% variation of Glut-1 expression (Table 2). Residual analysis and influence analysis also indicated that all statistical assumptions were met.
Multiple Linear Regression of Glut-1
DISCUSSION
Increased Glut-1 expression correlates with increased glucose metabolism and utilization. Thus, overexpression of Glut-1 is observed in a variety of human tumors (7–11) due to a high metabolic rate and fast growth in an environment that often is unnatural, or less than ideal from a physiologic standpoint. Recently, 18F-FDG PET has been shown to be a useful tool for more effective recognition of both the main tumor and metastatic lesions in primary and recurrent cervical cancer patients (12–16). Also, the associations of Glut-1 expression, cell differentiation, clinical status, and the SUVs in a 18F-FDG PET scan have been studied in many cancers, such as carcinoma of lung, pancreas, and breast (7,10,19). However, to the best of our knowledge, it has not been reported in cervical cancer.
Correlation between the retention index and hexokinase (HK) expression, instead of Glut-1 expression, obtained from dual-phase 18F-FDG PET scanning has been reported (10). This is reasonable and showed that dual-phase 18F-FDG PET scanning did not add more in the evaluation of immunohistochemical expression of Glut-1. Our current study also showed a better correlation coefficiency of Glut-1 versus SUV1 (r = 0.74) than SUV2 (r = 0.65) (Fig. 3); therefore, we compared the results of SUV1 (or SUL) and Glut-1 expression in our study (cervical cancer) and that of others (lung cancer). Our study shows that the correlation of SUVs (or SUL) and Glut-1 is close but more significant in our work than that reported by others (Figs. 4 and 5) (11,19). We believe that such differences are due to at least 5 reasons. First, there are at least 3 subtypes of Glut (Glut-1, Glut-3, and Glut-5) that regulate glucose uptake in lung cancer (16,24,25). To the best of our knowledge, glucose utilization in cervical cancer is mainly through Glut-1 (18,26). Second, some of the specimens in this study were obtained from biopsies taken after coregistration of the different imaging modalities (n = 28) or intraoperatively with the PET probe (n = 2). Therefore, the specimen obtained was compatible with the region of a maximum SUV value, as determined in a 18F-FDG PET scan. Third, step sectioning was performed and the highest score was chosen in this study to minimize the heterogeneous expression of Glut-1 (27). Fourth, a different tumor type was studied in our work (cervical cancer) compared with that of others (lung and pancreatic cancer). Compared with the results of Glut-1 expression, our data showed that the SUV was higher in cervical cancer than those in lung cancer (Figs. 4 and 5). One possible reason is that the role of HK is more significant in reflecting glucose metabolism in cervical cancer than in lung cancer. Fifth, it is possible that Glut-1 is a potential ubiquitous important player in 18F-FDG uptake due to the overexpression of Glut-1 as a common phenomenon in many kinds of cancer cells. Therefore, a similarity exists between lung cancer and cervical cancer, examined by different observers and different groups, and can be expected. Actually, our data are closer to the data of Higashi et al. but are a little far away from the data of Brown et al. In addition to different cancer types, we believe that differences in laboratory conditions (room temperature, a well-experienced researcher, concentration of anti-Glut-1 antibody, and so forth) can cause different results in an immunohistochemical study.
It should be noted that this study has some limitations. First, the immunohistochemical expression of other subtypes of glucose transporters (Glut-2 to Glut-10, inclusive) was not studied, but Glut-1 has been indicated as the most common subtype and is overexpressed in cervical cancer (18,26). Next, our study focused on the expression of Glut-1. In fact, HK—in particular, hexokinase II—is another of the key glucose metabolism regulators in cancer cells (10,28). In this study, the distribution of Glut-1 versus SUV was clearly shifted to the right (Figs. 4 and 5). In conjunction with this and our previous studies, which indicated the significance of delayed PET images in identifying cervical cancer lesions (16,20,21), the importance of HK in reflecting glucose metabolism may be more obvious in cervical cancer than in lung cancer. In addition to intracellular HK activity, which is responsible for cellular 18F-FDG uptake, in vitro studies showed that phosphorylating activity in the mitochondria plays a more important role in determining how much 18F-FDG is retained by cells (29). Thus, there may be differences among cancers derived from different tissues in terms of how 18F-FDG is taken up and, perhaps, how their cells control glucose metabolism. The third limitation is that the dephosphorylating activity in the mitochondria, determined by G-6-Pase activity, was not measured in this study. Although in some studies, the lack of G-6-Pase in tumors might play a role in 18F-FDG retention in an animal model, the relationship between 18F-FDG retention and the diminished rate of dephosphorylation is not fully understood (30). In this study, the SUV1 and SUV2 are strongly associated (r = 0.832 for primary tumor and r = 0.973 for recurrent or persistent tumor) (Fig. 2). This implies that Glut-1 in not the only indicator for 18F-FDG uptake in cervical cancer. Increased HK enzyme activity, or even underexpression of G-6-Pase, may be closely involved in the 18F-FDG uptake of various cervical cancer tissues. The fourth limitation is the wide inhomogeneity of positive staining within tumors. Although 3 immunohistochemical staining studies for each specimen were done and the highest score was chosen in this study, some bias may have persisted.
In this study, we found that Glut-1 expression was not present or only weakly expressed (15%) in all normal cervical and CIN tissue. In 94.1% of our cervical cancer specimens, there were higher degrees of Glut-1 expression. Therefore, Glut-1 may play an important role in the glycolytic pathway in cervical cancer. In addition, our data show a close correlation between the immunoreactivity of Glut-1 and 18F-FDG uptake in cervical cancer (Fig. 3). We thus hypothesize that the mechanism of 18F-FDG uptake in cervical cancer cells may be due to overexpression of Glut-1 in these cells. In our study, the analysis of the association between Glut-1 expression and clinicopathologic characteristics showed that neither tumor grade nor tumor stage correlates with Glut-1 expression (Table 1). These results differ from those of previously published data for other tumors (31–33), but they are compatible with the results of Avril et al. for breast cancer (34). Theoretically, the more aggressive the tumor behavior, the more glucose is required for the increased growth. However, some less-differentiated cervical cancer tumors exhibiting higher 18F-FDG uptake were also observed in our studies. This study also shows that Glut-1 expression is lower in poorly differentiated or recurrent cervical cancer than in moderately differentiated cancer. When SUV is also considered, this suggests that measurement of 18F-FDG uptake will not result in a direct assessment of the pathologic grade of the lesion in individual cervical cancer patients. Increased glucose metabolism in cancer cells was found to be related to oncogene activation, the loss of tumor-suppressor genes, hypoxic conditions, and angiogenesis (35). Also, recent molecular studies suggest that cellular energy metabolism is affected predominantly by the expression of transcription factors that regulate genes encoding metabolic enzymes after the development of malignancy (36). Thus, the microenvironment of tumors may play an important role for the biologic behavior of cancer cells, including size and histopathologic grading. In addition, our results also clearly demonstrated that the main lesions had higher Glut-1 expression and higher SUV1, whereas lymph nodes had lower Glut-1 expression and lower SUV1. Our previous studies showed that delayed PET scanning is most valuable in detecting lymph node metastases (16,20,21), which may imply that the enzyme activity of HK is higher in metastatic lymph nodes than in primary cervical tumor. It is possible that Glut-1 expression may reflect a more important role than HK for 18F-FDG accumulation in the main cervical tumor.
Our results lead to the following hypotheses. Glut-1 overexpression in cervical cancer plays the main role in both its increased glucose uptake and energy utilization. Second, the high 18F-FDG uptake in cervical cancer cells may occur through the mechanism of overexpression of Glut-1. Third, the levels of Glut-1 overexpression cannot fully explain the biologic behavior of cervical cancer. Further investigations should evaluate the contributions of the enzyme activities of HK and G-6-Pase and tumor hypoxia in cervical cancer. We plan to monitor the response to therapy, follow-up, and in particular, to determine the survival outcome of patients in whom these evaluations have been performed.
CONCLUSION
In this prospective study, Glut-1 expression was found to be related to 18F-FDG uptake in cervical cancer. Our study also showed that there is zero or low Glut-1 expression in normal cervical and CIN cells. The degree of histopathologic differentiation of SCCC and the result of Glut-1 determination from immunohistochemical staining did not explain the variation of 18F-FDG uptake. Although there is no clear correlation between the degree of histopathologic differentiation of SCCC, Glut-1 levels, and 18F-FDG uptake, there is significantly higher Glut-1 expression in the recurrent or persistent SCCC tumor than in metastatic deposits. We thus hypothesize the following. First, Glut-1 overexpression in cervical cancer plays the main role in both its increased glucose uptake when evaluated with SUV1 and utilization of energy. Second, Glut-1 is important but is not the only indicator for 18F-FDG uptake in cervical cancer. HK enzyme activity may also play a role in reflecting glucose metabolism in cervical cancer. Third, since overexpression of Glut-1 has been proven in many kinds of cancer cells, including cervical cancer, Glut-1 may be a potentially ubiquitous player in 18F-FDG uptake in various malignancies. Further investigations should be performed using these compounds, including evaluation of the enzyme activities of HK and G-6-Pase and tumor hypoxia of these cervical cancer specimens. Our group will also monitor the response to therapy and follow-up the outcome survival of these patients.
Acknowledgments
We thank Wei-Ju Chen for her contribution to this work. This research was supported by grant NSC 91-2314-B-182A-163 from the National Science Council of Taiwan and grant CTRP016 from the Chang Gung Memorial Hospital and University.
Footnotes
Received Apr. 17, 2003; revision accepted Sep. 25, 2003.
For correspondence or reprints contact: Swei Hsueh, MD, Department of Pathology, Chang Gung Memorial Hospital at Taipei, 199, Tung Hwa North Rd., Taipei 105, Taiwan.
E-mail: swei{at}adm.cgmh.org.tw
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Warburg effect: 80 years on
- A Continuously Infused Microfluidic Radioassay System for the Characterization of Cellular Pharmacokinetics
- Oncologic Imaging in Gynecologic Malignancies
- Microregional Expression of Glucose Transporter-1 and Oxygenation Status: Lack of Correlation in Locally Advanced Cervical Cancers