


Abstract
Gated SPECT allows combined assessment of regional myocardial perfusion and left ventricular function. The aim of this study was to address the prognostic value of gated SPECT performed during dobutamine stress testing and during rest on patients with acute myocardial infarction treated with thrombolysis. Methods: Eighty-eight consecutive patients with uncomplicated acute myocardial infarction who underwent predischarge (3–7 d after admission) dobutamine (5–40 μg/kg of body weight per minute in 3-min dose increments) and rest gated 99mTc-sestamibi SPECT were followed for a mean of 48 mo (range, 4–64 mo). Results: Eighteen cardiac events (8 cardiac deaths and 10 nonfatal myocardial infarctions) occurred. Ischemia at dobutamine SPECT imaging (summed difference score ≥ 1) was present in 60% of the patients. In patients without ischemia, there was a lower event rate (11%), compared with patients with mild ischemia (18%) and moderate-to-severe ischemia (40%) (P < 0.05). Patients with events showed also a higher summed difference score, compared with patients without events (2.3 ± 1.6 vs. 1.3 ± 1.6, P < 0.05). Independent predictors of events were the number of segments with preserved 99mTc-sestamibi uptake at rest and the number of akinetic or dyskinetic segments with preserved 99mTc-sestamibi uptake and preserved wall thickening (global χ2 of the model, 13.6; P < 0.01). The assessment of the incremental prognostic value of variables added sequentially showed that the addition of the summed difference score added information to perfusion status at rest (P < 0.05). Combined assessment of regional myocardial perfusion and left ventricular function at rest further improved the model (P < 0.05). Conclusion: The present study indicated that predischarge 99mTc-sestamibi gated SPECT gives prognostic information on patients recovering from acute myocardial infarction. Patients with preserved systolic wall thickening should be regarded as a high-risk subgroup, requiring closer follow-up for appropriate treatment.
Identifying among patients recovering from acute myocardial infarction those at risk for subsequent cardiac events is important for clinical decision making. Predischarge exercise or pharmacologic perfusion imaging has incremental prognostic value over clinical data in the assessment of these patients for risk stratification (1–5). The measurement of infarct size by cardiac SPECT at the time of hospital discharge is also a useful parameter for predicting functional recovery and prognosis (6,7). Gated SPECT allows combined assessment of myocardial perfusion and left ventricular (LV) function during a single examination, and this technique has been extensively discussed and validated (8–12). The addition of functional information to perfusion data improves the detection of multivessel coronary artery disease and helps to evaluate the physiologic significance of mild coronary artery disease, sometimes insufficient to result in perceptible flow disturbances but already responsible for wall thickening abnormalities (13,14). The ability of combined assessment of LV ejection fraction and perfusion data to predict cardiac events in patients with coronary artery disease (15–17) and after myocardial infarction (18,19) has been previously demonstrated. However, the prognostic value of gated SPECT in the subset of patients with uncomplicated myocardial infarction who do not undergo subsequent revascularization has not been extensively evaluated. Therefore, the present study was designed to assess the prognostic value of the combined analysis of regional myocardial perfusion and LV function by gated SPECT during dobutamine stress and rest in patients after uncomplicated myocardial infarction treated with thrombolysis, excluding those referred for coronary revascularization.
MATERIALS AND METHODS
From June 1996 to December 1997, 138 consecutive patients underwent predischarge (3–7 d after admission) myocardial perfusion gated SPECT with 99mTc-sestamibi after a first uncomplicated acute myocardial infarction. All patients were treated with systemic thrombolysis during the acute phase. All patients met the following criteria: the acute infarction was their first Q-wave myocardial infarction; they were in stable hemodynamic condition; and they had no early postinfarction angina, a sinus rhythm, and no conduction disturbances. Patients with a history of diabetes, severe hypertension with LV hypertrophy, valvular heart disease or other detectable cardiac disorders, or severe concomitant illness were excluded. All patients underwent coronary angiography within the first month after the acute infarction. Forty-six patients who underwent revascularization procedures within 90 d from the radionuclide imaging were excluded, leaving 92 patients with available data to be analyzed. At discharge, all these latter patients were receiving antiplatelet agents and nitrates. The decision to submit patients to coronary revascularization was made by referring physicians taking into account symptoms, coronary anatomy, and patient preferences and without being aware of the results of radionuclide studies. The ethics committee of our institution approved the protocol, and all patients provided informed consent.
Stress Test and Imaging
All patients underwent dobutamine and rest cardiac SPECT imaging. Dobutamine was infused in 3-min dose increments at 5, 10, 20, 30, and 40 μg/kg of body weight per minute with monitoring of symptoms, blood pressure, and 12-lead electrocardiography. The peak dose was achieved in 82 patients. In the other patients, dobutamine infusion was stopped because age-predicted maximal heart rate was achieved (n = 4) or complex ventricular arrhythmia appeared (n = 2). No patients developed severe anginal pain, hypotension, or other intolerable side effects. 99mTc-sestamibi, 740 MBq, was injected intravenously 1–2 min before completion of the dobutamine infusion, and imaging was performed 60 min later. Rest imaging was performed on a separate day 60 min after tracer injection (740 MBq). Data were acquired using a rotating single-head gamma camera (SP4HR; Elscint) equipped with a low-energy, all-purpose, parallel-hole collimator and connected with a dedicated computer system. Gating was performed using a 100% acceptance window with acquisition of 8 frames per cycle. Perfusion imaging was reconstructed by summing the gated data at each projection into an “ungated” raw data file before low-phase prefiltering and ramp-filtered backprojection. Thirty-two projections (30 s per projection) were obtained over a semicircular 180° arc, which extended from the 30° right anterior oblique to the left posterior oblique position. A 20% symmetric energy window centered on the 140-keV peak was used. Filtered backprojection was then performed with a low-resolution Butterworth filter with a cutoff frequency of 0.5 cycle per pixel, order 5.0. No attenuation or scatter correction was applied.
Two independent observers who were unaware of angiographic findings analyzed scintigraphic studies. Discordance in the evaluation was resolved by consensus, using a third observer. For each patient, 13 anatomic segments were scored using a 4-point system (3 = absence of tracer uptake, 2 = severe reduction of uptake, 1 = moderate reduction of uptake, and 0 = normal uptake). High intra- and interobserver reproducibility for visual analysis has been reported by our institution (20). Discordance in the evaluation was resolved by consensus. Segments with reduced tracer uptake were considered reversible defects if the activity score decreased ≥1 point from stress to rest. Scintigraphic variables incorporating both the extent and the severity of perfusion defects were calculated (21). A summed stress score reflecting both ischemia and scar was obtained by adding the scores of the 13 segments of the stress images. A summed rest score reflecting the extent of nonreversible defects was obtained by adding the scores of the 13 segments of the rest images. Finally, a summed difference score representing the amount of ischemic myocardium was calculated as the sum of differences between each of the 13 segments on the stress and rest images (22). Patients were considered to have no ischemia if their score was 0, mild ischemia if their score was 1–2, and moderate to severe ischemia if their score was >2.
For each segment, 2 readers performed a masked evaluation of wall motion and wall thickening on resting gated SPECT images. Discordance in the evaluation was resolved by consensus, using a third observer. Wall motion was visually scored using a 3-point scoring system (1 = normal, 2 = hypokinetic, and 3 = akinetic or dyskinetic). Akinetic or dyskinetic segments were considered to show preserved 99mTc-sestamibi uptake when the tracer activity score was 0 or 1 and severely reduced 99mTc-sestamibi uptake when the tracer activity score was 2 or 3. Wall thickening was scored from normal to absent (1 = normal, 2 = reduced, and 3 = absent) on the basis of visually assessed brightening of the myocardial wall in systole. Regional wall thickening was considered normal if a ≥20% increase in count density occurred in the portion of the defect with the lowest count density during systole. Change in count density was estimated by visual comparison with a reference color scale displayed alongside each set of images. For segments in which functional assessment was not possible because of absence of tracer uptake, a score of 3 was assigned for both wall motion and thickening. Akinetic or dyskinetic segments were evaluated as having preserved wall thickening (score of 1 or 2) or absence of apparent wall thickening (score of 3).
In all patients, on the day of SPECT imaging (3–7 d after admission), LV ejection fraction was assessed by standard echocardiography using a Sonos 1000 ultrasound system (Hewlett-Packard). LV volumes were measured using the modified biplane Simpson’s rule algorithm. The mean values of 3 measurements of the technically best cardiac cycles were taken from each examination.
Follow-up
Follow-up was obtained for a mean of 48 mo after discharge (range, 4–64 mo). Scripted and masked telephone interviews were performed. Events were defined as either cardiac death or nonfatal myocardial infarction, whichever occurred first. The occurrence of late (>90 d from radionuclide studies) revascularization procedures was also monitored. Cardiac death was confirmed by review of death certificates and hospital charts or physician records, and nonfatal myocardial infarction was evidenced by hospital records indicating the appropriate combination of symptoms, the electrocardiogram, and levels of myocardial creatinine phosphokinase. Four patients were lost to follow-up and therefore were excluded from the study.
Statistical Analysis
Continuous variables are expressed as mean ± SD, and categoric data as percentage. Patients with and without events were compared using the 2-tailed Student t test for continuous variables and the Yates-corrected χ2 test for categoric variables. A P value < 0.05 was considered statistically significant. Cox proportional hazards regression analysis was applied to determine independent predictors of events. To avoid detecting spurious associations (23), only 4 variables were analyzed: LV ejection fraction, total number of segments with preserved 99mTc-sestamibi uptake at rest, number of akinetic or dyskinetic segments with preserved 99mTc-sestamibi uptake and preserved wall thickening, and summed difference score. For each variable, the regression coefficient B and its exponent expB (hazards ratio) with 95% confidence intervals were calculated. Two different multivariate analyses were performed. The first was performed according to the unmodified forward stepwise procedure to evaluate the independent prognostic value of the variables; for this analysis, variables were entered into or removed from the model on the basis of a computed significance probability (maximized partial-likelihood ratio). The latter multivariate analysis aimed to assess the incremental prognostic value of variables added sequentially on the basis of the increases in the overall likelihood ratio statistics. The increment in information provided by the model at each step was considered significant when the difference in log-likelihood associated with each model, adjusted for differences in degree of freedom, corresponded to P < 0.05. Finally, a power analysis was performed to determine the possibility of a type II error. The statistical software used was SPSS 10.0 and SamplePower 1.0 (SPSS Inc.).
RESULTS
Eighty-eight patients (73 men; mean age, 53 ± 10 y) had available follow-up data. Characteristics of these patients are reported in Table 1. The length of follow-up was 54.6 ± 9.4 mo in patients without events and 21 ± 8.3 mo in patients with events (P < 0.05). Cardiac events occurred in 18 (21%) patients (8 cardiac deaths and 10 nonfatal myocardial infarctions). Reinfarction occurred in the same coronary artery territory in 6 patients and in a different vascular territory in 4 patients. No late revascularization procedure occurred.
Characteristics of Study Population (n = 88)
Clinical and Imaging Data in Patients With and Without Cardiac Events
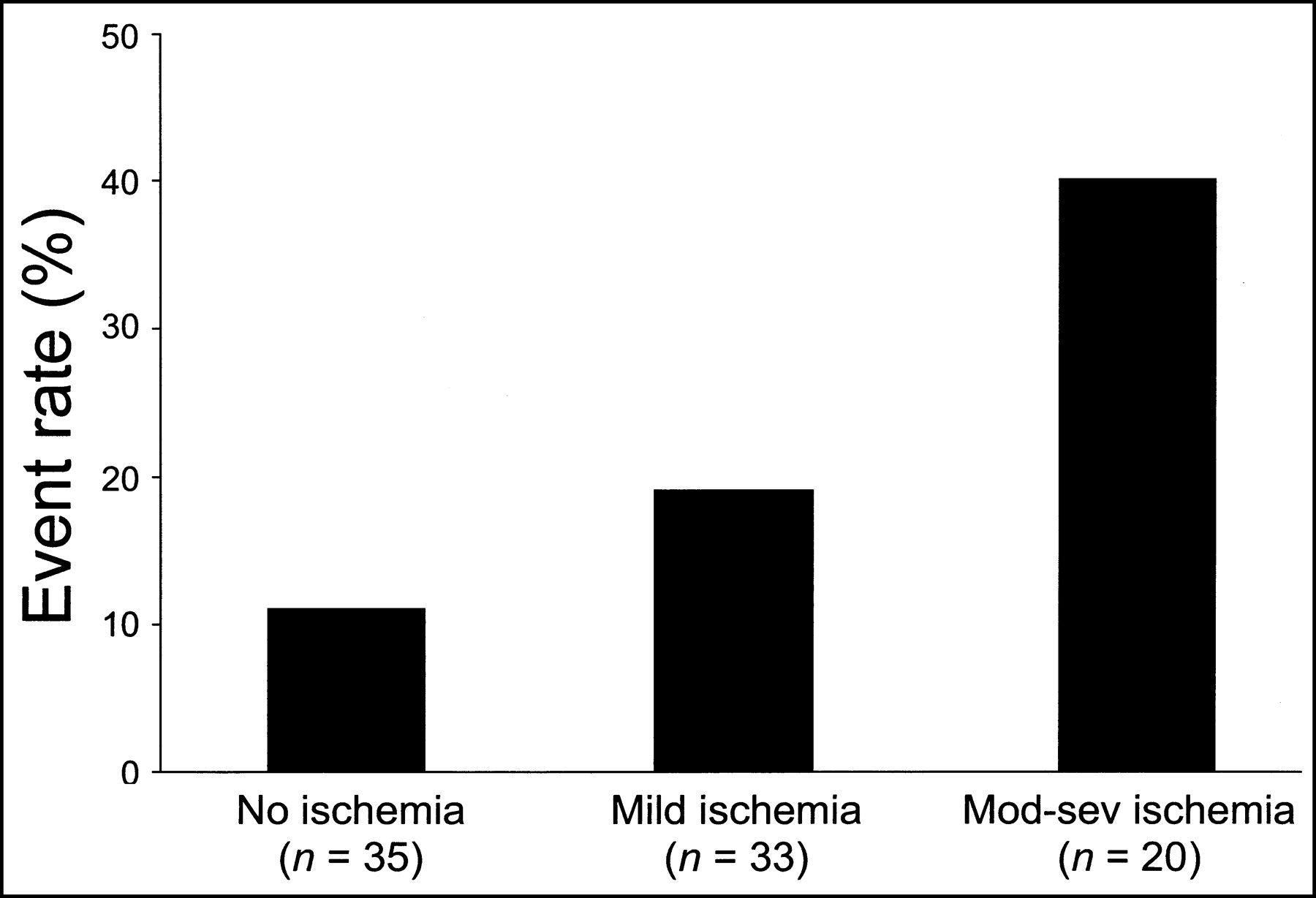
As reported in Table 2, age, sex, site of myocardial infarction, number of diseased coronary vessels and echocardiographic LV ejection fraction were not different in patients with and in those without events. After dobutamine, myocardial ischemia at SPECT imaging (summed difference score ≥ 1) was present in 53 (60% of the total) patients. In patients with moderate-to-severe ischemia, there was a higher event rate (40%), compared with patients with mild ischemia (18%) and without ischemia (11%) (P < 0.05; Fig. 1). Reversible defects were within the infarct-related area in 20 patients, in remote areas in 6 patients, and in both infarct-related and distant areas in 12 patients. Patients with events showed a higher summed difference score, compared with patients without events (Table 2). In contrast, site of ischemia and summed stress score were not different and summed rest score showed only borderline significance. Power analysis revealed that this study had only a 72% chance of detecting a difference of 2 in summed rest score between patients with and without events.
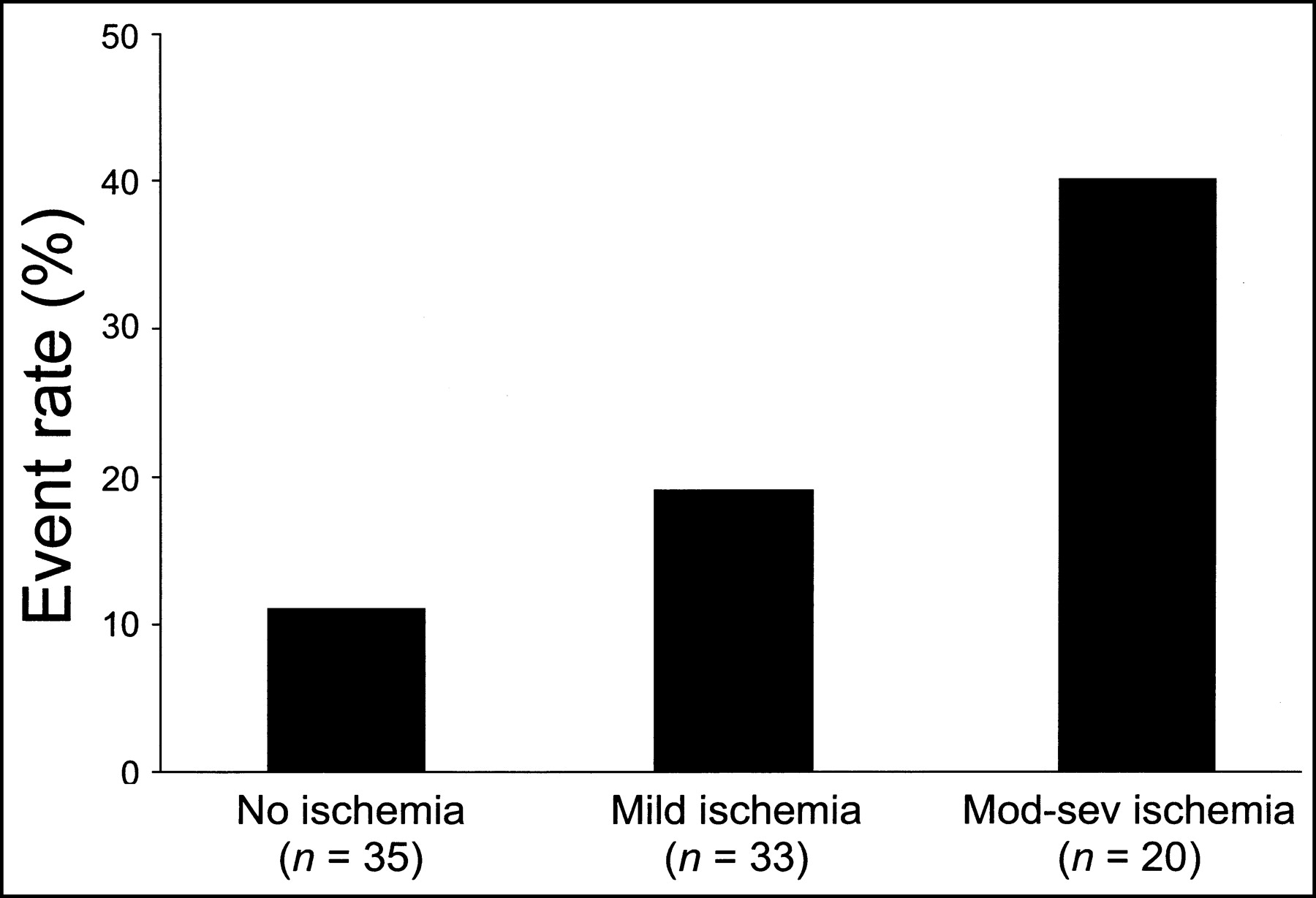
Event rate in patients without ischemia (summed difference score = 0), with mild ischemia (summed difference score of 1 to 2), and with moderate-to-severe (mod-sev) ischemia (summed difference score > 2). Statistically significant increase in cardiac events occurred as function of SPECT result (P < 0.01).
Characteristics of Patients With and Without Cardiac Events
Patients with events showed a higher number of segments with preserved 99mTc-sestamibi uptake at rest (tracer activity score of 0 or 1), compared with patients without events (Table 2). The total number of akinetic or dyskinetic segments was comparable in patients with and in those without events (3.11 ± 2.60 vs. 3.94 ± 1.61, respectively, P = not statistically significant). Akinetic or dyskinetic segments were evaluated according to 99mTc-sestamibi uptake and to presence or lack of wall thickening at gated SPECT (Table 3). Patients with events showed a lower number of akinetic or dyskinetic segments with reduced 99mTc-sestamibi uptake (tracer activity score of 2 or 3) and a greater number of akinetic or dyskinetic segments with preserved 99mTc-sestamibi uptake and preserved wall thickening.
Sestamibi Activity and Regional LV Function in Akinetic or Dyskinetic Segments
Independent Predictors of Cardiac Events
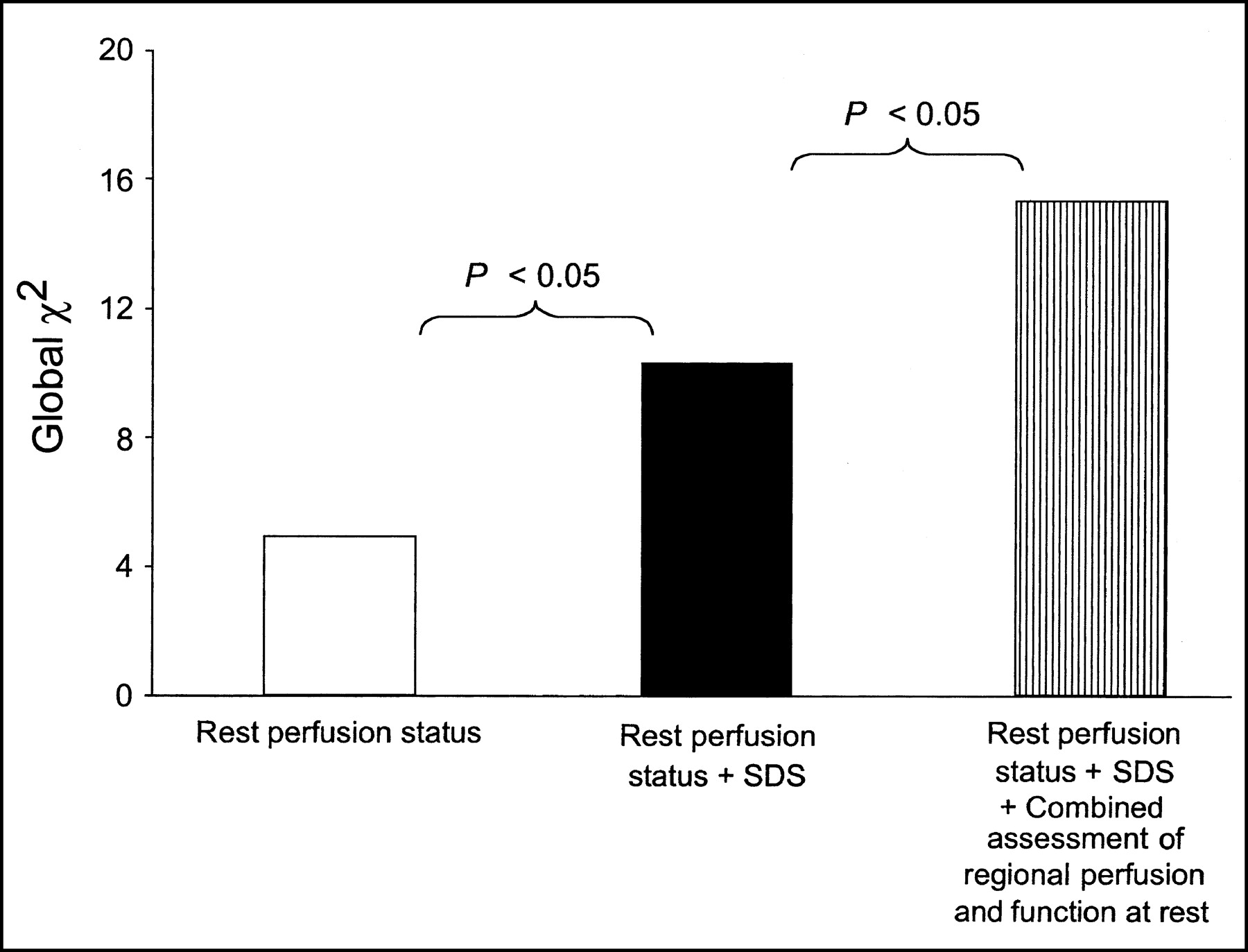
At stepwise multivariate analysis, among the variables considered independent predictors of cardiac events were the number of segments with preserved 99mTc-sestamibi uptake at rest and the number of akinetic or dyskinetic segments with preserved 99mTc-sestamibi uptake and preserved wall thickening (global χ2 of the model = 13.6; P < 0.01) (Table 4). The incremental prognostic value of variables added sequentially is depicted in Figure 2. As shown, the addition of summed difference score added prognostic information to perfusion status at rest, increasing the global χ2 of this model from 4.92 to 10.32 (P < 0.05). Combined assessment of regional myocardial perfusion and LV function at rest induced a further significant improvement of the model, increasing the global χ2 to 15.31 (P < 0.05).
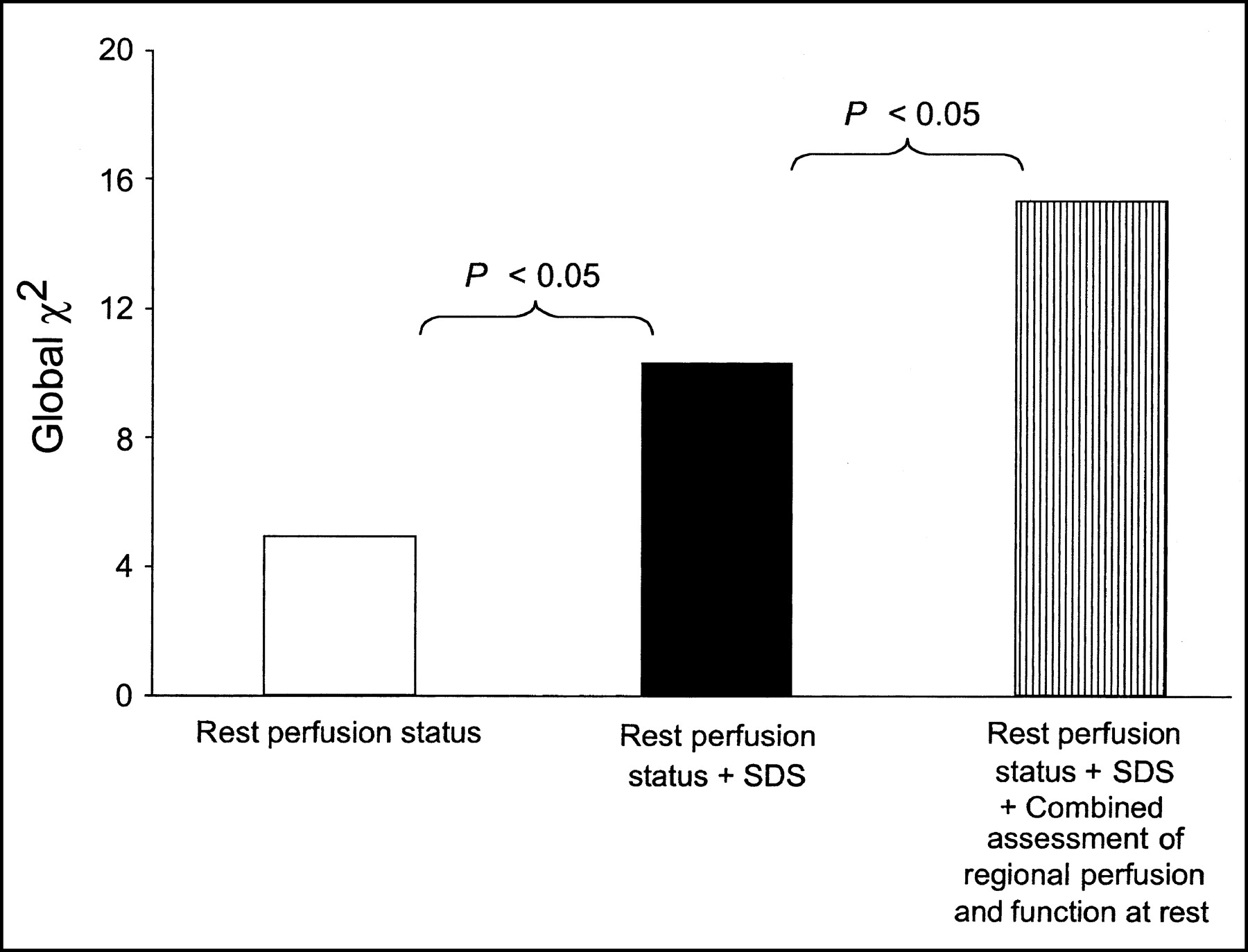
Incremental prognostic value for cardiac events (global χ2 values on y-axis) obtained with consideration of hierarchical order: rest perfusion status (regional 99mTc-sestamibi activity score at rest; white bar); rest perfusion status and summed difference score (black bar); and rest perfusion status, summed difference score, and combined assessment of regional perfusion and regional function (i.e., regional wall thickening score at rest) at rest in akinetic or dyskinetic segments (hatched bar). SDS = summed difference score.
Independent Predictors of Cardiac Death or Recurrent Acute Myocardial Infarction
DISCUSSION
A composite of cardiovascular death and myocardial infarction was the outcome of interest of the present study, designed to investigate the prognostic value of dobutamine stress–rest gated 99mTc-sestamibi SPECT imaging in patients after acute uncomplicated myocardial infarction who were treated with thrombolysis and did not undergo subsequent revascularization. Stress testing performed with dobutamine represents the usual pharmacologic provocative test in patients with recent myocardial infarction at our institution. The results demonstrated that in this subset of patients, a finding of ischemia on dobutamine SPECT is associated with a poor outcome. However, combined assessment of regional perfusion and LV function at rest provided independent and incremental prognostic information over that obtained by the dobutamine stress test.
The prediction of subsequent risk after an acute myocardial infarction is a stimulating challenge for cardiologists. Identification of patients at risk of cardiac death and recurrent myocardial infarction is important for selecting the appropriate treatment. In areas of infarction, there may be a mixture of necrotic, ischemic, and viable tissue (24,25). A finding of ischemia on radionuclide perfusion imaging has been shown to be a predictor of events after acute myocardial infarction, although not consistently so (16–18). In our study, stress-induced ischemia was associated with an increased risk of cardiac events during follow-up. However, the prognostic power was lessened by multivariate analysis. The likely explanation is that most patients with significant ischemia on predischarge testing underwent early revascularization and were censored from our population. Similarly, the prognostic value of myocardial viability has been investigated with conflicting results. In particular, some investigators have reported a beneficial effect of viability on prognosis, whereas others have reported a negative or neutral effect (26–28).
Radionuclide imaging techniques have been shown to correctly differentiate necrotic from hypoperfused but still viable myocardium in dysfunctional areas. Perfusion imaging at rest has been increasingly used to assess myocardial viability, and considerable emphasis has been placed on the amount of tracer uptake within dysfunctional regions (29). A large body of evidence supports the validity of 99mTc-sestamibi SPECT imaging for determination of the infarct area (6,7,30,31). A close association between 99mTc-sestamibi activity and the extent of histologically viable myocardium has been found (32–34). The addition of gating to myocardial perfusion SPECT provides accurate and reproducible information on LV function (8–12). Therefore, the addition of functional information to perfusion imaging may improve the ability to identify viable myocardium. Currently, assessment of regional function involves visual analysis of the endocardial border on gray-scale display or visual analysis of regional myocardial thickening on color display.
Gated SPECT with 99mTc-labeled sestamibi or tetrofosmin was found to have a considerable prognostic impact on patients after acute myocardial infarction (18,19). Analysis focusing on global LV systolic function demonstrated that LV ejection fraction by gated SPECT is an independent predictor of cardiac events. Patients with LV ejection fraction < 40% showed a nearly 3-fold increase in risk for cardiac death or infarction over those with a lesser impairment of LV systolic function (18,19). These findings agree with those of previous studies assessing LV ejection fraction by radionuclide angiography (35) and reflected those found in larger populations of unselected patients with known or suspected coronary artery disease (16,17). In the present study, a low prevalence of severely reduced LV ejection fraction and of 2- or 3-vessel disease placed the patients at low risk. In this setting of patients with myocardial infarction, regional perfusion and function were better predictors of outcome than was global LV function. A noteworthy finding was that changes in regional function did not always parallel those in perfusion. In asynergic regions, it was possible to identify different patterns characterized by normal perfusion, mildly reduced perfusion, or severely reduced perfusion, with or without associated systolic thickening. In our patient population, the strongest predictor of cardiovascular risk was the presence of dysfunctional but viable myocardium with preserved systolic thickening. As is known, dysfunctional myocardium with mildly reduced tracer uptake and preserved systolic thickening might represent either nontransmural necrosis or viable, although hypoperfused, tissue. It is conceivable that this latter condition might carry a high likelihood of subsequent ischemic events. These findings seem to be in contrast to those of other studies demonstrating that larger infarct size measured by 99mTc-sestamibi imaging after acute myocardial infarction is associated with an increased mortality risk during a short-term follow-up (7). However, one should consider that in the patients of the present study the infarct size was quite small and that in previous investigations only infarcts > 12% of the LV myocardial mass correlated to mortality (7). In the patients of the present study, a small extent of necrosis signified an unfavorable prognosis. In fact, viable jeopardized myocardium may be a trigger of events in patients with normal LV function. Risk stratification of patients with an uncomplicated acute myocardial infarction and without severe impairment of LV function relies mainly on the identification of viable jeopardized myocardium within the infarct area and of stress-induced ischemia in remote areas. In our study population, the decision to submit patients to revascularization or medical treatment was made by referring physicians taking into account symptoms, coronary anatomy, and patient preferences and without knowing the results of radionuclide studies. In addition, this decision was probably influenced by the consideration that patients with single-vessel disease and uncomplicated myocardial infarction should present a relatively low risk. However, the present findings indicate that patients recovering from an uncomplicated acute myocardial infarction who have residual dysfunctional but viable myocardium with preserved systolic wall thickening should be regarded as a high-risk subgroup, demanding closer follow-up for appropriate treatment. In this study, patients with LV hypertrophy or conduction disturbances, such as left bundle branch block, were excluded. In these subsets of patients, radionuclide cardiac tomography would give more valuable prognostic information, compared with exercise electrocardiography or stress echocardiography (36–38).
The present study had potential limitations. The relatively small number of patients and consequent small number of cardiac events did not allow for separate evaluation of cardiac death and nonfatal myocardium infarction. Furthermore, some variables showed only borderline statistical significance in predicting the outcome, and this finding may also have been due to inadequate sample size. In fact, at post hoc analysis, the power of the study was <80%, the usually accepted lower limit of statistical power. Finally, follow-up coronary angiography was not performed. Although a progression of coronary artery disease in patients with adverse events could not be excluded, the relationship between adverse events and the presence of postinfarct myocardial viability was meaningful.
CONCLUSION
Among patients with uncomplicated myocardial infarction not referred for early revascularization and with relatively preserved global LV function, combined assessment of regional myocardial perfusion and LV function by gated SPECT adds information to that obtained from the dobutamine stress test and is useful to estimate risk for subsequent cardiac events. Therefore, in this subset of patients, gated SPECT has the potential to play an essential role in identifying those at a high enough risk to warrant more aggressive strategies.
Acknowledgments
The authors thank Carmine di Nuzzo for his excellent technical assistance in the execution of the radionuclide imaging studies.
Footnotes
Received Nov. 4, 2002; revision accepted Mar. 10, 2003.
For correspondence or reprints contact: Alberto Cuocolo, MD, Dipartimento di Scienze Biomorfologiche e Funzionali, Università Federico II, Via Pansini, 5, 80131 Napoli, Italy.
E-mail: cuocolo{at}unina.it




{kind=link}
{kind=link}