


Abstract
Several PET studies have been performed on conscious nonhuman primates to examine brain function. However, it is unclear how anxiety or stress during PET measurements influences brain function. In the present study, we examined the effects of a well-known anxiety-provoking agent, m-chlorophenyl-piperazine (mCPP), on regional cerebral blood flow (rCBF) and the regional cerebral metabolic rate of glucose (rCMRglc) using PET on conscious rhesus monkeys. Methods: Male rhesus monkeys with experience undergoing PET measurements were used. Twenty and 40 min after mCPP injection (0.2, 1.0, or 5.0 mg/kg intramuscularly; n = 5), rCBF and rCMRglc were measured using an intravenous injection of 15O-H2O and 18F-FDG, respectively. Physiologic parameters, plasma cortisol, and prolactin levels were monitored during PET measurements. Results: Treatment with mCPP significantly increased rCBF in both the cingulate cortex and striatum in a dose-dependent manner, and bell-shaped reductions in rCMRglc were observed for all regions examined. mCPP also significantly increased plasma cortisol and prolactin levels. Physiologic parameters were not affected by mCPP treatment. Conclusion: The present study demonstrates that treatment with the anxiety-provoking agent mCPP significantly affects rCBF and rCMRglc in conscious monkeys. Therefore, since the increases in hormone levels demonstrate that mCPP treatment produced anxiety or stress, these results suggest that anxiety or stress influences conscious brain function. Furthermore, the present study suggests that prevention of anxiety or stress is important when measuring conscious brain function in monkeys.
PET studies on nonhuman primates are useful for understanding brain function and for developing novel therapeutic agents (1–5). Furthermore, because anesthetics affect the binding of several PET tracers, studies using conscious animals are particularly useful (4,5). We have carefully controlled stress in our own work with conscious animals (1–3), although PET studies investigating how stress or anxiety influence brain function in nonhuman primates are rare.
Pharmacologic induction of stress and anxiety provides a reproducible and convenient method for measuring stress-induced changes in brain function. A 5-hydroxytryptamine (5-HT) receptor agonist and antagonist, m-chlorophenyl-piperazine (mCPP) (6–8), is a commonly used anxiety-provoking agent. This compound is a major metabolite of trazodone (9), an atypical antidepressant drug, and produces anxiety in both healthy volunteers and patients (10–13). mCPP is also anxiogenic in several rodent models (14–16). mCPP is considered to produce anxiety through 5-HT2C receptor activation, because it has a partial agonistic property for the 5-HT2C receptor with the highest affinity (affinity values, −log mol/L [pKD] = 7.68) (6). Therefore, several mCPP-induced anxiety models in rodents are often used for screening of therapeutic agents (14,15), and novel 5-HT2C receptor antagonists with anxiolytic properties have been discovered (17–19).
Therefore, to determine how stress or anxiety affects brain function, we examined the effect of mCPP on regional cerebral blood flow (rCBF) and the regional cerebral metabolic rate of glucose (rCMRglc) using PET on conscious rhesus monkeys.
MATERIALS AND METHODS
Animals
Studies were performed on 5 male rhesus monkeys (Macaca mulatta) weighing 7.04–7.60 kg (6–7 y old). All experiments were performed in accordance with the institutional guidelines of the Medical and Pharmacologic Research Center Foundation. T1-weighted MR images of monkeys were obtained on an MRT-50A/II scanner (Toshiba) with a magnetic field strength of 0.5 T. The skull of each monkey was chronically attached to an acrylic plate head-holder, used to fix the head to a monkey chair during PET scans (1,3). The animal was allowed to recover from the procedure for more than 1 mo. The monkeys had been previously acclimatized to chair restraint during repeated training sessions several times a week, starting more than 1 mo before the initiation of the PET study.
PET Experiment
PET scans were obtained with a high-resolution animal PET scanner (SHR-7700; Hamamatsu Photonics K.K.), with a transaxial resolution of 2.6 mm in full width at half maximum in the center of the scan field and a center-to-center distance of 3.6 mm (20). A 68Ga–68Ge-blank scan (120 min) was obtained before each study. Monkeys were transiently anesthetized with about 2% sevoflurane in a N2O and O2 gas mixture (N2O:O2 = 7:3) during catheterization of the left femoral artery for measuring mean arterial blood pressure, heart rate, and arterial blood sampling and during catheterization of the saphenous vein for administration of tracers. After catheterization, anesthesia was immediately discontinued. For the PET scans, each monkey’s head was fixed to a monkey chair with a head-holder and stereotactically aligned parallel to the orbitomeatal plane with a laser marker, and then 68Ga–68Ge transmission scanning (30 min) was performed. From the start of each transmission scan, mean arterial blood pressure and heart rate were continuously monitored with a life monitoring system (Nihon Kohden). About 1 h after discontinuance of anesthesia, the partial pressure of carbon dioxide (pCO2), partial pressure of oxygen (pO2), and pH of arterial blood were measured (ABL615; Radiometer) to confirm the physiologic condition of the monkey. PET emission scanning was performed in dimmed light with the monkey’s ears unplugged and eyes open.
mCPP was purchased from Sigma and dissolved in sterilized saline. mCPP (0.2, 1.0, or 5.0 mg/kg; n = 5 for each dose) was intramuscularly administered (0.25 mL/kg) 20 min before rCBF measurement. The experimental protocol was crossover designed, with each monkey receiving 3 doses of mCPP with at least 3 wk of washout.
Twenty minutes after intramuscular administration of mCPP, 15O-H2O (1 GBq in 2 mL saline) was injected intravenously for rCBF measurement. A 2-min emission scan consisting of 12 frames was obtained after injection of 15O-H2O. During that period, 24 timed arterial blood samples (0.2 mL) were withdrawn from a catheter placed in the femoral artery for measurement of arterial radioactivity using an automated well γ-counter (1480 Wizard; Wallac Oy). Because of the very short half-life of 15O (2.037 min), the radioactivity rapidly decayed after the 15O-H2O study. Therefore, 40 min after mCPP administration, 18F-FDG (370 MBq in 2 mL of saline) was injected intravenously for the rCMRglc measurement. A 60-min emission scan consisting of 22 frames was obtained after injection of 18F-FDG. During that period, 17 timed arterial blood samples (0.2 mL) were withdrawn for arterial radioactivity measurements. The blood samples obtained at 45 and 60 min after injection were also analyzed for blood glucose levels (ABL615).
To measure plasma cortisol and prolactin levels, arterial blood samples were collected before mCPP treatment and at 20, 40, 70, and 100 min after mCPP treatment. A plasma fraction for each arterial sample was prepared. Cortisol and prolactin levels were analyzed using mini-VIDAS assay kits (bioMerieux Vitek, Inc.).
Data Analysis
rCBF images were generated in accordance with an autoradiographic method (21–23). PET images from 0 to 60 s after the 15O-H2O injection and an arterial input function were used for calculation of rCBF images. A partition coefficient of 0.7, derived from preliminary kinetic analysis in monkeys (data not shown), was used. rCMRglc images were generated in accordance with an autoradiographic method with an operational equation derived by Sokoloff et al. (24) and modified by Phelps et al. (25). The parameters derived by Reivich et al. (26) were used for this calculation. PET images from 40 to 60 min after injection of 18F-FDG were used for calculation of rCMRglc images. All PET images and MR images were anatomically standardized using 3-dimensional stereotactic surface projection (NEUROSTAT) for monkeys (27). Regions of interest were taken for the cingulate, frontal, parietal, temporal, and occipital cortices; the striatum; the thalamus; and the cerebellum after anatomic standardization.
All data are represented as the mean ± SD. Statistical analysis was performed using repeated-measures ANOVA followed by post hoc Dunnett multiple comparison, and our laboratory standard data for conscious monkeys (n = 14) were used as the control group. A probability value of less than 0.05 was considered significant.
RESULTS
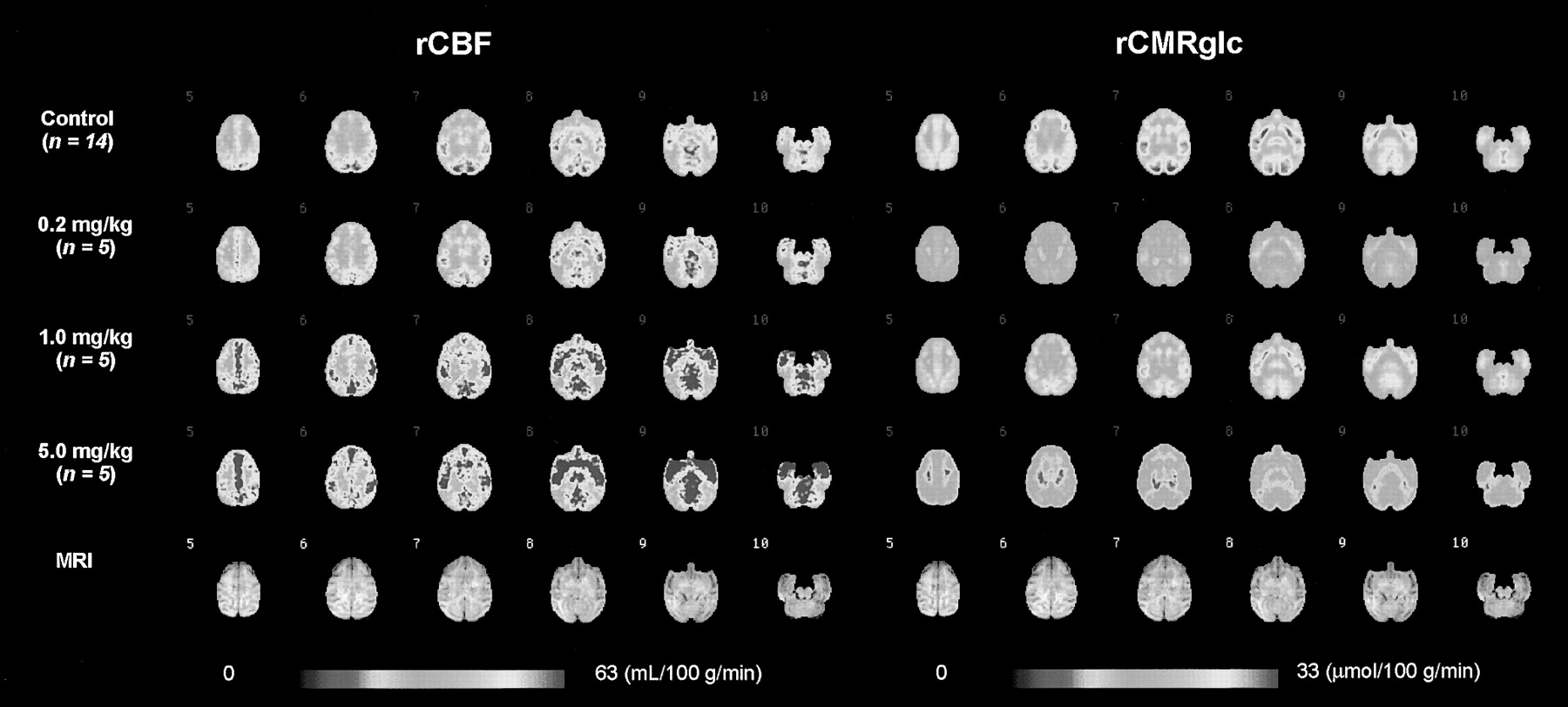
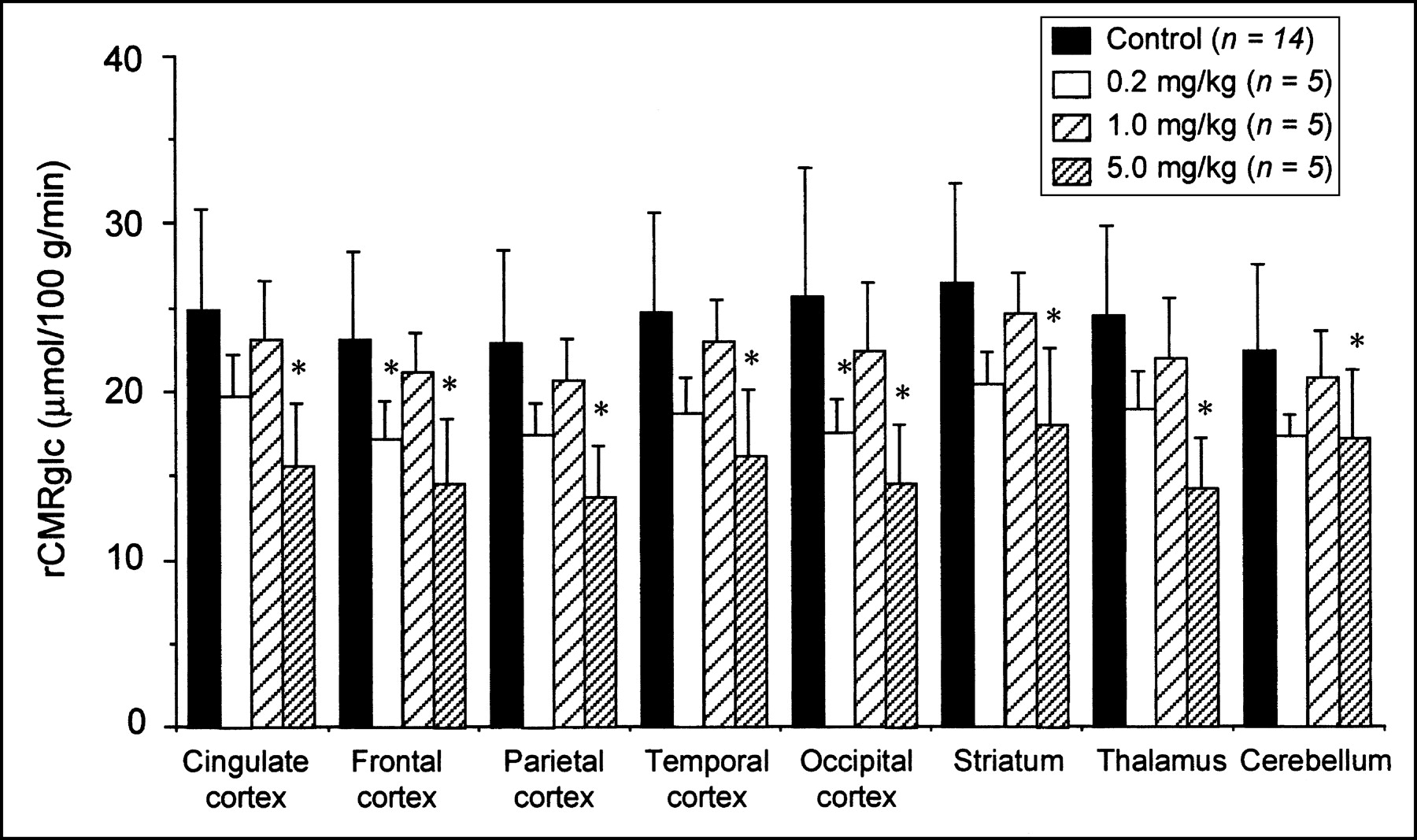
The mean rCBF and rCMRglc images and mCPP-treated groups are shown in Figure 1. The rCBF (Fig. 2) and rCMRglc (Fig. 3) values are shown for the cingulate, frontal, parietal, temporal, and occipital cortices; the striatum; the thalamus; and the cerebellum. Treatment with mCPP increased rCBF (F3,7 = 30.614, P < 0.0001), and a significant increase after treatment with 5.0 mg/kg was observed in the cingulate cortex and striatum (Fig. 2). mCPP significantly affected rCMRglc (F3,7 = 27.926, P < 0.0001). Treatment with 0.2 mg/kg decreased rCMRglc in all brain regions examined, and a significant decrease was observed in the frontal and occipital cortices. Treatment with 1.0 mg/kg did not change rCMRglc. A significant reduction in rCMRglc after treatment with 5.0 mg/kg was observed in all brain regions examined (Fig. 3).

Mean rCBF and rCMRglc images in control group and in groups treated with 0.2, 1.0, and 5.0 mg/kg mCPP and corresponding MR image.
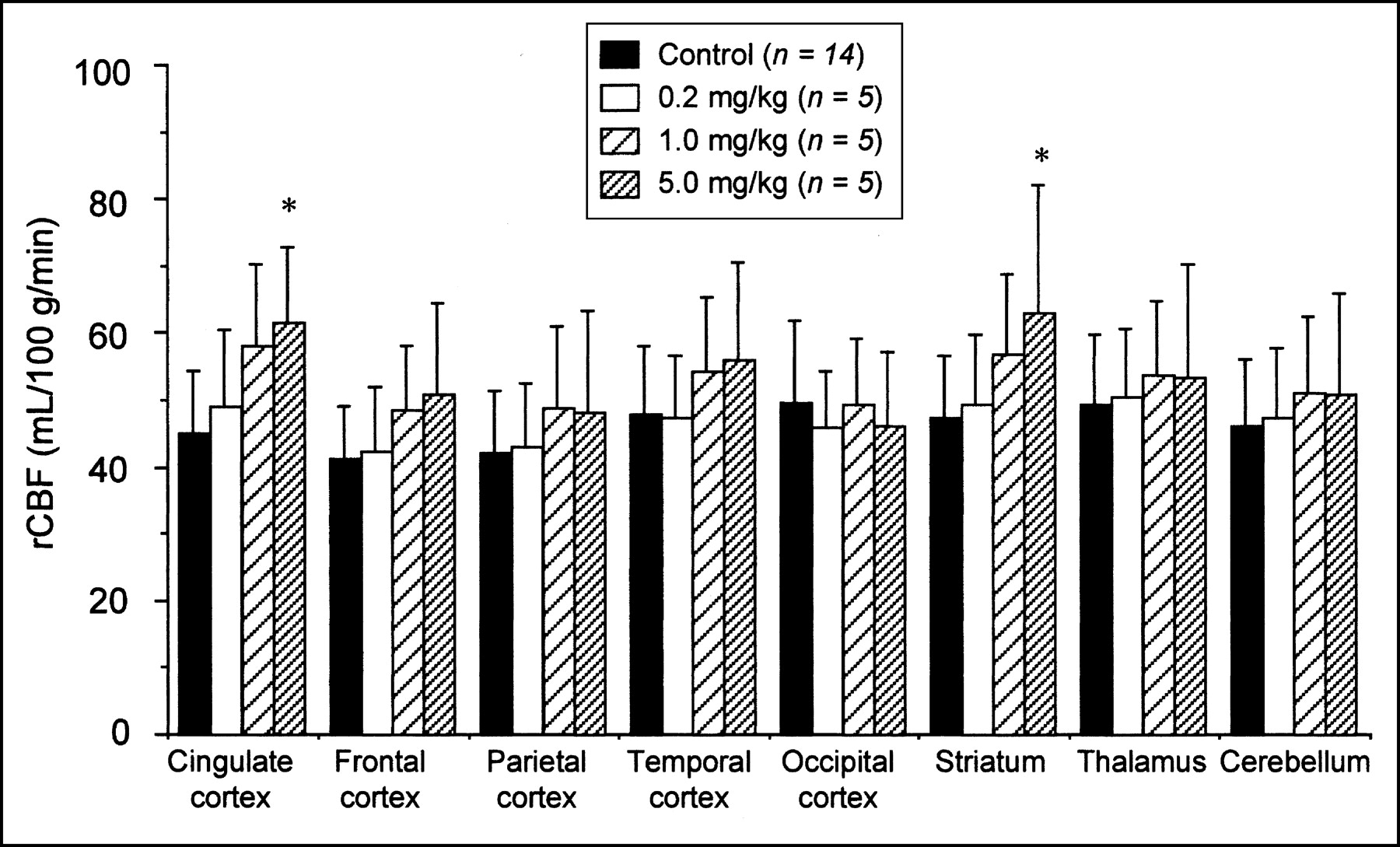
rCBF changes after mCPP treatment of conscious rhesus monkeys. Control group data are standard data from our laboratory. Each column represents mean, and bars indicate SD. *P < 0.05 versus control group.
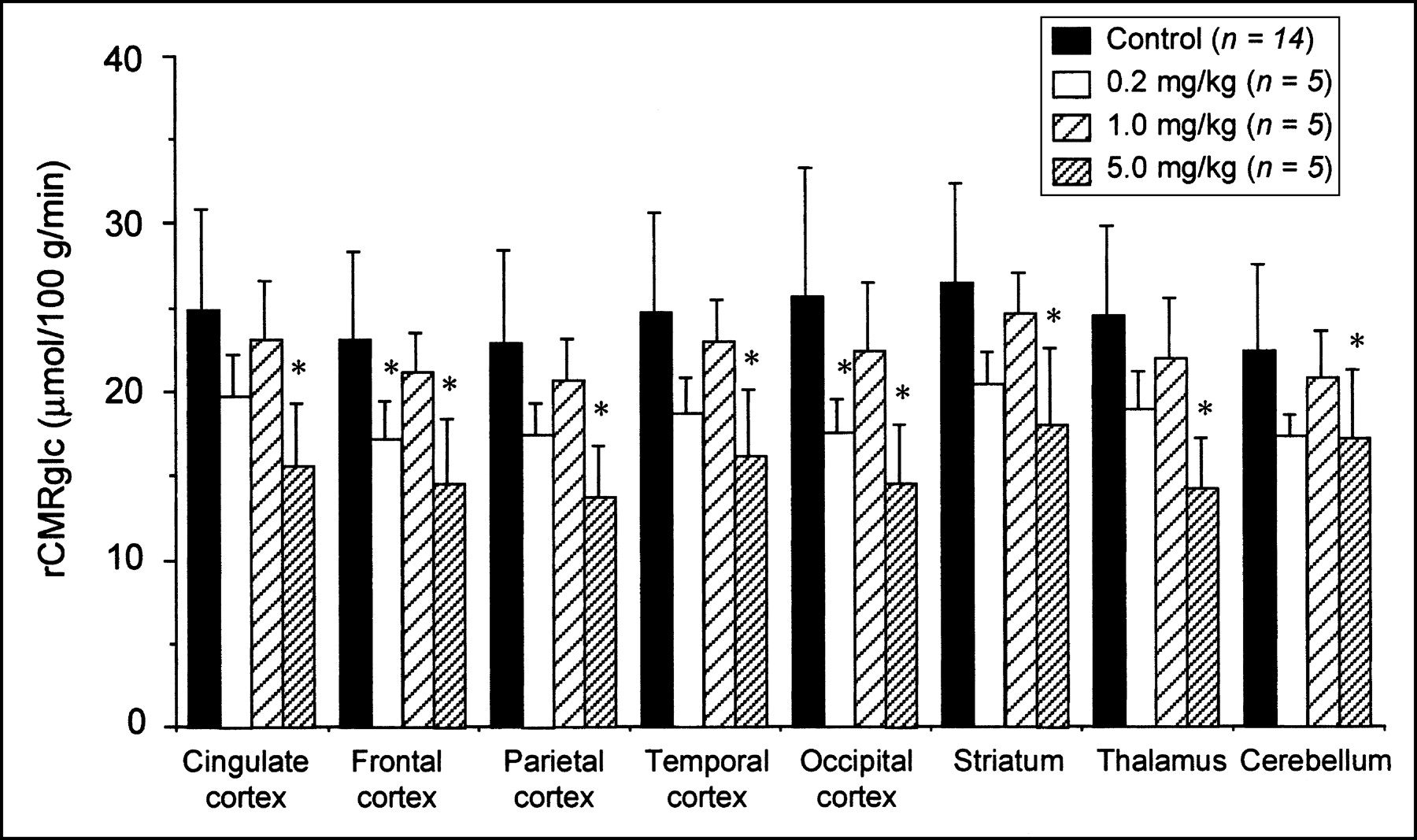
Changes in rCMRglc after mCPP treatment of conscious rhesus monkeys. Control group data are standard data from our laboratory. Each column represents mean, and bars indicate SD. *P < 0.05 versus control group.
Plasma cortisol levels were significantly increased by mCPP treatment. A marked increase was observed in the group treated with 1.0 mg/kg of mCPP (Fig. 4A). A transient and significant increase in prolactin levels in plasma was observed in the groups treated with 1.0 and 5.0 mg/kg of mCPP (Fig. 4B).
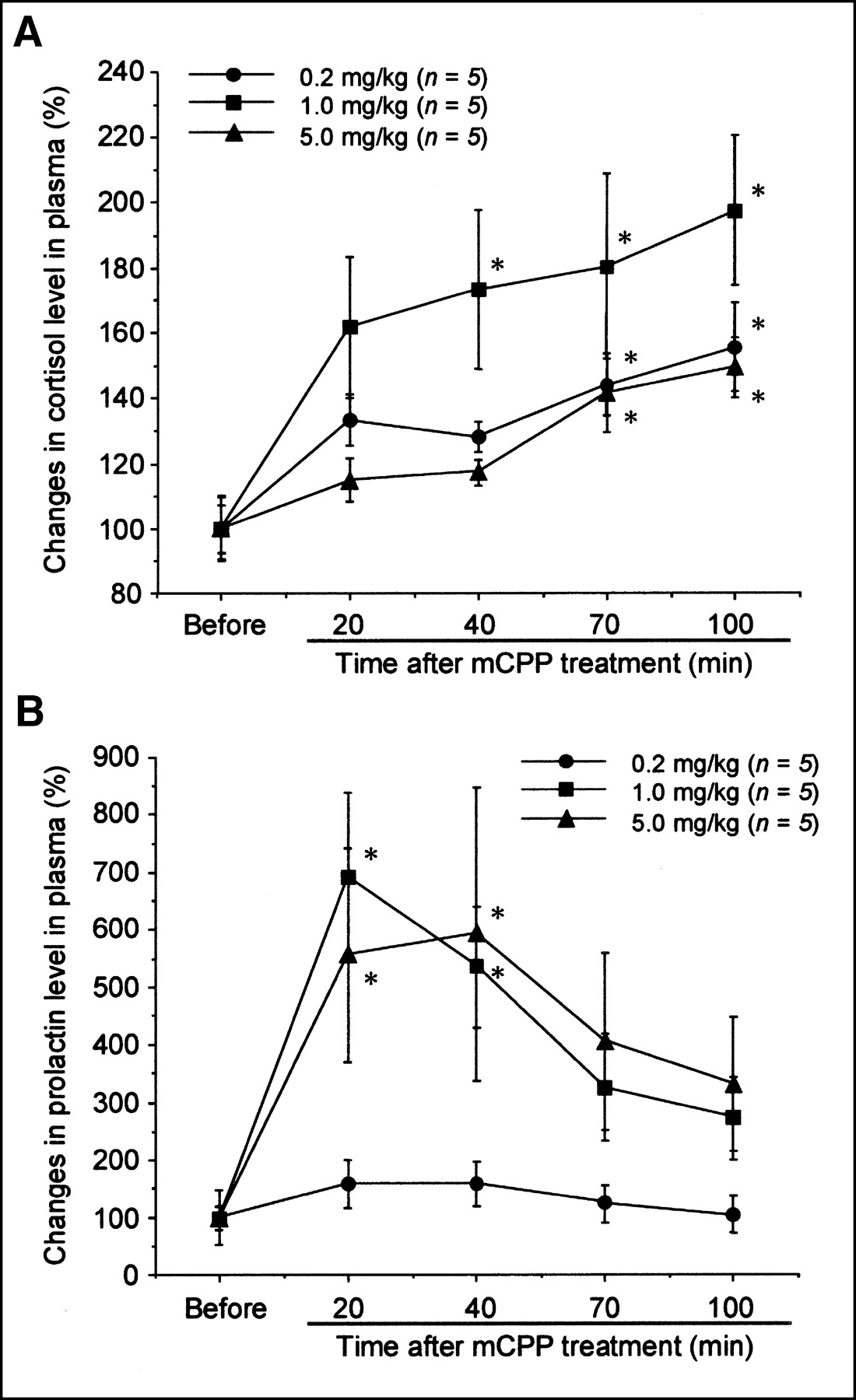
Changes in plasma cortisol (A) and prolactin level (B) after mCPP treatment of conscious rhesus monkeys. Each symbol represents mean, and bars indicate SD. *P < 0.05 versus plasma cortisol and prolactin levels before mCPP treatment.
Physiologic parameters after mCPP treatment remained within the normal range (Table 1). When 5.0 mg/kg of mCPP was used, all animals became sedated and somnolent.
Physiologic Parameters After mCPP Treatments in Conscious Rhesus Monkeys
DISCUSSION
In the present study, we demonstrated that rCBF and rCMRglc change after treatment with an anxiety-provoking agent, mCPP, in conscious rhesus monkeys. mCPP significantly increased plasma cortisol and prolactin levels, as reported for rhesus monkeys (28) and humans (8,10,11,29–31). The present treatment (0.2–5.0 mg/kg) was administered intramuscularly 20 min before rCBF measurement. Aloi et al. (28) reported that intravenous treatment with mCPP (0.5–3.0 mg/kg) significantly increased plasma cortisol and prolactin levels in monkeys 20 min after treatment. We used intramuscular administration of mCPP to maintain stable plasma concentrations long enough to determine both rCBF and rCMRglc. Furthermore, the correlation between mCPP-induced cortisol release and clinical anxiety levels confirms that our treatment paradigms mimic anxiety and stress (30).
For 2 reasons, we conclude that the increase in cortisol resulted from mCPP administration and not from stress PET measurements. First, the animals had been sufficiently acclimated to the PET apparatus. Animals were used for the study only when plasma cortisol did not increase after a 2-h training period. Second, in the control group, the plasma cortisol level after sequential rCBF and rCMRglc measurements (about 80 min after rCBF measurement) was 425.2 ± 40.5 ng/mL. This level was not significantly different from the initial absolute value in the mCPP-treated group (0.2 mg/kg: 372.4 ± 40.5 ng/mL; 1.0 mg/kg: 398.9 ± 63.4 ng/mL; 5.0 mg/kg: 365.5 ± 67.4 ng/mL). However, because there were individual differences in plasma cortisol levels, we showed changes of cortisol level as a percentage increase compared with baseline.
mCPP treatment significantly increased rCBF in the cingulate cortex and the striatum in a dose-dependent manner. A low dose of mCPP significantly decreased rCMRglc in the frontal and occipital cortex, and a high dose significantly decreased rCMRglc in all brain regions examined. These changes did not depend on physiologic parameters, which were unchanged by mCPP treatment. mCPP produced sedation and somnolence at the highest dose, which might reduce anxiety. At this dose, plasma prolactin was significantly and almost maximally increased, and plasma cortisol was significantly increased, although not to the same extent as in the 1.0 mg/kg group. Recent clinical studies have shown that mCPP-induced increases in plasma cortisol directly correlated with clinical measures of anxiety (30), whereas prolactin changes did not (11), and that this effect could be blocked by a 5-HT2 receptor antagonist (28). Thus, changes in plasma cortisol level are linked to the anxiogenic effects of mCPP, whereas plasma prolactin level is linked to direct central 5-HT receptor activation by mCPP. Therefore, a dose of 5.0 mg/kg with mCPP might be too high for anxiety induction in rhesus monkeys. The rCMRglc reduction after 5.0 mg/kg of mCPP leads to a decline in brain function, with sedation and somnolence. At the same dose, mCPP increased rCBF. mCPP has been reported to increase cerebral blood flow in limbic and motor regions (32). Therefore, the rCBF increase at 5.0 mg/kg was due to the effects of mCPP on rCBF rather than due to anxiety.
At 0.2 or 1.0 mg/kg, mCPP increased plasma cortisol and prolactin levels in a dose-dependent manner. In these treatments, rCBF tended to increase or did not change, whereas rCMRglc was significantly reduced at 0.2 mg/kg but did not change at 1.0 mg/kg. These changes agree with previous results from rat studies showing that rCMRglc decreased with low-dose treatment with mCPP and increased with high-dose treatment (33–36). In human studies, rCMRglc decreased with anxiety and CBF paralleled the level of anxiety: Increases in CBF correlated positively with level of anxiety in low-anxiety patients but correlated negatively with level of anxiety in high-anxiety patients (37). These results may suggest a disconnection between rCBF and rCMRglc in anxious patients. The present study also demonstrated a similar phenomenon. The reasons were not clear, but this disconnection between rCBF and rCMRglc may be an important index in diagnosis using PET measurements.
In the present study, rCBF measurement was performed 20 min after mCPP treatment, and at that time plasma cortisol level was increased, but not significantly. However, rCBF was significantly increased in some brain regions. Charney et al. (13) reported that the peak of mCPP-induced anxiety occurred 30 min after the drug was administered, whereas peak plasma cortisol occurred 45–60 min after the challenge, regardless of whether panic-disorder patients or healthy subjects were tested. These results and those of the present study suggest that the psychologic effects of mCPP occur before its physiologic effects. It is tempting to speculate that if rCBF measurements had been performed later, more substantial rCBF changes might have been observed. The present sequential measurement limited the present study. Another limitation was that a behavioral study after mCPP treatment could not be performed during PET measurements. Therefore, the present results for rCBF and rCMRglc changes after mCPP treatment could not be specifically correlated with anxiety or stress.
CONCLUSION
The present PET studies using conscious monkeys demonstrated that treatment with an anxiety-provoking agent, mCPP, significantly affected rCBF and rCMRglc. An increase in hormonal parameters suggested that the treatment produced anxiety or stress. We demonstrated that mCPP-induced anxiety or stress significantly influenced rCBF and rCMRglc, strongly suggesting that prevention of anxiety or stress is important when measuring conscious brain function.
Acknowledgments
We thank Akeo Kurumaji, MD, PhD (Tokyo Medical and Dental University School of Medicine) for helpful discussions. We also thank Shigeo Hayashi for operation of the cyclotron.
Footnotes
Received Jan. 21, 2003; revision accepted May 1, 2003.
For correspondence or reprints contact: Hiroyuki Takamatsu, PhD, Medical and Pharmacological Research Center Foundation, Wo32, Inoyama-Town, Hakui-City, Ishikawa, 925-0613, Japan.
E-mail: takamatsu{at}mprcf.or.jp




{kind=link}
{kind=link}
{kind=link}
{kind=link}