


Abstract
This study directly compared the prognostic value of predischarge dobutamine stress echocardiography (DSE) and dobutamine myocardial SPECT perfusion imaging in patients with prior myocardial infarction. Methods: The study population consisted of 146 consecutive patients who underwent predischarge DSE and SPECT with 99mTc-sestamibi after a first acute uncomplicated myocardial infarction treated with thrombolysis. Fifty patients who underwent revascularization within 90 d from the imaging studies were excluded. Cardiac death and nonfatal myocardial infarction were considered events. Follow-up was 98% complete in a mean period of 44 ± 19 mo. Results: Myocardial ischemia was detectable in 55 (58%) patients at SPECT and in 63 (67%) patients at DSE. Concordance between SPECT and DSE in detecting ischemia was observed in 68 (72%) of the 94 patients (κ value, 0.41). During the follow-up, there were 20 cardiac events (9 deaths and 11 nonfatal myocardial infarctions). Ischemia at SPECT was a significant predictor of events (hazards ratio = 4.8; 95% confidence interval, 1.4–16.3; P < 0.01). However, ischemia at DSE (biphasic or worsening patterns) was not associated with events, whereas biphasic pattern alone was associated with a poor outcome compared with direct worsening (P < 0.05). Finally, at Cox multivariate analysis, ischemia at SPECT but not biphasic pattern at DSE was a significant independent predictor of events (P < 0.01). Conclusion: These results indicate that, after uncomplicated myocardial infarction, ischemia at SPECT is associated with an increased risk of cardiac events at long-term follow-up. However, ischemia at DSE was unable to stratify patients after myocardial infarction.
Residual ischemia after acute myocardial infarction is a significant predictor of adverse outcome (1,2). Stress myocardial perfusion imaging with SPECT and echocardiography has been widely used for the detection of stress-induced ischemia (3–6). The value of stress echocardiography is enhanced by the assessment of inotropic reserve during low-dose dobutamine infusion and the detection of wall motion deterioration during high-dose infusion, particularly in patients with wall motion abnormalities at rest (7,8). Several studies have demonstrated the prognostic value of SPECT and stress echocardiography in patients with prior myocardial infarction (9–13). Despite the extensive use of both stress echocardiography and SPECT in the evaluation of myocardial ischemia and viability, the comparative prognostic value of these noninvasive techniques in patients after acute myocardial infarction has not been defined. Few data have directly compared the value of exercise echocardiography and SPECT for risk stratification in the same patients with suspected or known coronary artery disease (14,15). The aim of this prospective study was to directly compare the prognostic value of predischarge dobutamine stress echocardiography (DSE) and dobutamine SPECT in patients after uncomplicated acute myocardial infarction treated with thrombolysis.
MATERIALS AND METHODS
Study Population
From June 1996 to June 1998, a total of 183 patients (152 men; mean age, 55 ± 12 y) with a first acute uncomplicated myocardial infarction were referred to the coronary care unit of our university. Of these, 146 consecutive patients (123 men; mean age, 54 ± 11 y) underwent predischarge (3–7 d after admission) DSE and SPECT with 99mTc-sestamibi. All patients were treated with systemic thrombolysis during the acute phase and met the following criteria: first Q-wave myocardial infarction, stable hemodynamic conditions, no early postinfarction angina, sinus rhythm, and no conduction disturbances. Patients with history of severe hypertension, valvular heart disease, or other detectable cardiac disorders or severe concomitant illness were excluded. Fifty patients who underwent revascularization procedures within 90 d from the imaging studies were not considered for the purpose of the present investigation, which left 96 patients with available data to be analyzed. At discharge, all of the latter patients were on antiplatelet agents and nitrates. The decision to submit patients to coronary revascularization was made by referring physicians. The ethics committee of our institution approved the protocol and all patients provided the informed consent.
Stress Test and Image Acquisition
All patients underwent a predischarge dobutamine stress test with simultaneous echocardiography and SPECT. Antianginal medications, except nitrates, were discontinued 48 h before imaging in all patients. Dobutamine was infused in 3-min dose increments at 5, 10, 20, 30, and 40 μg/kg body weight per minute with monitoring of symptoms, blood pressure, and 12-lead electrocardiography. Test endpoints were target heart rate (85% of age- and sex-related maximal heart rate), horizontal or downsloping ST-segment depression >2 mm, ST-segment elevation >1 mm, severe angina, systolic blood pressure decrease >20 mm Hg, blood pressure >220/120 mm Hg, or clinically important cardiac arrhythmias. If the test endpoint was not reached at the maximum dose, atropine (up to 1 mg) was given. An intravenous β-blocker was used to reverse the effects of dobutamine or atropine. Standard 2-dimensional echocardiogram, using a Hewlett-Packard Sonos 1000 ultrasound system was continuously monitored during the test and up to 10 min after the end of the infusion. 99mTc-Sestamibi (740 MBq) was injected intravenously 1–2 min before completion of dobutamine infusion and SPECT was performed 60 min later. Rest imaging was performed on a separate day 60 min after tracer injection (740 MBq). SPECT data were acquired using a rotating single- head γ-camera (Elscint SP4HR) equipped with a low-energy, all-purpose, parallel-hole collimator and connected with a dedicated computer system. Thirty-two projections (30 s per projection) were obtained over a semicircular 180° arc, which extended from the 30° right anterior oblique to the left posterior oblique position. No attenuation or scatter correction was applied.
Image Analysis
At echocardiography, regional wall motion was visually evaluated, using a 3-point scoring system (1 = normal, 2 = hypokinetic, 3 = akinetic or dyskinetic) in 13 segments, by 2 experienced observers, who were unaware of scintigraphic data. In case of disagreement, consensus was achieved by a third observer. DSE results were classified as biphasic response (low-dose improvement followed by a high-dose deterioration); worsening (direct deterioration at low or high dose); sustained improvement (low-dose improvement that was maintained at high dose); no change (no change during the entire protocol). Patients with biphasic response or worsening response patterns in at least one segment were considered as having ischemia.
Two independent observers who were unaware of echocardiographic findings analyzed SPECT studies. Discordance in the evaluation was resolved with a consensus of a third observer. In each patient, 13 anatomic segments were scored using a 4-point system (3 = no tracer uptake, 2 = severe reduction, 1 = moderate reduction, 0 = normal tracer uptake). Segments with reduced tracer uptake were considered reversible defects if the activity score decreased ≥1 point from stress to rest. Scintigraphic variables incorporating the extent and severity of perfusion defects were calculated (16). A summed stress score reflecting both ischemia and scar was obtained by adding the scores of the 13 segments of the stress images. A summed rest score reflecting the extent of nonreversible defects was obtained by adding the scores of the 13 segments of the rest images. Finally, a summed difference score representing the amount of ischemic myocardium was calculated (17). Patients with a summed difference score of 0 were considered as having no ischemia, score of 1–2 as having mild ischemia, and a score of >2 as having moderate-to-severe ischemia (11).
The intra- and interobserver concordances for both echocardiography and SPECT studies have been assessed in a subgroup of 10 patients. For echocardiography, intra- and interobserver concordance was 92% and 90%, respectively. For SPECT, intra- and interobserver concordance was 98% and 96%, respectively.
Follow-Up
Scripted and blinded telephone interviews were periodically performed. Events were defined as either cardiac death or nonfatal myocardial infarction, whichever occurred first. The occurrence of late (>90 d from imaging studies) revascularization procedures was also monitored. Cardiac death was confirmed by review of death certificates and hospital charts or physicians records, and nonfatal infarction was evidenced by hospital records, indicating the appropriate combination of symptoms, electrocardiogram, and myocardial creatinine phosphokinase and troponin levels.
Statistical Analysis
Continuous variables are expressed as mean ± SD and categoric data are expressed as percentage. The κ statistic was used as a measure of agreement between SPECT and DSE. A value of 1 denotes perfect agreement, and 0 indicates no agreement beyond chance. In general, κ values ≥ 0.5 are considered indicative of good agreement. Univariate and multivariate Cox regression analyses were performed to identify among clinical variables and variables representing myocardial ischemia at both DSE and SPECT those associated with outcome (18,19). For each variable, the regression coefficient B and its exponent expB (hazards ratio) with 95% confidence intervals were calculated. Two different multivariate analyses were performed. The first was performed according to the unmodified forward stepwise procedure to evaluate the independent prognostic value of the variables; for this analysis, variables were entered into or removed from the model on the basis of a computed significance probability (maximized partial likelihood ratio). The validity of the models was measured by means of the concordance statistic (C index). The latter multivariate analysis aimed to assess the incremental prognostic value of variables added sequentially on the basis of the increases in the overall likelihood ratio statistics. An increment in information of the model at each step was considered significant when the difference in log-likelihood associated with each model, adjusted for differences in degree of freedom, corresponded to P < 0.05. Survival curves were constructed using the Kaplan–Meier method to account for censored survival times and were compared with the log rank test (18). P < 0.05 was considered significant. The statistical software used was SPSS 11.0 (SPSS Inc.).
RESULTS
Follow-up was 98% complete in a mean period of 44 ± 19 mo (range, 7–76 mo) and was available in 94 patients (79 men; mean age, 53 ± 10 y). Characteristics of these patients are reported in Table 1. Cardiac events occurred in 20 (21%) patients (9 cardiac deaths and 11 nonfatal myocardial infarctions). A late revascularization procedure occurred in 4 patients. These latter patients were censored at the time of the procedure to avoid potential referral bias.
Clinical Data and Stress Test Results of Study Population (n = 94)
Stress Test Results
The peak dose was achieved in 89 patients. In 26 (29%) of these patients, atropine was added. In 7 patients, dobutamine infusion was stopped for achievement of age-predicted maximal heart rate (n = 5) or appearance of complex ventricular arrhythmia (n = 2). No patients developed severe anginal pain, hypotension, or other intolerable side effects.
Stress test results of the overall study population are reported in Table 1. At SPECT, myocardial ischemia was detectable in 55 (58%) patients (homozonal in 45 and heterozonal in 10). In particular, 34 (62%) of these patients had mild ischemia and 21 (38%) had moderate-to-severe ischemia. At DSE, the response pattern was biphasic in 16 (17%) patients, worsening in 47 (50%) patients, sustained improvement in 9 (10%) patients, and no change in 22 (23%) patients. Thus, 63 (67%) patients were considered to have myocardial ischemia at DSE (homozonal in 53 and heterozonal in 10). Concordance between SPECT and DSE in detecting ischemia was observed in 68 (72%) of the 94 patients and the κ value was 0.41 (Fig. 1). The coronary territory distribution for regions with myocardial ischemia at SPECT and DSE is illustrated in Table 2. Among the 26 patients with discordant results, 17 (65%) had myocardial ischemia at DSE but not at SPECT and 9 (35%) had ischemia at SPECT but not at DSE.
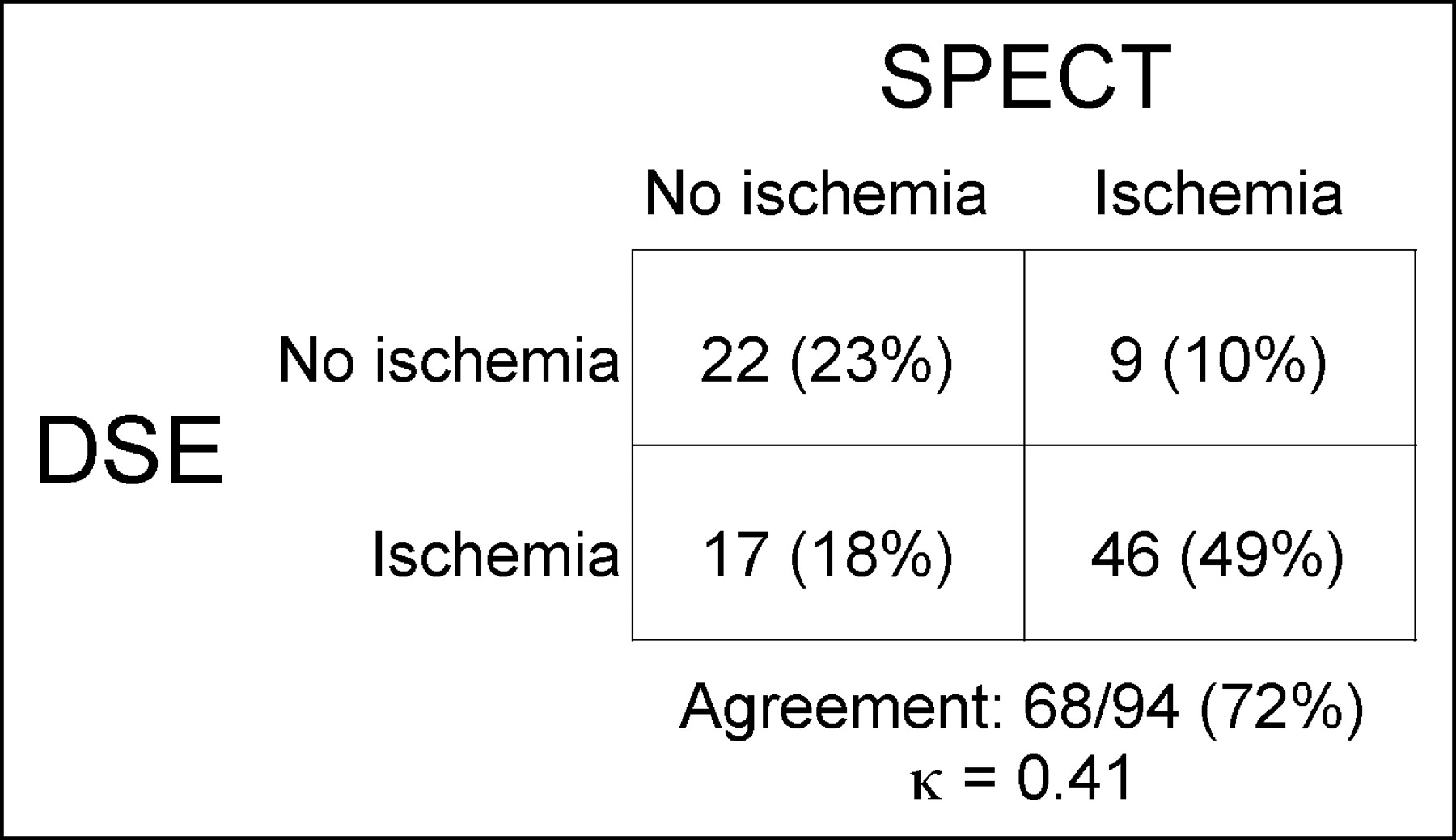
Concordance between myocardial perfusion SPECT and DSE for classification of patients as nonischemic or ischemic.
Coronary Territory Distribution for Regions with Myocardial Ischemia at Stress Myocardial Perfusion Imaging and DSE
Myocardial Ischemia and Outcome
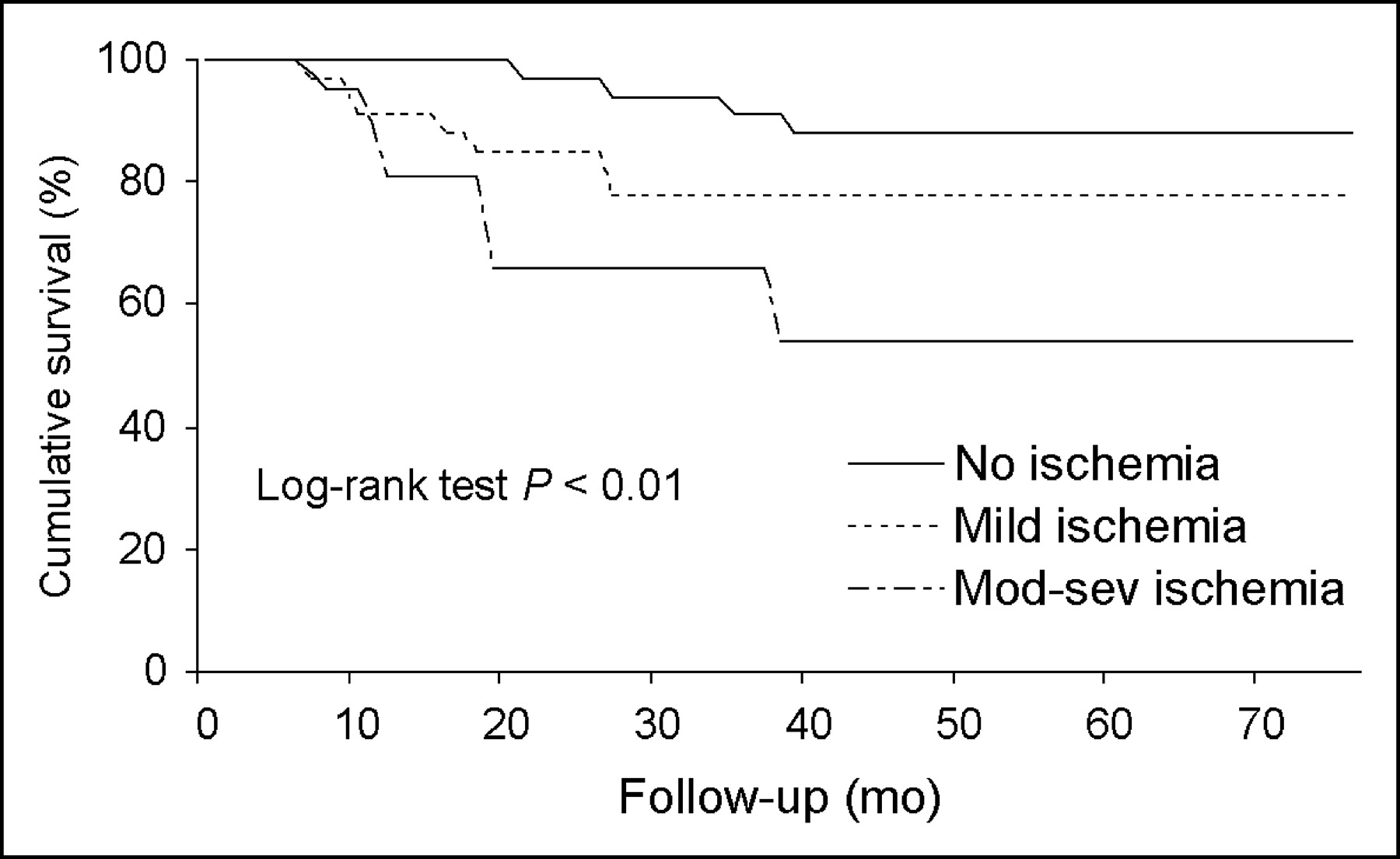
At Cox univariate analysis, the presence of myocardial ischemia at SPECT was a significant predictor of cardiac events (hazards ratio = 4.8; 95% confidence interval, 1.4–16.3; P < 0.01; C index of 0.70). In particular, cardiac events occurred in 17 (31%) of the 55 patients with ischemia at SPECT and in 3 (8%) of the 39 patients without ischemia. Event-free survival curves in patients with and without ischemia at SPECT are illustrated in Figure 2. Considering not only the presence but also the extent and severity of ischemia at SPECT, the cumulative probability of event-free survival was 88% in patients without ischemia, 78% in patients with mild ischemia, and 54% in those with moderate-to-severe ischemia (Fig. 3).

Event-free survival curves by Kaplan–Meier analysis in patients without or with ischemia at myocardial perfusion SPECT. Numbers of patients available for follow-up at 0, 10, 20, 30, 40, 50, and 60 mo were, respectively, 39, 39, 38, 31, 29, 17, and 10; and 55, 51, 42, 33, 26, 22, and 11.

Event-free survival curves by Kaplan–Meier analysis in patients without ischemia and in those with mild or moderate-to-severe ischemia at myocardial perfusion SPECT. Numbers of patients available for follow-up at 0, 10, 20, 30, 40, 50, and 60 mo were, respectively, 39, 39, 38, 31, 29, 17, and 10; 34, 31, 28, 19, 18, 14, and 5; and 21, 20, 14, 14, 8, 8, and 6. Mod-sev = moderate to severe.
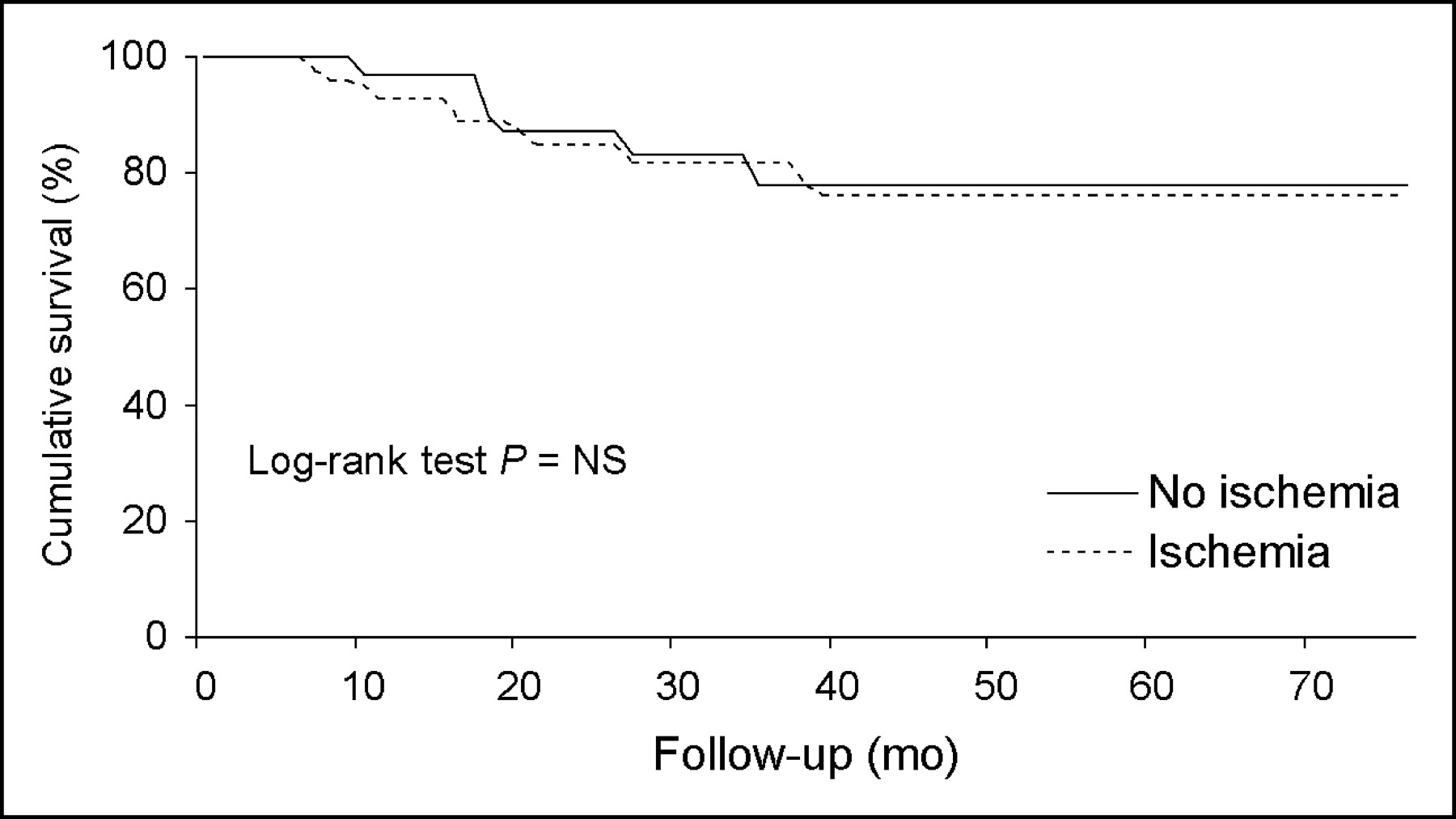
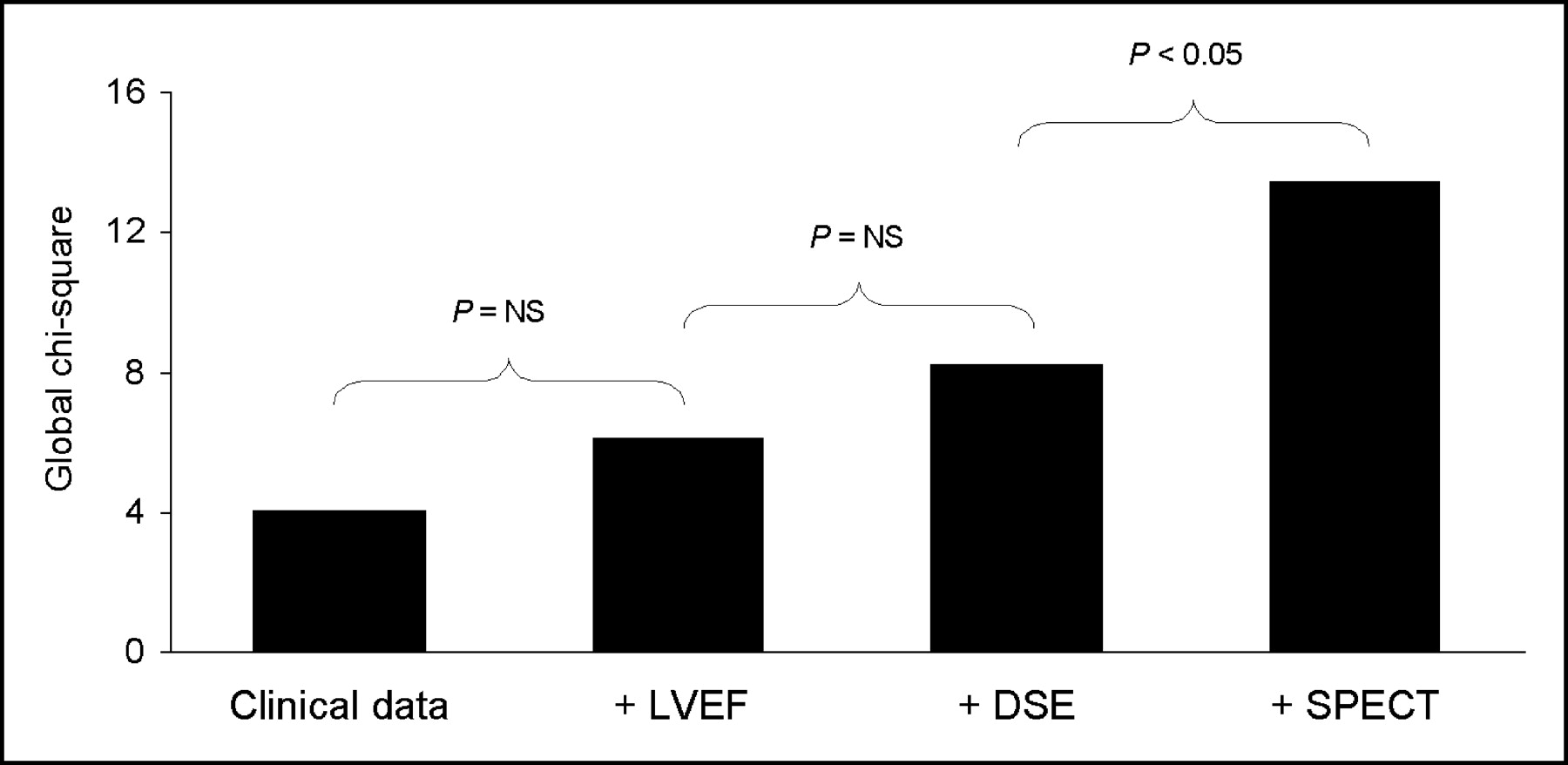
The presence of ischemia detected at DSE (biphasic or worsening patterns) was not associated with events (hazards ratio = 0.88; 95% confidence interval, 0.34–2.28; P = 0.78; C index 0.52). In fact, 14 (22%) of the 63 patients with ischemia and 6 (19%) of the 31 patients without ischemia experienced cardiac events. However, a biphasic pattern was a univariate predictor of events (hazards ratio = 3.29; 95% confidence interval, 1.3–8.3; P < 0.01). Event-free survival curves were similar in patients with and without ischemia at DSE (Fig. 4). Among patients with ischemia at DSE, a biphasic pattern was associated with a lower event-free survival as compared with a direct worsening pattern (56% and 83%, respectively; P < 0.05) (Fig. 5). At Cox multivariate analysis, only the presence of myocardial ischemia at SPECT was an independent significant predictor of events (hazards ratio = 3.81; 95% confidence interval, 1.05–13.9; P < 0.05). The incremental prognostic value of variables added sequentially is depicted in Figure 6. As shown, the addition of SPECT data to clinical variables, left ventricular ejection fraction, and DSE increased the global χ2 of this model from 6.2 to 13.4 (P < 0.005).
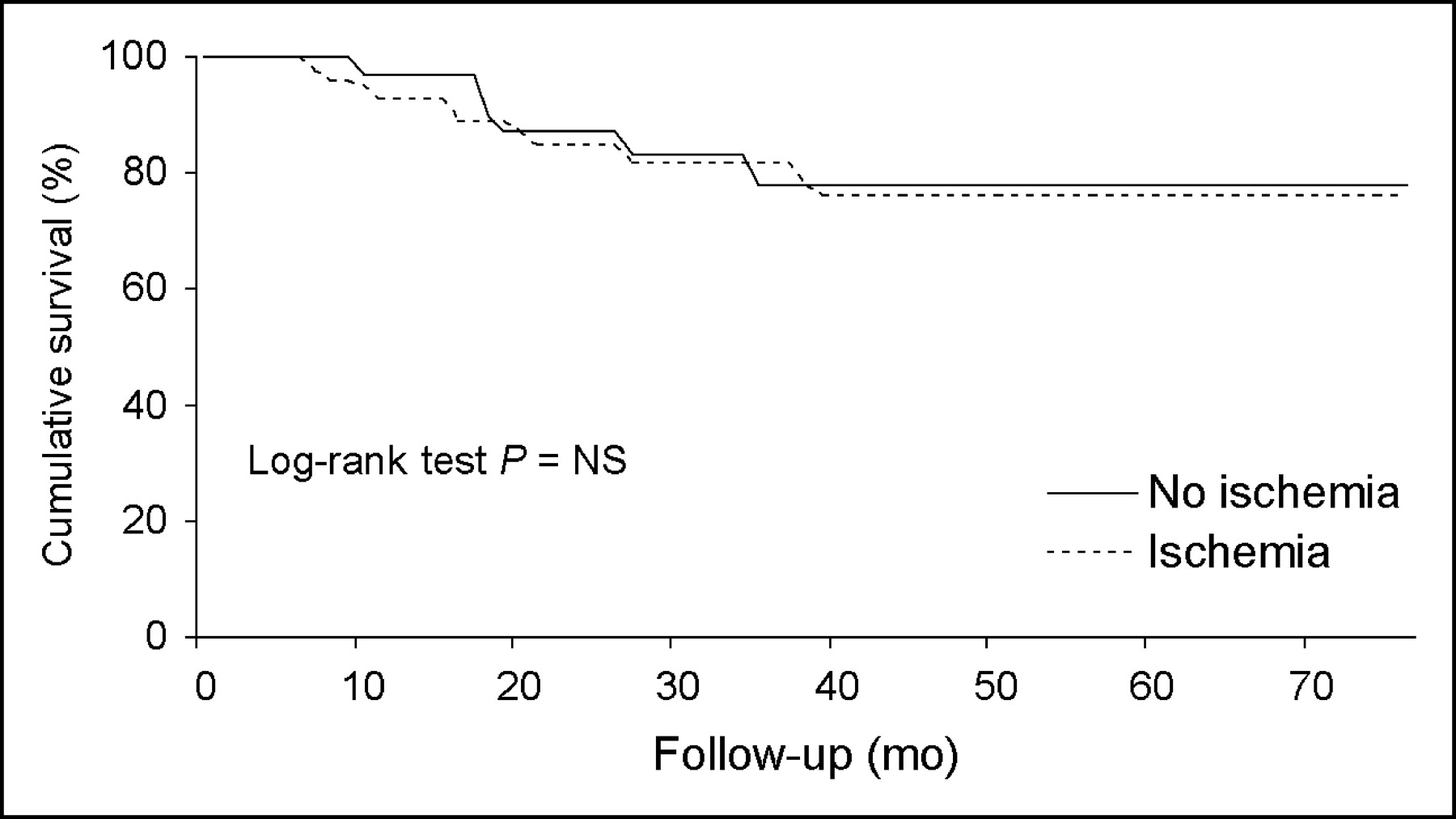
Event-free survival curves by Kaplan–Meier analysis in patients without or with myocardial ischemia at DSE. Numbers of patients available for follow-up at 0, 10, 20, 30, 40, 50, and 60 mo were, respectively, 31, 30, 26, 19, 18, 11, and 4; and 63, 60, 54, 45, 37, 28, and 17. NS = not significant.

Event-free survival curves by Kaplan–Meier analysis in patients with worsening or biphasic patterns at DSE. Numbers of patients available for follow-up at 0, 10, 20, 30, 40, 50, and 60 mo were, respectively, 47, 45, 45, 36, 31, 24, and 13; and 16, 15, 9, 9, 6, 4, and 4.

Incremental prognostic value for cardiac events (global χ2 values on y-axis) obtained considering in hierarchical order: clinical data; clinical data and left ventricular ejection fraction (LVEF); clinical data, LVEF, and DSE; clinical data, LVEF, DSE, and SPECT. NS = not significant.
In the 26 patients with discordant imaging results, the incidence of events was significantly higher in the 9 patients with myocardial ischemia at SPECT as compared with the 17 patients with ischemia at DSE (44% and 6%, respectively; P < 0.01). The cumulative probability of event-free survival was 94% in the 17 patients with ischemia only at DSE and 55% in the 9 patients with ischemia only at SPECT (P < 0.01) (Fig. 7).
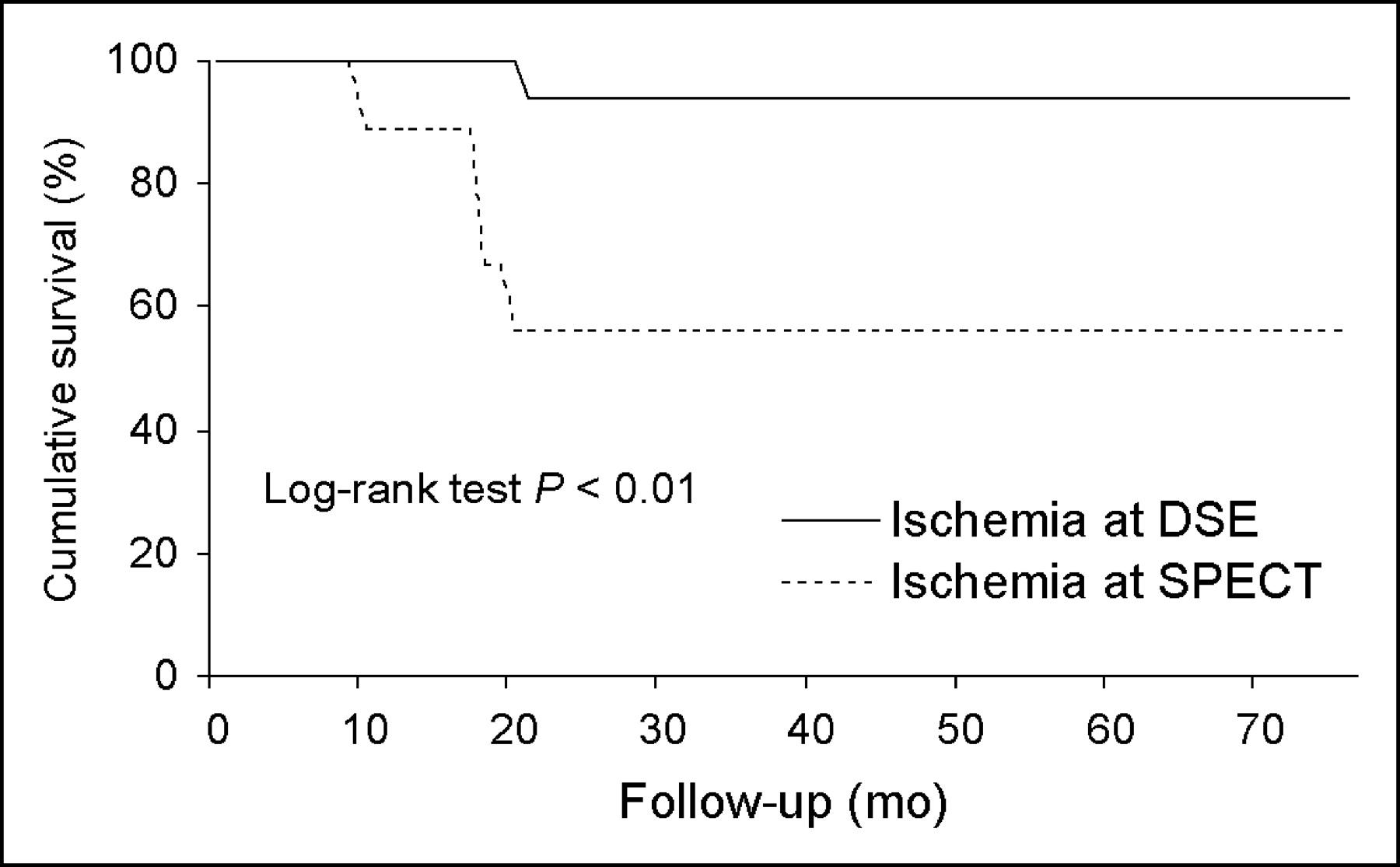
Event-free survival curves by Kaplan–Meier analysis in patients with ischemia and discordant results between myocardial perfusion DSE and SPECT. Numbers of patients available for follow-up at 0, 10, 20, 30, 40, 50, and 60 mo were, respectively, 17, 17, 17, 15, 14, 9, and 6; and 9, 8, 5, 3, 3, 3, and 0.
DISCUSSION
To our knowledge, this is the first study evaluating the comparative long-term prognostic power of DSE and SPECT myocardial perfusion imaging in patients with uncomplicated acute myocardial infarction and relatively preserved left ventricular function undergoing both imaging modalities during the same stress test. The results indicate that in these patients the presence of myocardial ischemia at SPECT is associated with an increased risk of cardiac events at long-term follow-up. In addition, not only the presence but also the extent and severity of ischemia at SPECT provide prognostic information. Differently from myocardial perfusion imaging, myocardial ischemia at DSE was unable to stratify patients after myocardial infarction and only the presence of a biphasic response was associated with a poor outcome.
Previous studies directly compared the prognostic value of stress echocardiography and SPECT in the same patient population with suspected or known coronary artery disease (14,15,20–22). Olmos et al. (14) reported that exercise echocardiography and exercise 201Tl imaging provide comparable prognostic information and can be used interchangeably for risk stratification. However, Hoque et al. (15) found that a moderate-to-large amount of ischemia by echocardiography was a better predictor of cardiac death, whereas a moderate-to-large fixed defect by SPECT was better for the prognosis of ischemic events, such as myocardial infarction or unstable angina. These authors concluded that stress echocardiography and nuclear imaging results might not be interchangeable for the long-term prediction of a specific cardiac event (15). Geleijnse et al. (20) showed that DSE and sestamibi SPECT provide comparable prognostic information in patients with suspected myocardial ischemia. However, SPECT added prognostic information in patients with nondiagnostic echocardiographic studies (20). Pasquet et al. (21) compared the ability of dipyridamole stress SPECT and echocardiography to predict perioperative and long-term cardiac events in patients referred for vascular surgery and found that the sensitivity of SPECT for the prediction of early events was 90% and that of echocardiography was 60%. Schinkel et al. (22) found a comparable long-term prognostic value of DSE and SPECT in patients with suspected or known coronary artery disease who were unable to exercise. Only one study directly compared the prognostic value of dipyridamole echocardiography and SPECT in patients after uncomplicated myocardial infarction (23), a population similar to that of the present study. The authors reported the limited value of the dipyridamole stress test in predicting events in this setting of patients, with both imaging techniques (23). In the present study, we enrolled only patients with uncomplicated acute myocardial infarction and the stress test was performed by dobutamine infusion. In survivors after acute myocardial infarction DSE is a useful technique, allowing the identification of myocardial ischemia and the detection of myocardial viability in dysfunctional areas (3,7,8). Several studies addressed the prognostic value of DSE in the setting of acute myocardial infarction (7,8,24–26). Spinelli et al. (26) demonstrated that an inotropic response to low-dose dobutamine was the best predictor of segmental and global functional improvement in medically treated patients, whereas sestamibi imaging was useful to identify patients with dysfunctional myocardium without contractile reserve that may benefit by coronary revascularization. Bigi et al. (8) found that a biphasic pattern response, but not worsening, was a significant predictor of hard events in patients with acute myocardial infarction and mildly impaired left ventricular function. However, in that study, event-free survival was comparable in patients with ischemia only (i.e., worsening response) and in those with nonischemic response (8). Our findings confirm that patients with ischemic and nonischemic response at DSE have a similar long-term outcome and also underscore the prognostic value of a biphasic response in these patients. In particular, 15% of patients with a worsening pattern at DSE experienced cardiac events as compared with 44% of those with a biphasic pattern (P < 0.01). These results support the concept that myocardial ischemia by DSE provides significant prognostic information only if associated with the presence of dysfunctional viable tissue (27). On the other hand, a direct worsening pattern reflects the imbalance between myocardial oxygen demand and supply in a normal or mildly dysfunctional region (28). According to previous findings (8,27) and our results, in patients with uncomplicated acute myocardial infarction and mildly impaired left ventricular function, the prevalence of a biphasic response pattern at DSE is relatively low (∼15%), whereas most patients exhibit direct worsening (∼45%). Therefore, DSE may have a limited prognostic value in this subset of patients. Accordingly, in our study, at Cox multivariate analysis, the presence of myocardial ischemia at SPECT but not a biphasic pattern at DSE was a significant independent predictor of events (P < 0.01). It is conceivable that the superior prognostic value of SPECT compared with DSE is related to the direct capability of this technique to identify an ischemic area (28).
Previous studies demonstrated that stress echocardiography is more specific but less sensitive than SPECT for the detection of coronary artery disease (3,4). In the present investigation, ischemia was detected in a higher number of patients by DSE compared with SPECT. However, we considered as having ischemia not only patients with worsening but also those with a biphasic response.
Among the patients with discordant results, 65% had myocardial ischemia at DSE but not at SPECT and 35% had ischemia at SPECT but not at DSE. In these patients, there was a higher event rate in those with an ischemic response at SPECT compared with those with ischemic patterns at DSE. These findings may be explained by 2 different mechanisms. First, augmented contraction at maximal dobutamine depends not only on increased myocardial blood flow but also on tethering, resulting in overestimation of ischemia by DSE (29,30). In addition, regions with persistent akinesia and reversible defects at SPECT may represent a hibernating myocardium unresponsive to dobutamine or a necrotic myocardium with a small amount of viable, ischemic myocardium, resulting in reversible hypoperfusion yet incapable of demonstrating a contractile response at DSE (27).
The present study has some potential limitations that should be considered. The relatively small number of patients did not allow for separate evaluation of cardiac death and nonfatal myocardial infarction. The stress test was performed by dobutamine, which is not the optimal stress technique for radionuclide imaging. This approach represents the usual pharmacologic provocative test in patients with recent myocardial infarction when echocardiography is used. Finally, gated SPECT data were not available in all patients and, therefore, were not considered for the purpose of the present investigation. However, in a previous study we demonstrated that, in patients with recent infarction, gated SPECT provides incremental information to a dobutamine stress test and it is useful to estimate risk for subsequent cardiac events (11).
CONCLUSION
The detection of stress-induced myocardial ischemia at SPECT is useful for long-term risk stratification of patients with uncomplicated acute myocardial infarction and relatively preserved left ventricular function. In these patients, the predictive value of SPECT myocardial perfusion imaging is superior to that of DSE.
Footnotes
Received July 29, 2004; revision accepted Oct. 21, 2004.
For correspondence or reprints contact: Alberto Cuocolo, MD, Department of Biomorphological and Functional Sciences, University Federico II, Via S. Pansini, 5, I-80131 Napoli, Italy.
E-mail: cuocolo{at}unina.it.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}