


Abstract
Basal ganglia or thalamic activation has been reported in ictal SPECT studies of patients with intractable epilepsy. We hypothesized that lateralization of activation of these subcortical structures may aid in the lateralization of seizure foci in patients in whom the cortical focus is subtle or equivocal. Methods: This was a retrospective analysis of 72 ictal 99mTc-ethylcysteinate dimer SPECT studies in 43 patients with intractable epilepsy in whom seizure laterality could be eventually determined. All patients underwent video-electroencephalography (EEG) monitoring, MRI, and one or more ictal SPECT scans as well as an interictal SPECT scan. Intracranial electrode EEG monitoring and surgery were performed as clinically indicated. Ictal and interictal studies were coregistered with patients’ MRI scans using automated software, and ictal minus interictal subtraction images were obtained. The presence of asymmetric basal ganglia or thalamic activation was determined by 2 experienced observers who were unaware of clinical information. The final seizure focus was determined by surgical cure in 37 patients. In patients in whom surgery was not indicated or initial surgery was performed at another institution (n = 6), a consistent focus detected by intracranial electrode monitoring or repeated stereotypical seizures all originating from the same site on video-surface EEG monitoring was considered to indicate the final seizure focus. Results: Thirty-five patients had neocortical seizures and 8 had mesial temporal lobe seizures. Asymmetric basal ganglia activation was seen in 22 (30.6%) studies. This activation was ipsilateral to the final determined seizure focus in 17 of 22 of these studies (77.3%) and contralateral in 5 of 22 (21.7%). Asymmetric thalamic activation was seen in 15 studies (20.8%), of which 12 of 15 (80%) were ipsilateral to the final seizure focus, whereas 3 of 15 (20%) were contralateral. In 3 of 5 studies with contralateral basal ganglia activation and 1 of 3 studies with contralateral thalamic activation, the SPECT study as a whole was found to be falsely localizing. In another 2 cases of contralateral subcortical activation, the SPECT study as a whole was considered nonlocalizing. Worse outcome was not observed in patients with false ictal SPECT subcortical lateralization; however, the presence of asymmetric subcortical uptake, regardless of relationship to seizure focus, was associated with decreased incidence of seizures at 1 y after surgery. Conclusion: Although asymmetric basal ganglia or thalamic activation is common, it is rarely the sole indicator of seizure localization. However, it may be a useful confirmatory sign in subtle cases of cortical localization. In cases of false ictal SPECT subcortical lateralization, the basal ganglia appear to follow cortical activation pattern. Furthermore, there appears to be a correlation between lateralizing uptake in subcortical structures on ictal SPECT and postsurgical outcome in intractable epilepsy patients.
In intractable epilepsies, the accurate localization of the seizure focus before surgery is vital to increase the chances of surgical success (1,2). This becomes especially challenging in patients without structural lesions identified on MRI (1,3,4). Ictal SPECT studies have been used to improve the localization of foci in medically intractable epilepsy in conjunction with clinical evaluation, electroencephalography (EEG), and other imaging methods. The sensitivity of ictal SPECT studies for the seizure focus ranges from 89% to 97% in patients with temporal lobe epilepsy (TLE) (5–8) and from 73% to 92% in patients with neocortical epilepsy (4,8,9). Modifications in SPECT image-processing techniques, including ictal-interictal image subtraction and coregistration with MRI, have been introduced to improve the diagnostic yield (10–12).
Hyperperfusion of the basal ganglia and thalamus has been incidentally identified in several ictal SPECT studies (13–17). Only Shin et al. (18) and Newton et al. (19) studied subcortical activation on ictal SPECT systematically, with Shin et al. focusing on the relationship between basal ganglia and cerebellar hyperperfusion and Newton et al. focusing on the relationship of basal ganglia activation to dystonic posturing. Most of the ictal SPECT studies report subcortical activation ipsilateral to the cortical focus, whereas functional studies of the interictal state show ipsilateral subcortical hypometabolism on PET (20,21) and ipsilateral subcortical hypoperfusion on interictal SPECT images (22). In addition, anatomic and functional studies in animal epilepsy models have pointed to the basal ganglia and thalamus as regions important in the regulation of seizure propagation (23–25). We hypothesized that lateralization of basal ganglia or thalamic activation in ictal SPECT studies is not random and can be used as a supplementary finding in the localization of seizure foci on SPECT images of intractable epilepsy patients with subtle or equivocal cortical activation. To our knowledge, this is the first study analyzing the potential diagnostic usefulness of lateralizing uptake in basal ganglia and thalamus in ictal SPECT studies.
MATERIALS AND METHODS
Patients and Ictal Injections
From April 1994 to April 1999, 70 seizure patients undergoing presurgical evaluation at Dartmouth-Hitchcock Medical Center underwent at least 1 ictal brain SPECT study, at least 1 interictal brain SPECT study, as well as an MRI study that included a 3-dimensional (3D) spoiled gradient echo (SPGR) coronal sequence. This included patients with neocortical seizures in whom the focus had not been previous identified and any patients with TLE in whom lateralization was in doubt. These data were used as part of the clinical management of these patients. Approval from the Institutional Review Board at Dartmouth-Hitchcock Medical Center was obtained to review patient medical records and to perform the image registration and subtraction.
Patients were entered into this study if the data were available for all 3 studies (ictal SPECT, interictal SPECT, and MRI); the tracer used was 99mTc-ethylcysteinate dimer (ECD); and a unilateral focus or foci were identified by either intracranial EEG monitoring, repetitive congruent video-EEG monitoring, or results of surgical resection with at least 1 y of clinical follow-up. The ictal injections were performed on the epilepsy-monitoring unit during the patient’s inpatient noninvasive evaluation, which included video-EEG monitoring with scalp EEG electrodes. On the days when ictal SPECT was to be attempted (usually after antiseizure medication withdrawal and sometimes sleep deprivation), a shielded syringe containing 1,110 MBq (30 mCi) 99mTc ECD was brought to the unit and kept by the patient’s bedside. A trained member of the staff remained by the patient’s bedside from 8 am to 4 pm. This syringe was recalibrated in the Nuclear Medicine Department every 2 h, resulting in an injected dose of 888–1,110 MBq (24–30 mCi). Radiotracer injection was performed as rapidly as possible after seizure onset that was detected by either clinical signs or EEG changes, whichever came first. The injection time was later calculated through review of the video-EEG. The time in seconds from seizure onset to the midpoint of the injection was taken as the injection time in seconds. Time from injection to scan time was approximately 2–3 h.
SPECT
Patients were transferred to the Nuclear Medicine Department for imaging after stabilization. All scans were acquired on a Prism 3000 triple-head gamma camera (Picker International) using high-resolution collimators. Four 7-min SPECT images were acquired, each of 60 steps of 7 s each using a 128 × 128 matrix. The raw data files were summed before image processing, after confirming lack of patient movement. If movement occurred, files were omitted as appropriate (maximum of 2 files omitted). All studies were reconstructed in a similar manner using a ramp filter, followed by a postprocessing low-pass filter, order 4 with a 0.26 cutoff. Images were reconstructed in 3 planes, with coronal slices of 1 pixel (2.225 mm) used for registration purposes. Several patients had 2 or more ictal studies performed (to confirm findings, due to late injections or because of atypical seizures). The patient’s interictal studies were obtained after an injection on a different day, frequently as an outpatient. The acquisition and reconstruction parameters were identical.
MRI
The MRI studies were acquired on a General Electric Sigma 1.5-T magnet. As part of the routine epilepsy protocol, a 3D SPGR sequence was obtained in the coronal plane (124 × 1.5 mm slices), and this was used for registration purposes.
Image Registration and Subtraction
The General Electric MRI data were exported from the scanner in DICOM (Digital Imaging and Communications in Medicine) format and the SPECT data were exported in the PRISM image format. These files were transferred via the hospital network to a personal computer workstation within the Department of Radiology. The data were displayed, registered, and subtracted using an NT (Microsoft Corp.)-based software package, RVIEW, developed initially at United Medical and Dental Schools Guys Hospital London and further extended at Yale University (New Haven, CT). A fully automated rigid registration algorithm based on the multiresolution optimization of normalized mutual information (26) was used to bring each SPECT image into alignment with the patient’s high-resolution 3D MRI scan. An interactive contour-based display of SPECT tracer uptake on orthogonal MRI brain slices was used to visually confirm acceptable spatial alignment before image subtraction. After spatial alignment, normalization of SPECT counts in the 2 images was performed using an automated iterative normalization algorithm. A SPECT subtraction display was then produced in orthogonal planes using this normalization estimate.
Image Display and Interpretation
Images were retrospectively interpreted by consensus of 2 experienced nuclear medicine physicians who were unaware of clinical information. Images were assessed for the presence and location of suspected seizure foci (“hot spots”) on both the original (ictal and interictal pairs) and the subtracted and registered images. This included determination of basal ganglia and thalamic activation (increased uptake on the ictal relative to the interictal study). Basal ganglia or thalamic activation was recorded as “asymmetric” if either unilateral activation occurred or if visually asymmetric activation was seen either on the ictal images relative to the interictal study or on the subtracted images. All data were entered into an Access 97 (Microsoft Corp.) database at the time of image interpretation.
Clinical Data
Clinical data were obtained on all patients after the blinded retrospective image interpretation either from the hospital chart or from the neurologists concerned with care of the patients. Demographic information and history pertaining to the patient’s seizures were also obtained. The results of routine surface EEG, video-EEG monitoring, and invasive EEG monitoring (including sites of electrode placement) were recorded along with the type and date of any surgical procedures. The “final” seizure focus was identified from these data, where possible. The gold standard was ideally a successful surgical outcome but, because surgery was indicated only in a proportion of the patients (n = 39), other endpoints, such as successful localization of a consistent focus by intracranial electrode monitoring (n = 3) or repeated stereotypical seizures all originating from the same site on video-surface EEG monitoring (n = 1), were believed to be adequate confirmation of final seizure focus. Only those patients’ data for whom adequate clinical and EEG data were available to identify the “true” seizure focus were used to correlate subcortical activation with cortical focus on SPECT studies. When asymmetric subcortical activation occurred, the side of maximal activation was defined as being ipsilateral or contralateral to the final seizure focus. The presence or absence of seizures 1 y after surgery and Engel’s classification (class I, seizure free; class II, almost seizure free; class III, some improvement; class IV, no improvement) (27) at the last follow-up were used as outcome endpoints. Engel’s classification of surgical outcome was correlated with basal ganglia and thalamic uptake only in patients who underwent surgery in our institution (patients who underwent neurosurgery elsewhere were evaluated at our center because of poor postsurgical outcome.)
Data Analysis
Two-sample 2-tailed Student t test (numeric data) and χ2 test (ordinary data) were used for comparison between groups of patients with and without asymmetric subcortical structures with respect to age, sex, handedness, duration since seizure onset, injection time, and final seizure lateralization. The power of ipsilateral subcortical activation achieved by our sample size was calculated using the Fisher exact test for a single proportion. Simple regression and the Spearman rank correlation coefficient did not show any significant effect of the subject on the results of separate SPECT scans with respect to subcortical activation. The Fisher exact test was used to determine the correlation between asymmetric subcortical activation and postsurgical outcome in the 39 patients in whom surgery was indicated. The 95% confidence interval of the risk of persistent seizures was calculated without continuity correction.
RESULTS
Patients
Of the original 70 patients with intractable epilepsy who underwent 113 ictal SPECT studies, 27 patients were excluded because of either uncertain final seizure focus localization or insufficient follow-up after surgery (<1 y follow-up). Forty-three patients (22 male) fulfilled the criteria for study entry with a total of 72 ictal studies. The mean age of seizure onset was 13.5 ± 10.1 y, with a range of 3 mo to 42 y. The mean age of patients at the time of the first ictal SPECT study was 32.8 ± 9.9 y, with a range of 9–59 y. Thirty-nine patients (90.7%) were right-handed, whereas the remaining 4 patients (9.3%) were left-handed. Patients underwent 1–7 ictal studies (mean, 1.7 ictal studies per patient; median, 1) and 1–3 interictal studies (mean, 1.1; median, 1). Thirty-nine patients had surgical resection, 37 of which were performed at our institution. Fourteen of 39 patients (35.9%) continued to have seizures at 1-y follow-up despite appropriate medical management. Using Engel’s outcome classification in the 37 patients who underwent surgery at our institution, at the last follow-up there were 22 patients with class I outcome, 10 with class II, 5 class III. and none with class IV outcome. The 2 patients who had surgery at another institution and were evaluated afterward at our center had class III and class IV outcome. In both of these patients, the final epileptic focus with which lateralization of subcortical structures was compared was determined by repeated video-EEG, intracranial electrode monitoring, and congruent results of cortical uptake on ictal SPECT study.
Basal Ganglia and Thalamus Asymmetry
Table 1 lists the incidence of asymmetric basal ganglia and thalamic activation. The positive predictive value of ipsilateral basal ganglia and thalamus activation for the side of the definitively determined seizure focus in patients with asymmetric subcortical uptake was 77% and 80%, respectively (Figs. 1 and 2). A positive predictive value for basal ganglia or thalamus activation in localizing the side of the seizure focus was 88%. When the 2 studies that had 1 subcortical structure activated ipsilaterally, whereas the other was activated contralaterally, were excluded, the positive predictive value was 80%. Asymmetric subcortical activation occurred in patients with a final seizure focus located in all lobes except the parietal lobe (Table 2).
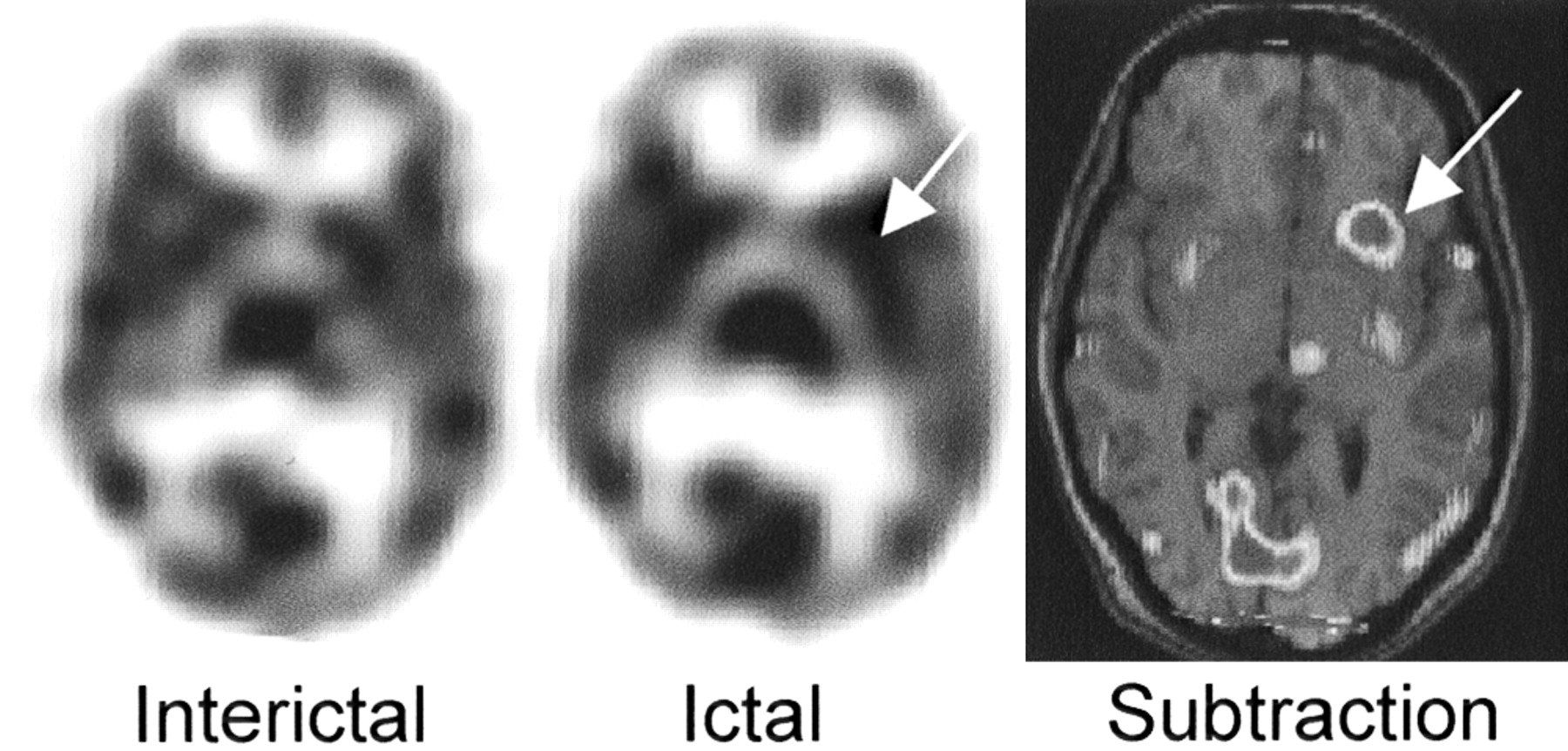
Example of ipsilateral basal ganglia lateralization. Asymmetric basal ganglia activation (left > right) in patient with left frontal focus (not visualized here) seen on transaxial ictal and subtraction SPECT images. Arrows indicate activation of left caudate.

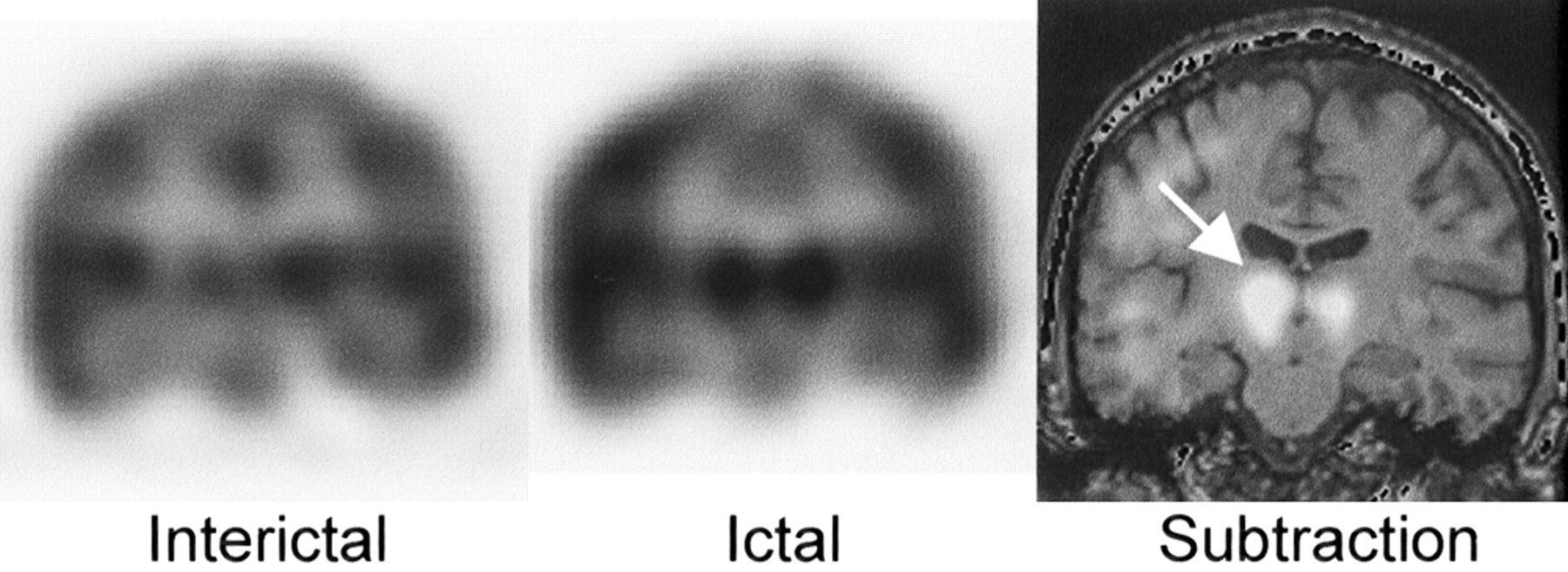
Example of ipsilateral thalamic lateralization. Asymmetric thalamus activation (right > left) in patient with right mesiotemporal focus seen on coronal ictal and subtraction SPECT images. Arrow indicates right thalamic activation.
Studies with Asymmetric Subcortical Activation
Lateralized Subcortical Activation with Respect to Final Localization of Foci on 72 Ictal SPECT Studies
Injection Timings
Injection timings were obtained for 67 of 72 studies (93.1%). Patients were injected at a median of 18.5 ± 13.6 s, with range of 2–80 s. The injection bolus usually took 1–2 s to complete. There was no difference between the injection time in studies with ipsilateral, contralateral, and nonlateralizing subcortical activation for either the basal ganglia or the thalamus (P > 0.05 for thalamus; P > 0.05 for basal ganglia).
Relationship Between Asymmetric Subcortical Structures and Patient Variables
There was no significant difference between the ipsilateral, contralateral, and nonlocalizing groups with respect to age, sex, handedness, number of studies per patient, duration since initial seizure onset, or lateralization of the final seizure focus (P > 0.05 in all instances). A statistically significant decrease in seizure presence at 1-y follow-up was found for patients in whom either thalamic (P = 0.013 all patients; P = 0.009 for subgroup of patients with neocortical epilepsy) or basal ganglia (P = 0.006 for all studies; P = 0.02 for the subgroup of patients with neocortical epilepsy) asymmetric hyperperfusion was identified on any study (Table 3). When Engel’s outcome classification was used as an endpoint, a similar relationship between outcome and subcortical asymmetry was observed (Table 4).
Comparison Between Seizure Frequency in Patients With and Without Asymmetric Subcortical Findings on Any Ictal Study at 1 Year After Surgery Follow-Up
Relationship Between Postsurgical Outcome of Patients Who Underwent Surgery at Our Institution as Determined by Engel’s Classification and Asymmetric Basal Ganglia and Thalamic Uptake on Ictal SPECT Studies
Reproducibility of Asymmetric Findings in Same Patient
Because a relatively large percentage (14/43 [32.6%]) of patients had >1 ictal SPECT study (7 patients had 2 studies, 4 patients had 3 studies, 2 patients had 5 studies, and 1 patient had 7 studies), we were able to examine the reproducibility of asymmetric subcortical activation. Of these 14 patients, only 7 (50%) had the same basal ganglia uptake findings, whereas 10 (71.4%) had the same thalamic uptake findings in all their ictal studies. There was no difference in injection timings between the initial and the subsequent ictal SPECT studies of these patients (P > 0.05). In the subgroup of patients with the same subcortical activation in all ictal studies, the observed pattern was primarily that of no subcortical uptake in both studies (85.7% patients with congruent basal ganglia activation on multiple ictal SPECT studies; 100% patients with congruent thalamic activation on multiple ictal SPECT studies). In patients with different subcortical activation in multiple ictal studies of the same patient (50% patients with multiple ictal studies with respect to basal ganglia activation; 18.6% patients with multiple ictal studies with respect to thalamic activation), the most frequent uptake pattern was activation of basal ganglia or thalamus in 1 ictal study but lack of activation in the other ictal study (or studies). However, there were 2 patients (patients 28 and 35) with basal ganglia uptake in whom 1 ictal SPECT study revealed ipsilateral basal ganglia activation, whereas another SPECT study showed contralateral basal ganglia activation.
Studies with Contralateral Subcortical Activation
In 6 patients (7 studies), the subcortical activation was contralateral to the final seizure focus (1 of these studies had concurrent contralateral basal ganglia and contralateral thalamic activation). These false localizing studies constituted 21.7% of the studies (5/22) with asymmetric basal ganglia activation and 20% of the studies (3/15) with asymmetric thalamic activation.
Potential reasons for contralateral subcortical localization have been identified in 6 of 7 studies. Two patients were injected during isolated auras, whereas another patient’s seizure generalized (Fig. 3). Despite 3 ictal SPECT studies with good injection timings, 1 patient’s focus could not be identified on any ictal SPECT studies, and the subtle uptake in the contralateral basal ganglia has been attributed to the overinterpretation of 1 SPECT study. The ictal SPECT study of an additional patient was false localizing, with the basal ganglia activation following the side of the cortical activation (Fig. 4). Two ictal SPECT studies of the most complex patient in the series contributed 3 false localizing findings (2 thalami, 1 basal ganglia). In 1 ictal SPECT study, the cortical activation as a whole was found to be nonlocalizing with subtle activation of contralateral subcortical structures. The other SPECT study was the only study in which the thalamus activated contralateral to an area of clear (and correct) cortical hyperperfusion.

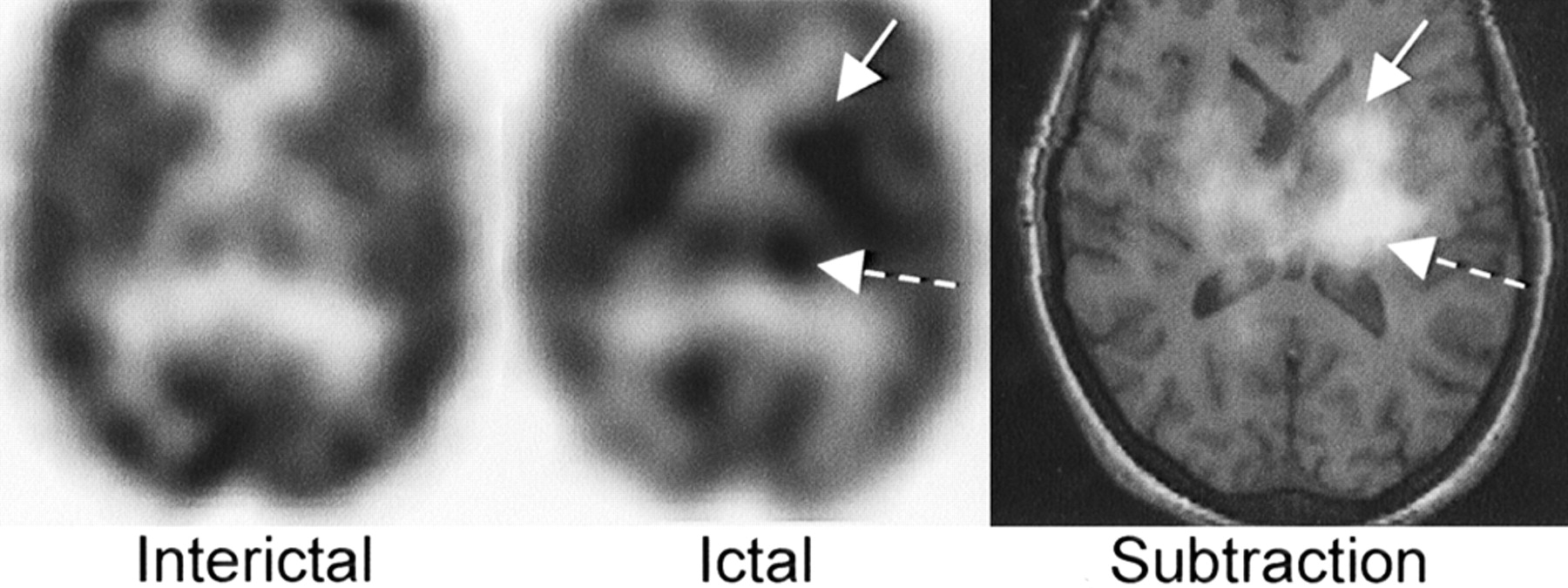
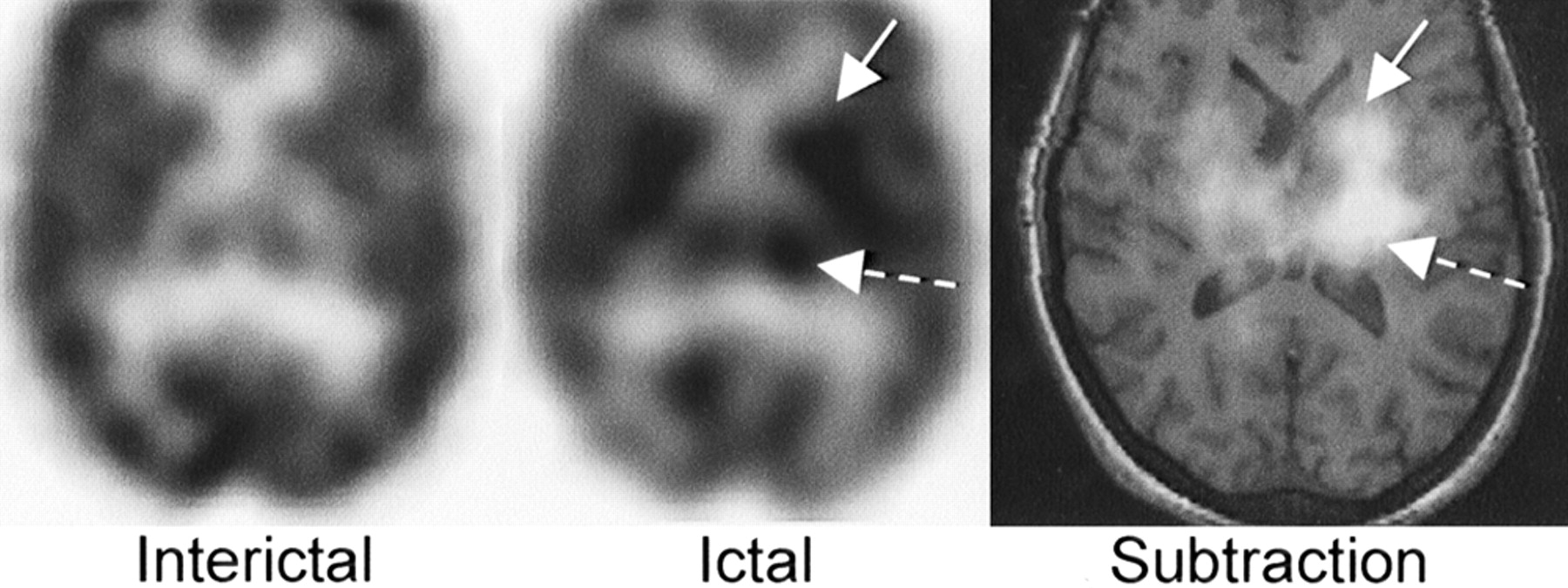
Example of contralateral basal ganglia activation. Transaxial SPECT images of patient with final focus in right temporal neocortex focus (not shown), who was found to have left basal ganglia uptake (solid arrow), right thalamic uptake (dashed arrow), and increased uptake in left temporal neocortex in study with injection time of 8 s.
Example of contralateral thalamic activation. Transaxial SPECT images show left thalamic (dashed arrow) and basal ganglia (solid arrow) activation. Left cortical activation observed in this study (presumably due to generalization of seizure) is not visualized. Patient’s final focus was located in right temporal lobe.
DISCUSSION
The anatomic connections between cortex, basal ganglia, and thalamus have been well delineated. The corticostriate connections provide communication between frontal, parietal, temporal, mesial temporal, and occipital cortices and the ipsilateral striatum. The striatum is connected afferently and efferently with the ipsilateral thalamus through fibers passing through the globus pallidus and substantia nigra. The thalamus and ipsilateral cortex communicate by reciprocal thalamocortical pathways (28). There are also interthalamic and caudocaudate pathways connecting these subcortical areas bilaterally (29). These pathways have been found to be involved in the propagation of cortical epileptiform discharges in the animal models of partial epilepsy (23–25,30–32). Furthermore, histopathologic studies of patients with known epilepsy have identified neuronal loss and gliosis in the thalami of some patients with temporal epilepsy and in all patients who died in status epilepticus (33,34).
PET studies have been instrumental in identifying interictal subcortical changes in patients with TLE. Sperling et al. (21) and Henry et al. (20) reported subcortical hypometabolism ipsilateral to the final seizure focus on interictal 18F-FDG PET studies in epilepsy patients. Dlugos et al. (35) even showed that the metabolism in subcortical structures as detected by PET correlates with the resected hippocampal cell density. Juhasz et al. (36) identified variable involvement of the lateral and dorsolateral motor nuclei of the thalamus using 18F-FDG and 11C-flumazenil PET in epilepsy patients. However, the etiology of these changes in the subcortical structures of epileptic patients is not well understood. Sperling et al. and Dlugos et al. postulated that in TLE, with the decreasing number of hippocampal cells, there is decreased activation of the striatum and thalamus as seen on PET. Yune et al. (22), in a study of thalamic hypoperfusion on interictal SPECT, suggested the possibility of thalamocortical diaschisis as a mechanism for the ipsilateral thalamic hypoperfusion during the interictal state.
Because ictal PET is impractical, most studies reporting ictal changes in the subcortical structures of both temporal and neocortical epilepsy have used SPECT (7,13–17,37). Only 2 of these studies, however, have looked specifically at the relation of subcortical structures with respect to either localizing clinical findings or final, clinically determined seizure focus. Newton et al. (19), studying dystonic posturing in temporal epilepsy patients, noted hyperperfusion of the basal ganglia ipsilateral to the seizure focus in ictal SPECT and postulated that this confirms the involvement of basal ganglia in transient dystonia. Shin et al. (18) looked at ictal basal ganglia perfusion primarily with respect to the cerebellar activation rather than the cortical seizure focus and found that cerebellar lateralization occurs contralateral to the basal ganglia uptake in 82.5% of patients. In the study of Shin et al., limited to temporal epilepsy patients, of those patients with increased uptake of radiotracer in the basal ganglia, 59% of the studies had ipsilateral and 18% had contralateral uptake with respect to SPECT cortical activation (23% of studies had bilateral basal ganglia activation).
Using the final, clinically determined seizure focus as a reference, we were able to demonstrate that, in patients in whom a unilateral seizure focus can be established, the lateralizing subcortical activation has a 77%–80% positive predictive value for the lateralization of the cortical focus. Extrapolating from experimental models of partial epilepsy, we postulate this is due to propagation of cortical impulses via known anatomic pathways to the ipsilateral basal ganglia and thalamus producing increased cerebral flow detected on the ictal SPECT studies. However, in view of the fact that >20% of studies have contralateral subcortical uptake as well as the possibility of imaging an atypical seizure for that patient (sometimes found on monitoring of intractable epilepsy patients), the subcortical structure lateralization should not be used as the sole indicator of the laterality of cortical seizure focus in intractable epilepsy patients. It may be useful in subtle or equivocal cases of cortical activation to further delineate the lateralization of the cortical focus.
Basal ganglia and thalamic activation is not restricted to TLE. We observed subcortical activation in all subgroups of neocortical epilepsies with the exception of the parietal lobe. Because subcortical activation in patients with parietal lobe epilepsy has been reported in the literature (14), we suspect that our results are due to small number of patients with parietal lobe epilepsy (n = 7) rather than a true distinction.
In our series, subcortical activation occurred contralateral to the seizure focus in 6 patients (7 studies). Most of these SPECT studies were as a whole judged either nonlocalizing or falsely localizing with respect to the final clinical focus. In addition, the false lateralization of subcortical activation followed the lateralization of cortical activation in all studies except one. Thalamothalamic and caudocaudate connections may also contribute to this contralateral activation. Another possibility for false localizations could be unsuspected multifocal seizures, but we have no evidence of this in this patient group despite multiple diagnostic studies.
Metabolic asymmetry of the thalamus on interictal PET has been correlated with worse surgical outcome in patients with TLE (38). We hypothesized that this relationship will hold in patients with extratemporal epilepsy as well. However, in our population of patients with both intractable temporal and neocortical epilepsy, we observed a statistically significant improvement in postsurgical outcome at 1-y follow-up in patients with asymmetric basal ganglia and thalamic uptake, regardless of whether the increased uptake was ipsilateral or contralateral. This relationship persisted when the outcome was evaluated using Engel’s classification at the last patient’s follow-up (Table 4). The incongruity of these studies can be due to different propagation pathways involved in mesial temporal and extratemporal epilepsy or different techniques used (studying ictal vs. interictal state, using SPECT vs. PET). The small number of mesial TLE patients and the uniformly good outcome in this subgroup limit our study. In view of this limitation, it would be helpful to look at subcortical activation of a larger group of TLE patients with greater outcome variation to see whether a worse outcome is observed in patients with thalamic uptake on ictal SPECT studies.
Major questions that arise from our study are: Why do some patients have increased uptake in subcortical structures, whereas others do not, and why, within a patient, does subcortical activation occur on some ictal scans but not on others? We observed the incidence of asymmetric subcortical activation in intractable epilepsy patients with mesial temporal and neocortical foci to be only approximately 20%–30%. One animal study found that the activation of basal ganglia structures and thalamus appeared to be related to the severity of the seizures (23), whereas others suggested a relationship between activation of basal ganglia and dystonic posturing (19). Because we were unable to find any correlation between time to injection and other patient clinical variables, we postulate that these 2 factors—severity of seizures or dystonic posturing—might be the determining factor for subcortical activation.
However, it is also possible that lateralizing subcortical activation may be due to regional differences in ECD clearance in these patients. It is possible that the clearance from subcortical structures is slowed in epilepsy patients, contributing to the differential uptake in these structures. Another possibility is that differences in ECD clearance can be attributed to the time lag between injection and scan time. One of the limitations of this study is that we have not recorded the exact time from injection to scanning. Ichise et al. (39), in a study of normal control subjects, found that images obtained up to 4 h after injection of ECD still maintain initial gray-matter activity (20); because our patients have been scanned 1–3 h after injection, this is unlikely to account for these findings.
The relatively small patient group in whom we had adequate localization of the final seizure focus also limited our study. Additionally, these patients tended to be those who had been referred for SPECT studies because of difficulties in localization by other means and may not correspond to an unselected group of intractable epilepsy patients. It is possible that a higher predictive value for subcortical structure localization may be identified in a more homogeneous group of mesial temporal epilepsy patients.
CONCLUSION
Asymmetric activation of the basal ganglia, thalamus, or both occurs in approximately 20%–30% of ictal SPECT studies regardless of the site of the cortical focus. In patients who do have asymmetric uptake in subcortical structures, the positive predictive value for the side of epileptic focus was 77% for basal ganglia and 80% for thalamus. In view of the false lateralization rate of approximately 20%, caution has to be taken in using the lateralization of subcortical structures as the sole indicator of the laterality of seizure focus. Incorporation of video-EEG and clinical data with the SPECT findings remains an important factor in the interpretation of functional imaging studies in intractable epilepsy. The presence of asymmetric thalamic and basal ganglia activation in patients with surgically treated epilepsy appears to be associated with decreased incidence of persistent seizures at follow-up.
Acknowledgments
We thank Maria V. Grau, MD, MPH, for review of the manuscript and helpful statistical advice. We also thank Richard Mazurek, Jill Lewis, Robert Wulpern, and Beryl McPhetres for the valuable technical support in performing these studies. This study was funded in part by Dupont Merck. Support was also received from the Schweizerischer Nationalfonds (Swiss National Research Foundation), the Kommission zur Forderung des academischen Nachwuchses des Kt. Zürich, and the Hitchcock Clinic.
Footnotes
Received May 14, 2002; revision accepted May 15, 2003.
For correspondence or reprints contact: Petra J. Lewis, MBBS, Department of Radiology, Dartmouth-Hitchcock Medical Center, One Medical Center Dr., Lebanon, NH 03756.
E-mail: petra.lewis{at}hitchcock.org




{kind=link}
{kind=link}
{kind=link}
{kind=link}