


Abstract
Recent reports have indicated the value and limitations of 18F-FDG PET and 201Tl SPECT for determination of malignancy. We prospectively assessed and compared the usefulness of these scintigraphic examinations as well as 18F-FDG PET delayed imaging for the evaluation of thoracic abnormalities. Methods: Eighty patients with thoracic nodular lesions seen on chest CT images were examined using early and delayed 18F-FDG PET and 201Tl-SPECT imaging within 1 wk of each study. The results of 18F-FDG PET and 201Tl SPECT were evaluated and compared with the histopathologic diagnosis. Results: Fifty of the lesions were histologically confirmed to be malignant, whereas 30 were benign. On 18F-FDG PET, all malignant lesions showed higher standardized uptake value (SUV) levels at 3 than at 1 h, and benign lesions revealed the opposite results. Correlations were seen between 18F-FDG PET imaging and the degree of cell differentiation in malignant tumors. No significant difference in accuracy was found between 18F-FDG PET single-time-point imaging and 201Tl SPECT for the differentiation of malignant and benign thoracic lesions. However, the retention index (RI) of 18F-FDG PET (RI-SUV) significantly improved the accuracy of thoracic lesion diagnosis. Furthermore, 18F-FDG PET delayed imaging measuring RI-SUV metastasis was useful for diagnosing nodal involvement and it improved the specificity of mediastinal staging. Conclusion: No significant difference was found between 18F-FDG PET single-time-point imaging and 201Tl SPECT for the differentiation of malignant and benign thoracic lesions. The RI calculated by 18F-FDG PET delayed imaging provided more accurate diagnoses of lung cancer.
Conventional radiologic assessment (chest radiography, CT, MRI) of thoracic abnormalities is being complemented by PET, which is becoming known as a powerful tool. In the thorax, PET has been used to evaluate tumor imaging. 18F-FDG, a d-glucose analog labeled with 18F used as a radiopharmaceutical, is ideally suited for tumor imaging (1,2). Many reports have indicated that 18F-FDG PET is sensitive and specific for the diagnosis and staging of several types of malignancies (3–5); however, 18F-FDG accumulation is not specific to malignancies because there are numerous causes of 18F-FDG uptake in benign processes (6–8). As the result, increased 18F-FDG uptake in lesions such as benign tumors or inflammatory processes leads to false-positive results and misdiagnoses of malignancies (9, 10). It has also been reported that 201Tl accumulations on SPECT differ between benign and malignant tumors (11,12). 201Tl SPECT is often used for the evaluation of malignancies because it is more cost efficient and more widely available than 18F-FDG PET. Furthermore, 201Tl accumulation is seen in malignant tumors on both early and delayed scans; however, it is not seen on delayed scans in the case of benign tumors. Therefore, retention of 201Tl on a delayed scan is strongly suggestive of malignancy (13).
Various cell types exhibit varying rates of 18F-FDG uptake and metabolism, and we hypothesized that measurements at 2 time points may prove to be helpful in differentiating malignant from benign diseases and that 18F-FDG PET is superior to 201Tl SPECT in terms of disease specificity. Therefore, we tested our hypothesis by assessing the results of dual-time-point 18F-FDG PET imaging. Furthermore, we performed a comparison of 18F-FDG PET and 201Tl SPECT in patients with thoracic abnormalities to validate the usefulness of 18F-FDG PET delayed imaging.
MATERIALS AND METHODS
Subjects
We studied 80 patients (49 men, 31 women; age range, 23–80 y; mean age, 65.0 ± 11.9 y) with thoracic abnormalities suspected to be thoracic malignancy—that is, lung cancer—on the basis of chest CT results. All patients underwent preoperative 18F-FDG PET and 201Tl SPECT examinations between October 1998 and April 2002, and the respective studies were completed within 1 wk of each other. All patients underwent a thoracotomy, open lung biopsy, or lung biopsy using video-assisted thoracoscopic surgery within 4 wk of the 18F-FDG and 201Tl examinations. All lesions were removed completely and examined histologically. Three patients with abnormal pulmonary shadows that disappeared or were reduced before surgery were diagnosed as having organizing pneumonia on the basis of results of a transbronchial lung biopsy and clinical follow-up. Another 3 patients were diagnosed with mycobacterial infection on the basis of positive results of a bacteriologic examination through bronchial lavage and clinical follow-up. All cases of tuberculosis and all designators of mycobacteria were proven by bacteriologic examination. Informed consent was obtained from all patients participating in the study.
18F-FDG PET
18F-FDG PET imaging was performed using a whole-body scanner (ADVANCE; General Electric Medical Systems, Milwaukee, WI). After at least 4 h of fasting, each subject underwent transmission scanning for attenuation correction for 10 min. Immediately after obtaining the transmission scan, 370 MBq 18F-FDG were intravenously administered, and static scans were obtained 1 h later for 10 min and 3 h later for 20 min. Only 1 preinjection transmission scan was acquired. In each emission scan, the patient’s body was carefully positioned with the guidance of a laser beam so that misregistration should not occur. Images were then reconstructed and viewed as transaxial slices of the chest and coronary slices of the whole body, with a slice thickness of 7 mm. Between the early and delayed scans, patients returned to their hospital room and waited quietly. CT was performed on all patients before 18F-FDG PET. On the basis of this information and the transmission scan, we can ensure that the tumor is in the field of view. 18F-FDG and 201Tl images were interpreted visually from the films and correlated carefully with the CT results at the same time. For qualitative analysis, any obvious foci of increased 18F-FDG or 201Tl uptake over the background were considered positive for a tumor. For semiquantitative analysis of the 18F-FDG uptake, a standardized uptake value (SUV) (tumor activity concentration/injected dose/body weight) measurement was obtained at the most active tumor site by drawing a region of interest (ROI) around the lesion that encompassed all pixels with uptake values of >90% of the maximum uptake in the transaxial slice, after which the average counting rate in each ROI was calculated. The SUV was calculated using a calibration factor between PET counts and radioactivity concentration. Primary lung lesions with an SUV of <2.5 or undetectable in early imaging and delayed imaging were considered benign. Furthermore, we calculated the retention index (RI-SUV) from the results of 1-h (early scan) and 3-h (delayed scan) imaging according to the following equation: RI-SUV (%) = (SUV [delayed scan] − SUV [early scan]) × 100/SUV (early scan). If the RI (SUV) of 18F-FDG was positive, the thoracic lesion was considered to be malignant by the results of RI-SUV. To assess nodal disease, all pulmonary and mediastinal malignancies were analyzed visually and considered positive if the 18F-FDG accumulation had increased relative to that in the adjacent mediastinal and soft-tissue structures in the early imaging. Furthermore, the RI of positive lymph nodes was calculated according to delayed imaging, and, if positive, nodal involvement was considered positive in the delayed imaging (RI) study. Nodal (N) staging was diagnosed according to pathologic findings. The results of 18F-FDG PET were expressed from early imaging, delayed imaging, and RI results and then compared among them.
If the results of 18F-FDG PET can be positive for malignancy or negative for benign disease, we considered that they should be accurate diagnoses and calculated the accuracy from the ratio of total cases.
201Tl SPECT
All patients were examined by 201Tl SPECT within 1 wk of the PET study. With the subjects at rest, 111 MBq 201Tl-chloride were injected into a peripheral vein, and imaging was performed after 15 min (early scan) and 3 h (delayed scan). SPECT was performed using a rotating gamma-camera system (GCA-9300A/HG; Toshiba, Tokyo, Japan) with a slice thickness of 5.8 mm. For semiquantative analysis of 201Tl SPECT, an ROI was defined manually on transaxial tomograms that showed the highest uptake of the lesion to be in the middle of the tumor. The ROI placed on the lesion encompassed all pixels that had uptake values of >90% of the maximum uptake in that slice, and the average counting rate in each ROI was calculated. Radioactivity was also measured for areas of the homologous contralateral normal lung to calculate the tumor-to-normal lung ratio (T/N) of the activity on early scans (early ratio [ER]) and on delayed scans (delayed ratio [DR]). The RI of 201Tl was also calculated for tumor activity according to the following equation: RI-Tl (%) = (DR-ER) × 100/ER.
If the RI of 201Tl was positive, the thoracic lesion was considered to be malignant, whereas all undetectable cases were considered benign. 201Tl SPECT images of all pulmonary and mediastinal malignancies were classified as positive for nodal involvement when there was at least 1 area of definitely increased radioactivity in the mediastinum, other than areas in the myocardium and thoracic spine. When there was no uptake of 201Tl in the mediastinum or when the accumulation was equivocal or could not be distinguished from that in the myocardium or vertebra, the images were considered negative (12). We also assessed the clinical accuracy compared with the pathologic diagnosis.
Thoracic CT
CT scans were obtained using a helical CT system (HiSpeed Advantage RP; General Electric Medical Systems). Contiguous 1-cm-thick sections were obtained at 1-cm intervals from the lung apices to the adrenal glands before and during intravenous bolus injection of contrast material at 2 mL/s by a power injector. Results of nodal staging were classified as either positive or negative on the basis of the presence or absence of mediastinal node enlargement, which was defined as a node of >1 cm in short-axis diameter on transaxial images. Results of the scans were correlated with the pathologic diagnosis.
Radiographic images were interpreted independently and prospectively by experienced radiologists and nuclear medicine physicians, without knowledge of histopathologic or other radiologic data.
Statistical Analysis
Results of 18F-FDG (uptake, RI) and 201Tl (uptake, RI) are expressed as mean ± SD. Differences in 18F-FDG uptake between the early (1 h) and delayed images (3 h), as reflected by SUV levels, were examined for statistical significance using the Wilcoxon signed rank test. Comparisons of differences between the results of 18F-FDG (SUV level, RI) or 201Tl uptake (T/N ratio, RI) were performed with 1-way ANOVA using the Fisher protected least-significant difference (PLSD). The diagnostic accuracy of PET and 201Tl SPECT was compared by a McNemar test. Any correlation between the 2 variables was analyzed with the Pearson coefficient of correlation. P < 0.05 was considered to be statistically significant.
RESULTS
Subject Demography and Clinical Characteristics
All malignancies (50 cases) and benign lesions (24 cases) were histologically confirmed by surgical resection. Three patients with abnormal pulmonary shadows that disappeared or were reduced before surgery were diagnosed as having organizing pneumonia on the basis of results of a transbronchial lung biopsy and clinical follow-up. Another 3 patients were diagnosed with a mycobacterial infection on the basis of positive results of a bacteriologic examination through bronchial lavage and clinical follow-up. The thoracic lesions ranged in size from 11 to 60 mm, with most lesions < 30 mm in diameter. The radionuclide examination results and diagnoses for the 80 thoracic lesions are summarized in Table 1.
Patient Characteristics
18F-FDG PET and 201Tl SPECT in Thoracic Lesions
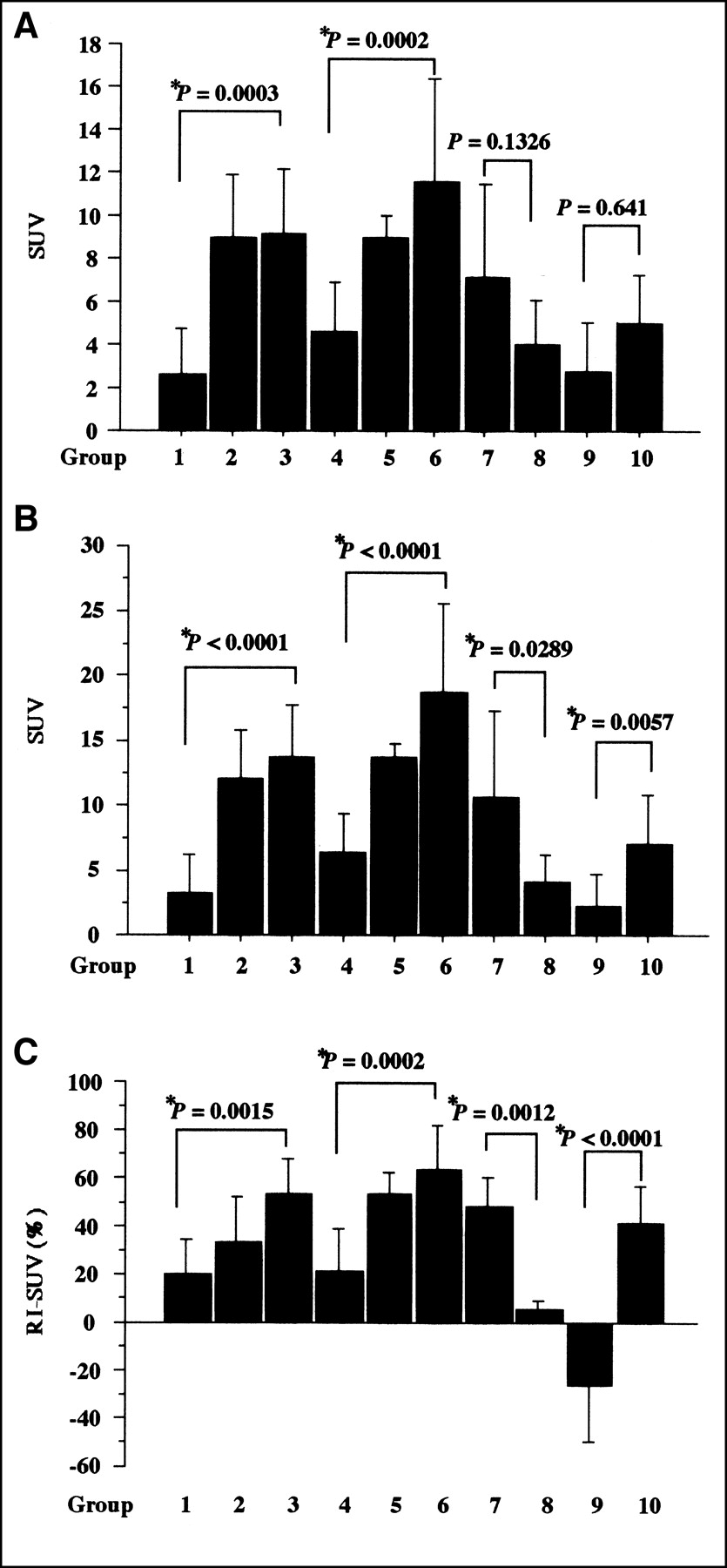
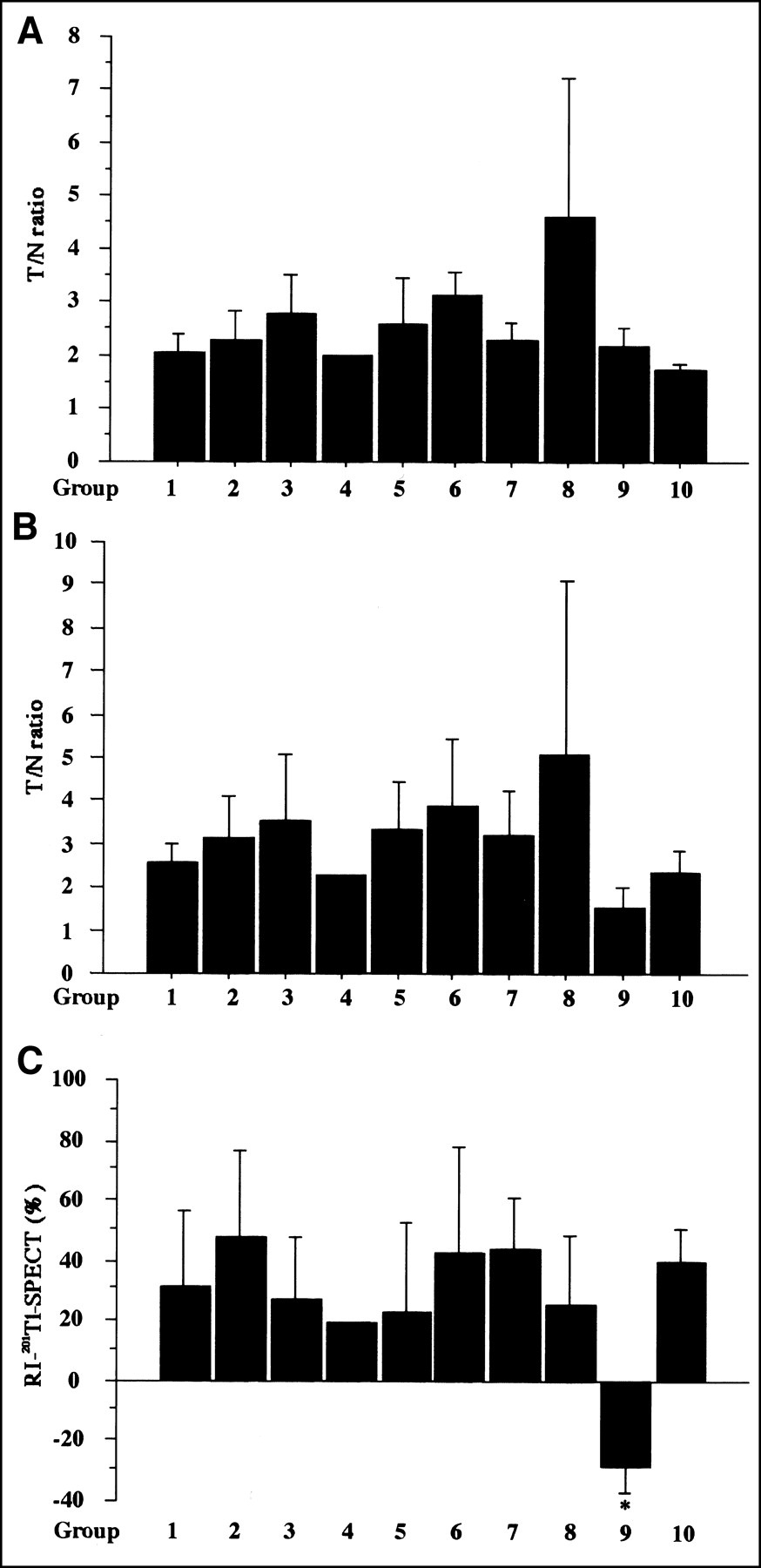
We observed all malignant tumors (malignant disease group) that exhibited a higher SUV level at 3 than at 1 h (Fig. 1A) (P < 0.0001, analyzed by Wilcoxon signed rank test). Benign lesions, with the exception of those with granulomatous disease (benign disease group), showed significantly lower SUV levels at 3 than at 1 h (Fig. 1B) (P = 0.0007, analyzed by Wilcoxon signed rank test), whereas all mycobacterial infections and 1 case of nodular sarcoidosis (granulomatous disease group) exhibited a higher SUV level at 3 than at 1 h (Fig. 1C) (P = 0.0051, analyzed by Wilcoxon signed rank test). The correlation between SUV level (1 h, 3 h, and RI-SUV) and degree of cell differentiation in thoracic malignancies is seen in Figure 2. Furthermore, the SUV levels at 1 and 3 h of well-differentiated adenocarcinoma and well-differentiated squamous cell carcinoma were significantly lower than those of poorly differentiated adenocarcinoma (P = 0.0003 at 1 h and P = 0.0001 at 3 h, analyzed by the Fisher PLSD) and poorly differentiated squamous cell carcinoma (P = 0.0002 at 1 h and P < 0.0001 at 3 h, analyzed by the Fisher PLSD). RI-SUV results were the same. Moreover, undifferentiated carcinoma (small cell carcinoma and large cell carcinoma) had a higher index (RI-SUV) than low-grade malignant diseases (carcinoid and mucosa-associated lymphoid tissue lymphoma) (P = 0.0012, analyzed by the Fisher PLSD). Representative cases of 18F-FDG PET delayed imaging for differential diagnosis of well-differentiated adenocarcinoma are shown in Figure 3 and benign lesions are shown in Figure 4. In contrast, no significant differences were found among 201Tl ER, DR, and RI (Fig. 5).
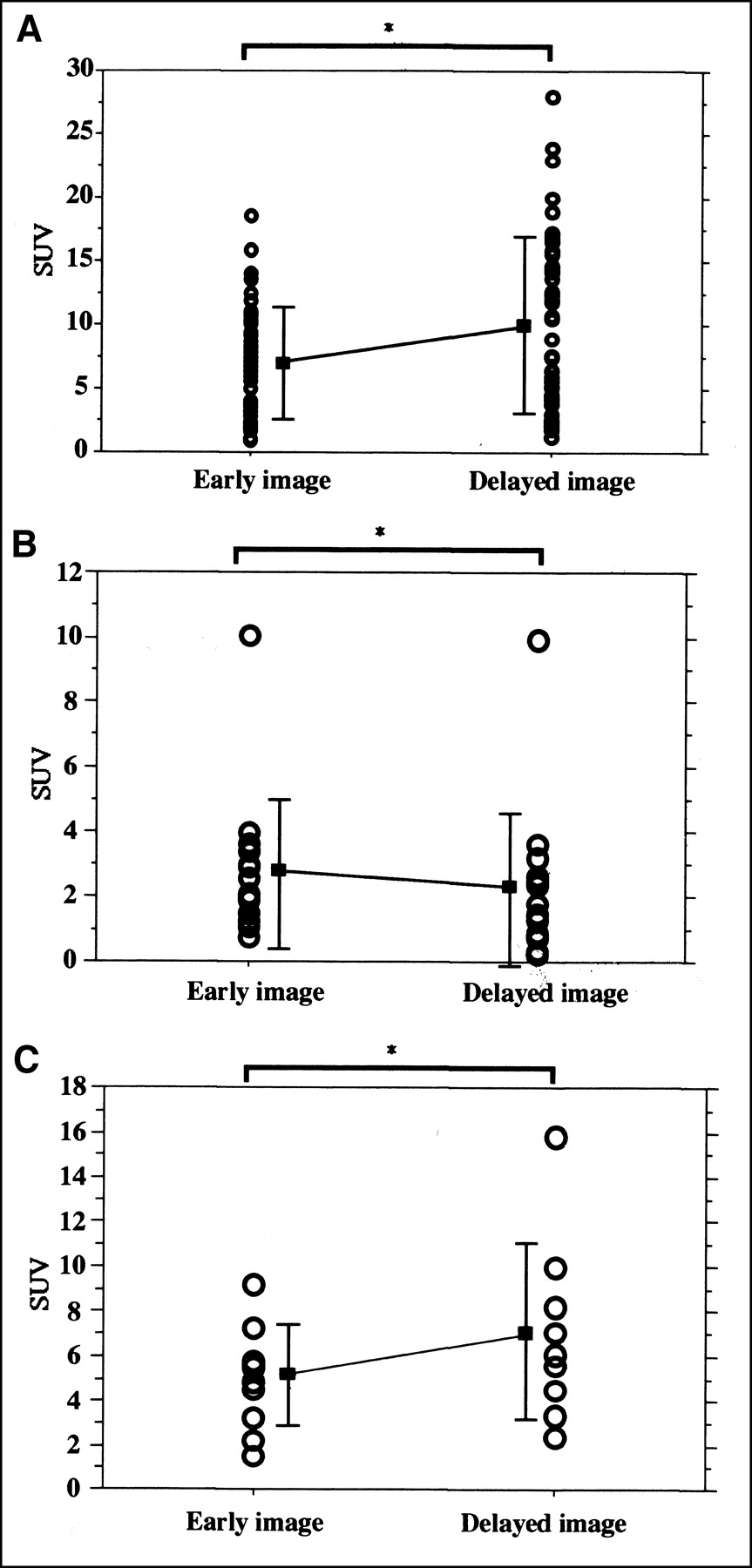
Changes in 18F-FDG accumulation (SUV) between early and delayed imaging in primary lesions of malignant lesion group (mostly lung cancer) (A), benign disease group (group 9) (B), and granulomatous disease group (group 10) (C). Significant increases of SUV in A and C and significant decrease of SUV in B were observed. Bars indicate mean ± SD. *P < 0.05.

Comparison of SUV levels with 18F-FDG PET. (A) Early imaging. (B) Delayed imaging. (C) RI in thoracic lesions. Significant correlations were observed between SUV levels and degree of cell differentiation in lung cancer. For adenocarcinoma, squamous cell carcinoma, and undifferentiated carcinoma, 18F-FDG accumulations in delayed images better reflected degree of cell differentiation than that in early images. For SUV RI, cell differentiation was better reflected and benign disease group (group 9) was significantly differentiated from other groups. Results are expressed as mean ± SD.
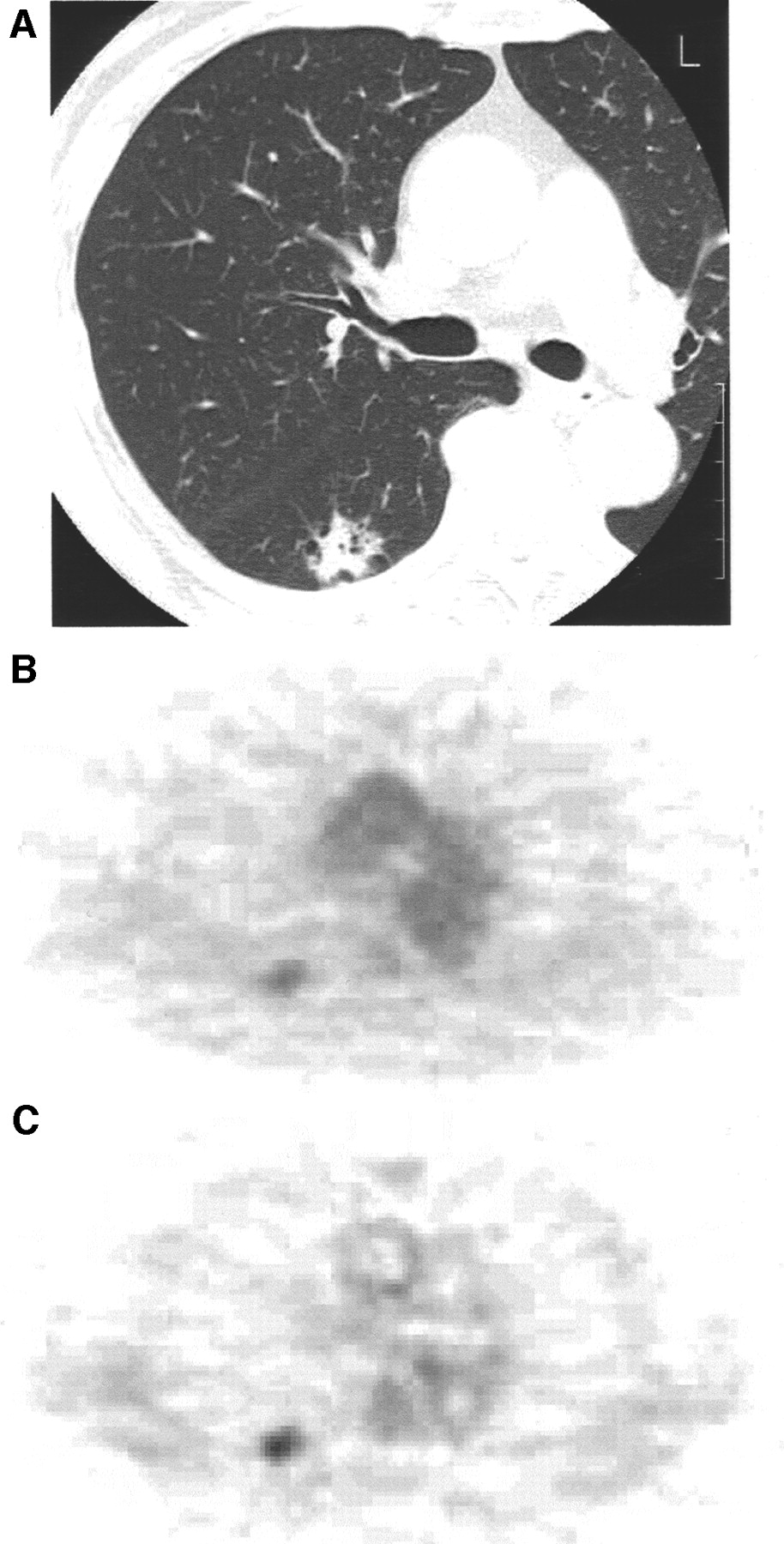
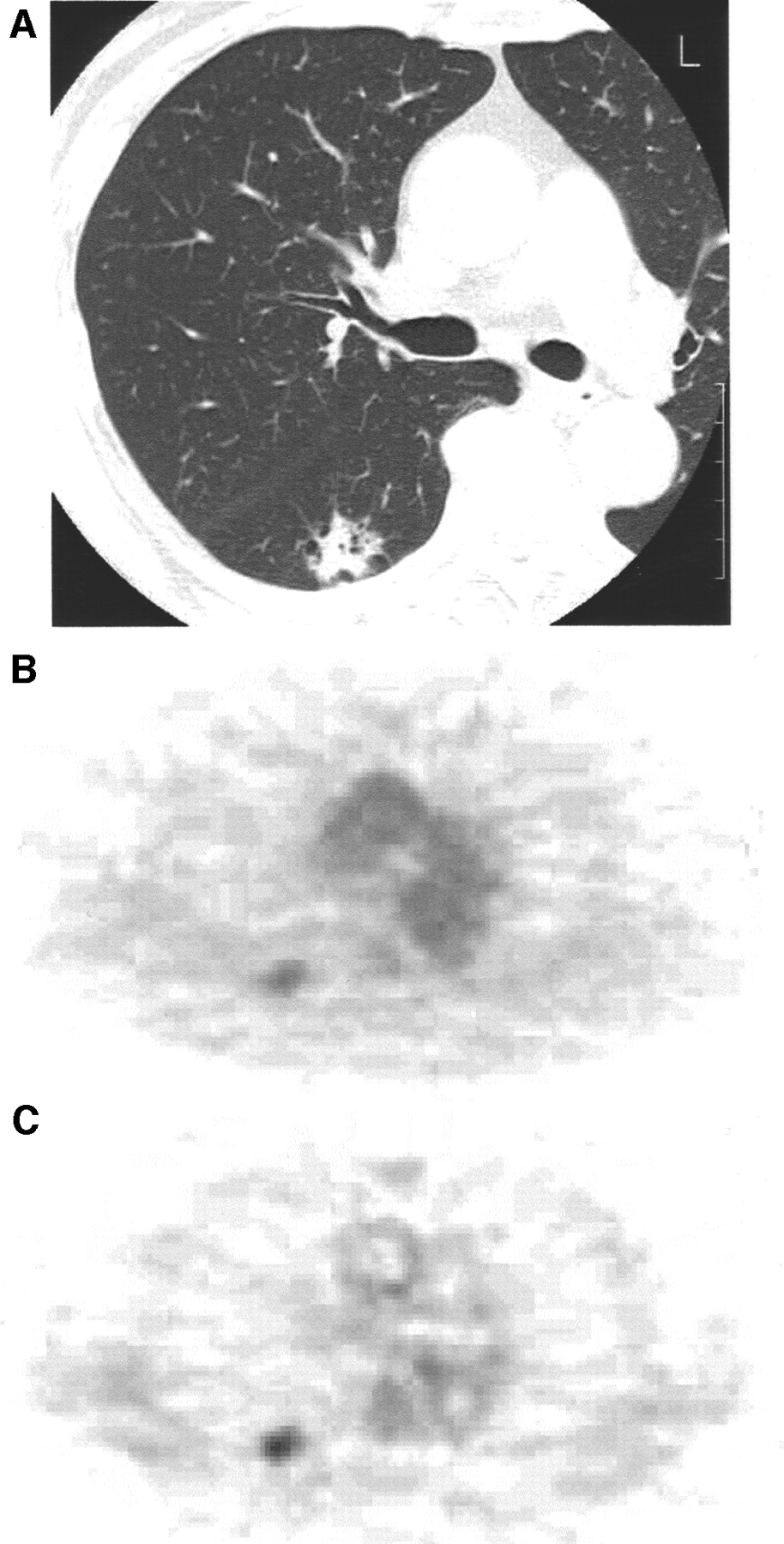
Patient with well-differentiated lung adenocarcinoma (2.2 × 2.0 cm). (A) CT image shows nodule in right lung. (B) 18F-FDG PET early image shows faint accumulation in nodule (SUV = 2.40). (C) 18F-FDG PET delayed image shows increased hot accumulation in nodule (SUV = 3.00) along with good visualization. Nodule was not detected by 201Tl SPECT (image not shown).
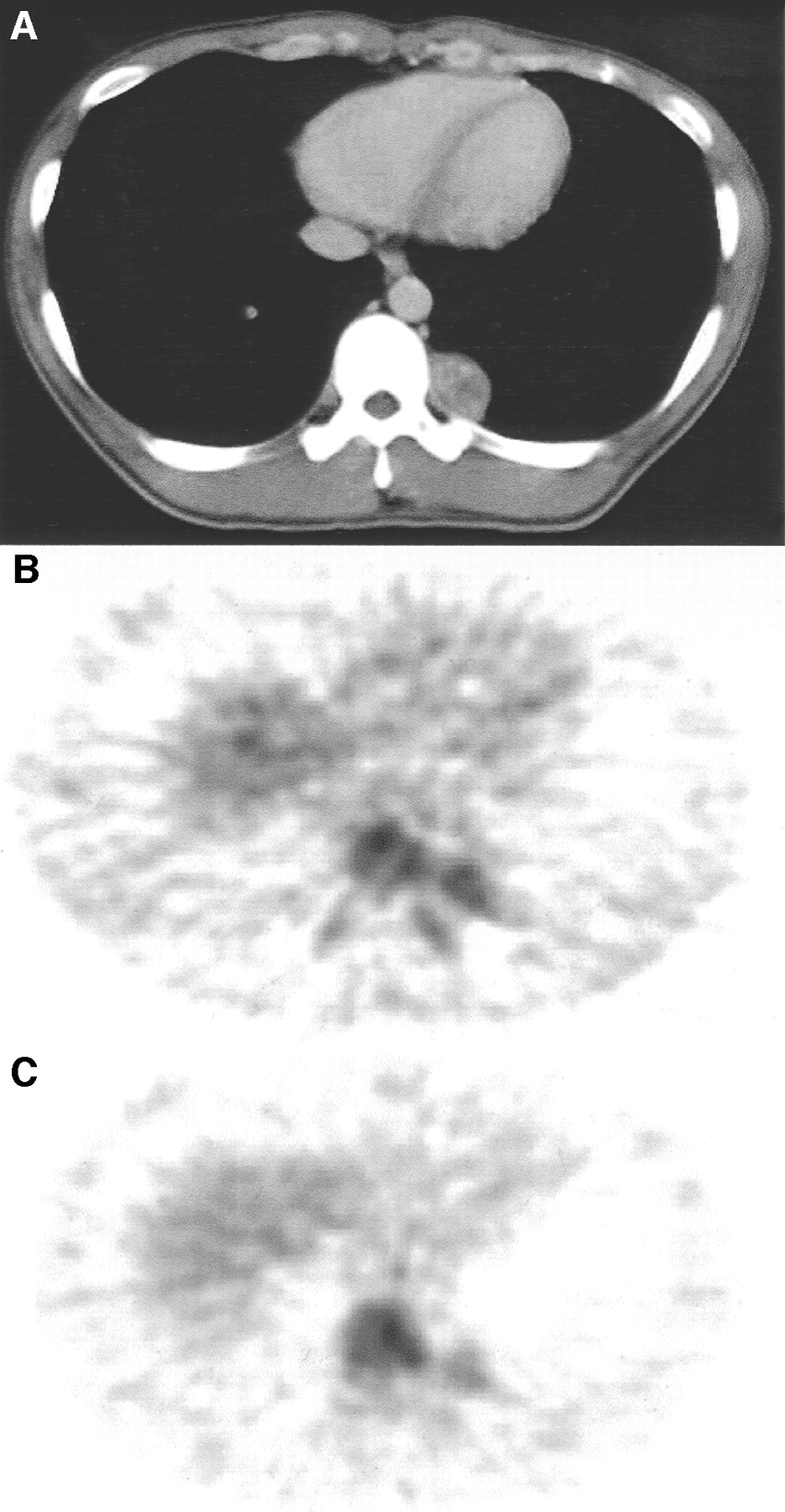
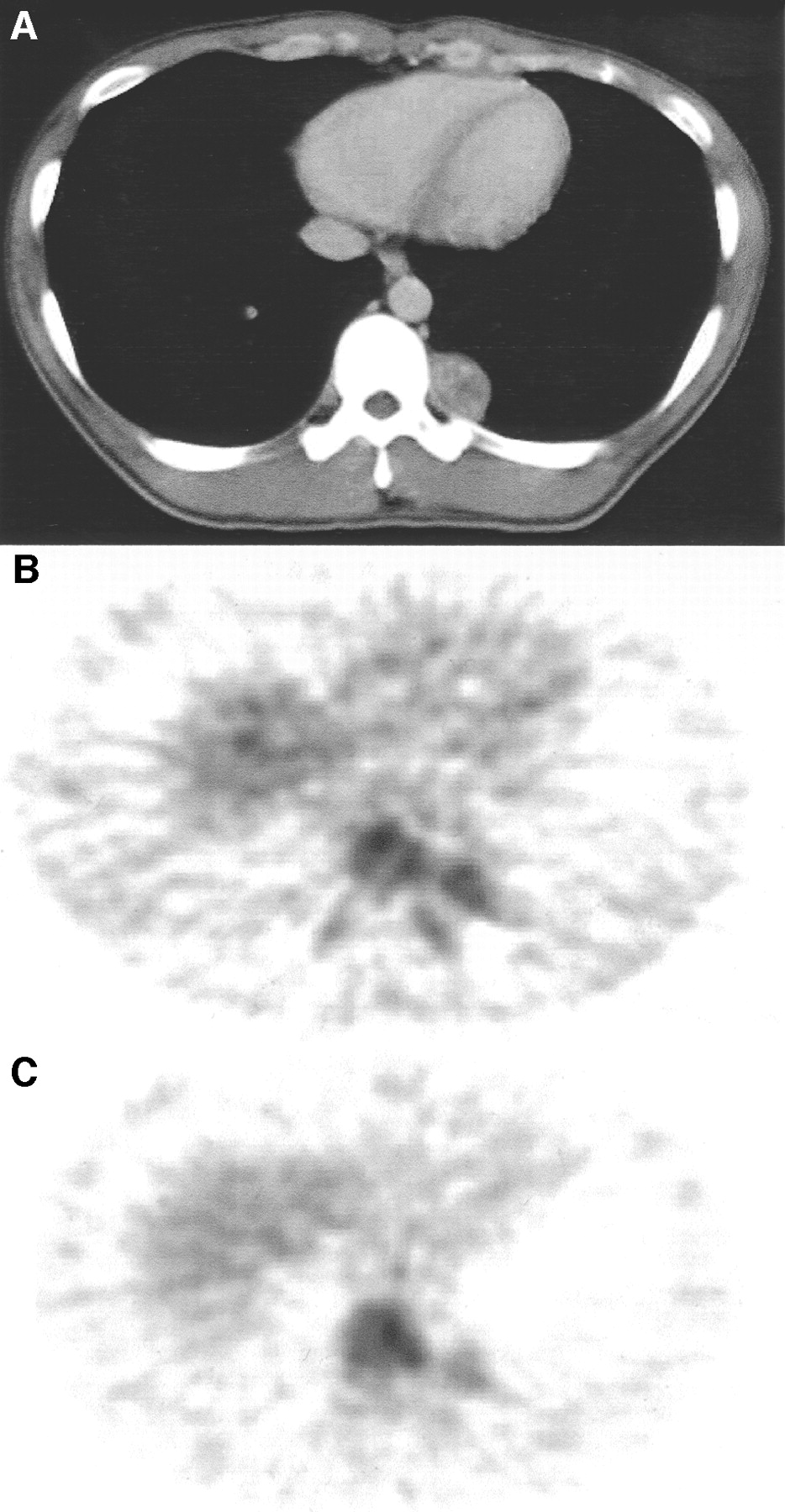
Patient with posterior mediastinal schwannoma (3.5 × 2.2 cm). (A) CT image shows nodule in left thorax. (B) 18F-FDG PET early image shows hot accumulation in nodule (SUV = 2.80). (C) 18F-FDG PET delayed image shows decreased hot accumulation in nodule (SUV = 1.70). Nodule was not detected by 201Tl SPECT (image not shown).
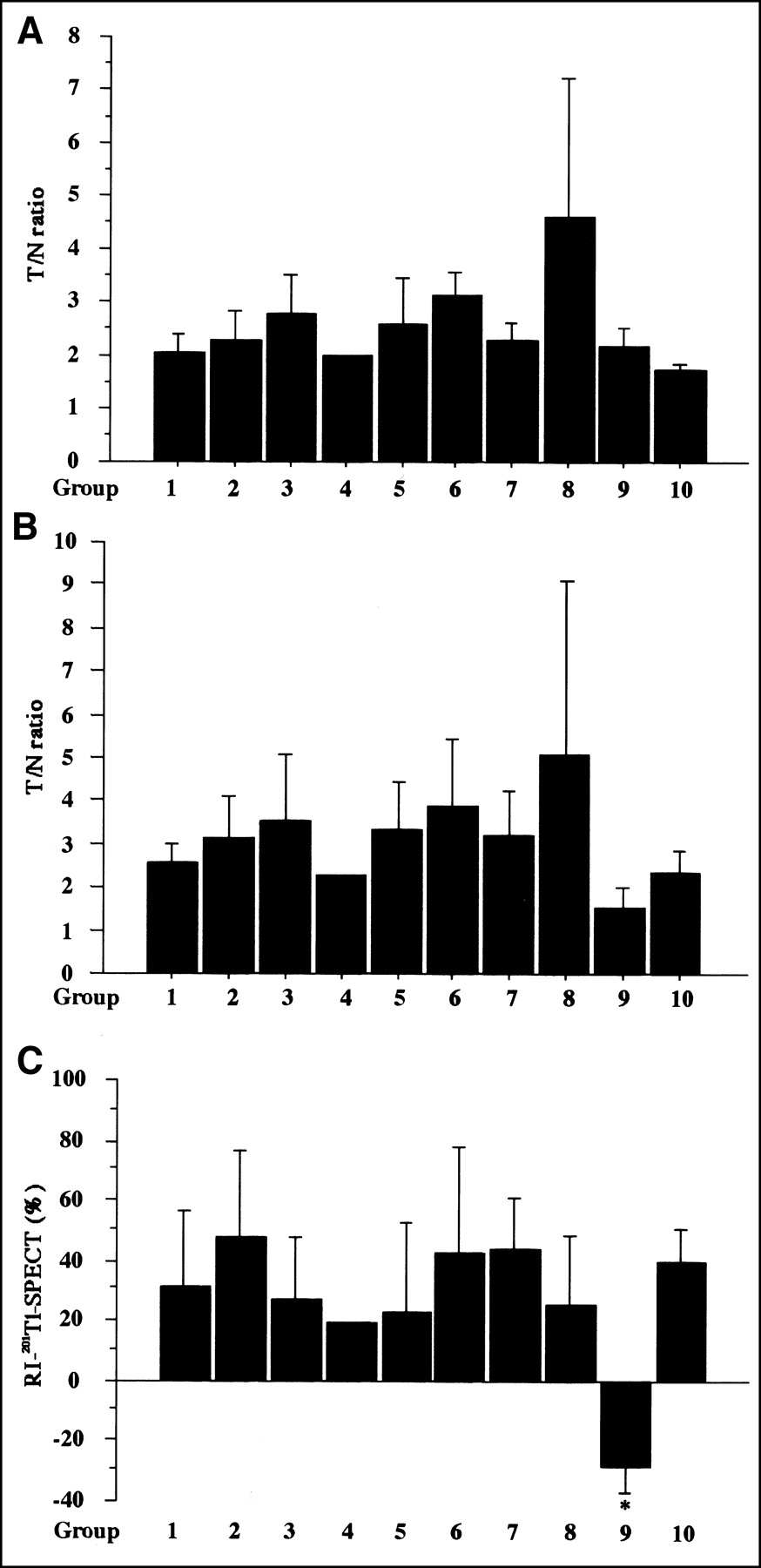
Comparison of results of 201Tl SPECT. (A) Early imaging. (B) Delayed imaging. (C) RI in thoracic lesions. No significant correlations were observed between results and degree of cell differentiation in lung cancer. As for RI of 201Tl SPECT, only benign disease group (group 9) was significantly differentiated from others. Results are expressed as mean ± SD. *P < 0.05 vs. other groups, excluding group 4.
The diagnostic values of 18F-FDG PET (early image, delayed image, and RI-SUV) and 201Tl SPECT were evaluated for thoracic lesions (Table 2). According to the results, 18F-FDG PET early image and delayed image and 201Tl SPECT showed no differences; however, RI-SUV was significantly superior in distinguishing a benign lesion from a malignant lesion in terms of accuracy (RI-SUV vs. 201Tl SPECT: P = 0.00558; RI-SUV vs. PET early image: P = 0.0001; RI-SUV vs. PET delayed image: P = 0.0005, analyzed by the McNemar test).
Comparison of 18F-FDG PET (Early Imaging, Delayed Imaging, and RI) and 201Tl SPECT Results for Diagnosis of Malignancy
18F-FDG PET and 201Tl SPECT in Diagnosis of Nodal Staging
In nodal staging, conventional 18F-FDG PET (early imaging) and 201Tl SPECT were more accurate than thoracic CT (Table 3), and 18F-FDG PET imaging showed excellent sensitivity compared with that of other modalities. In the delayed imaging (RI) study, the specificity was significantly improved from 62.9% to 91.4% (P = 0.0044, analyzed by the McNemar test). Overall, 18F-FDG PET delayed imaging (RI) was significantly more accurate than the other modalities (PET delayed imaging study vs. CT: P = 0.0004; PET delayed imaging study vs. 201Tl SPECT: P = 0.009; PET delayed imaging study vs. PET early imaging: P = 0.003, analyzed by the McNemar test). Furthermore, a close correlation between the RI-SUV results of the primary lesion and lymph node metastasis was observed (Fig. 6), which was helpful in the diagnosis of nodal staging.
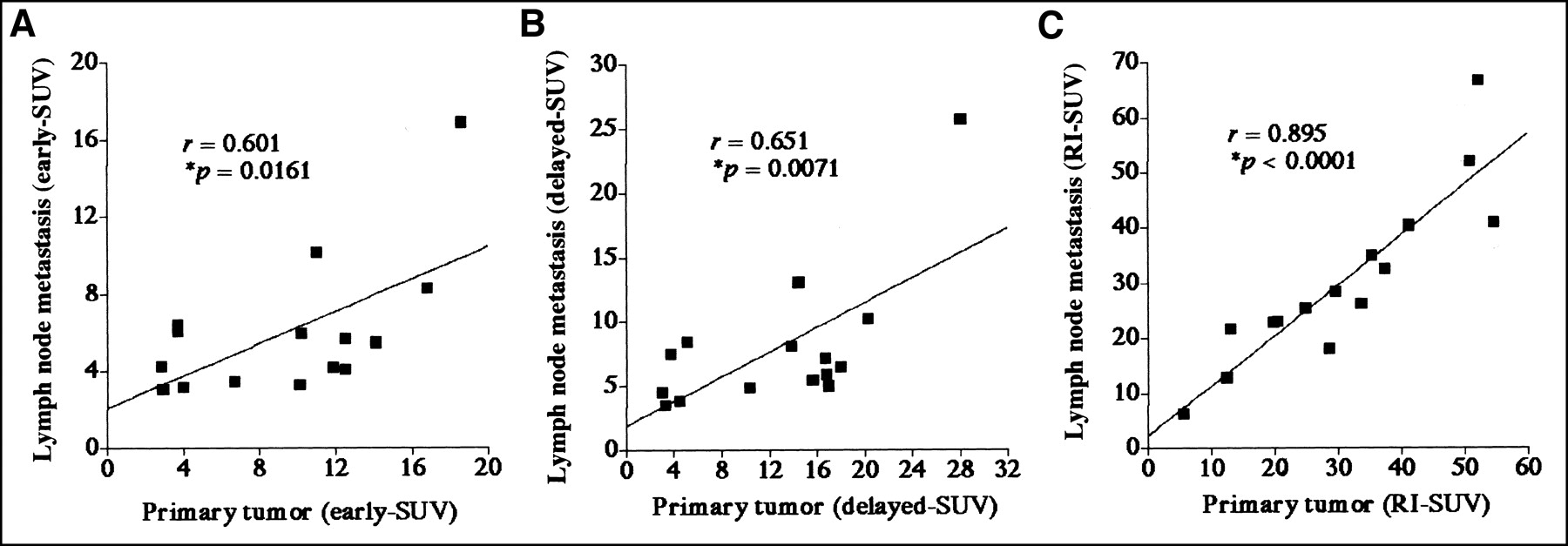
(A) Correlation between SUV levels of lymph node metastases and primary tumors in 18F-FDG PET early imaging of lung cancer patients with nodal involvement. Correlation between SUV levels of lymph node metastases and primary tumors was found (y = 0.418x + 2.113; r = 0.601; P = 0.0161). (B) Correlation between SUV levels of lymph node metastases and primary tumors in 18F-FDG PET delayed imaging of lung cancer patients with nodal involvement. Correlation between SUV levels of lymph node metastases and primary tumors was found (y = 0.482x + 1.894; r = 0.651; P = 0.0071). (C) Correlation between RI-SUV (%) of lymph node metastases and primary tumors in 18F-FDG PET early imaging of lung cancer patients with nodal involvement. Good correlation between RI-SUV (%) of lymph node metastases and primary tumors was found (y = 0.917x + 2.180; r = 0.895; P < 0.0001). Result in C showed best correlation among 3 graphs.
Comparison of 18F-FDG PET (Early Imaging, Delayed Imaging, and RI), 201Tl SPECT, and CT Results for Lymph Node Staging of Malignancy (Including 49 Cases of Lung Cancer)
DISCUSSION
In this study, we compared 18F-FDG PET and 201Tl SPECT, including early images, delayed images, and SUV RI, in evaluations of several kinds of thoracic lesions. As for differentiation between malignant and benign diseases, there were no significant advantages among 18F-FDG PET early and delayed imaging and 201Tl SPECT imaging; however, 18F-FDG PET RI (RI-SUV) was found to be useful and far superior to other scintigraphic techniques, thus improving diagnostic potential. Our results clearly suggest significant advantages of dual-time-point 18F-FDG PET imaging for differentiating malignant lesions from benign lesions, whereas delayed 18F-FDG PET imaging alone may not be helpful for differential diagnosis.
Several studies have shown the advantages of delayed imaging with 18F-FDG, and delayed scans have been reported as useful for the diagnosis of pancreatic cancer and breast cancer (14,15). Recently, Kubota et al. (16) found that 18F-FDG PET 2-h delayed imaging of the whole body easily detected malignant lesions because of the increased uptake by tumors along with a decreased normal background. Zhuang et al. (17) also showed differences in the rates of 18F-FDG uptake between malignant and inflammatory mononuclear cells and processes in vitro and suggested that lung lesions with decreased or stable SUVs over time are likely to have a benign etiology, whereas those with increased SUVs over time are likely to be caused by malignancy. Thus, we believe that the results presented in these reports support our clinical data. Actually, the usefulness of dual-time-point 18F-FDG PET imaging for the evaluation of pulmonary nodules was also reported by Matthies et al. (18). We consider that their outcomes were quite similar to ours. We selected a 1-h time point for early imaging and a 3-h time point for delayed imaging. Imaging 1 h later seems to be a conventional timing in 18F-FDG PET studies. As for 3-h later imaging, we expected the merit of 3-h later imaging compared with Kubota’s 2-h delayed imaging to be that the longer interval brought the larger difference of SUV of the thoracic lesion. The report of Hamberg et al. (19) supported our hypothesis. We also had to take into account the decay of radioactivity of 18F-FDG. Then, we decided on the imaging time points 1 and 3 h later.
The accuracy of nodal staging can also be improved by a combination of early and delayed 18F-FDG PET imaging. It is well recognized that the results of current nodal staging procedures in patients with lung cancer are not accurate; even 18F-FDG PET cannot provide sufficient data (12,20). Furthermore, previous reports have shown the advantages and limitations of 201Tl SPECT and 18F-FDG PET imaging in nodal staging (10, 12). The former is insufficient for sensitivity and the latter is inadequate for specificity of mediastinal staging, although they are better than CT. 18F-FDG accumulation with PET had a high sensitivity for malignancy; however, it also accumulated in many kinds of inflammatory lymph node swelling, reducing the specificity for diagnosis. Our results indicated similar findings as well. However, we found that 18F-FDG PET, including the analysis of RI, could distinguish between benign and malignant lymph nodes because malignant lymph nodal metastasis always increased SUV on delayed images and RI-SUV, whereas most normal tissue—including muscle, mediastinum, or benign lymph node swelling (such as inflammation and hyperplasia)—decreased SUV on delayed images and RI-SUV, with the exception of granulomatous inflammation such as sarcoid reaction. In addition, a close correlation between RI-SUV for primary tumors and lymph node metastasis is useful in the diagnosis of nodal involvement. Consequently, this method is considered to improve the specificity of mediastinal staging and provide a new and effective means for staging thoracic lymph nodes in patients with lung cancer, making it superior to other modalities for the assessment of hilar and mediastinal nodal metastases.
It is unclear why inflammatory and malignant lesions exhibit a differential 18F-FDG uptake pattern over time, although several cellular factors may contribute to this phenomenon. It is well known that many cancer cells express increased numbers of glucose transporters (21); thus, metabolic trapping through phosphorylation of FDG appears likely to be the rate-determining step for 18F-FDG retention in the cell. Hexokinase and glucose-6-phosphatase mediate the phosphorylation and dephosphorylation, respectively, of intracellular FDG. Unless 18F-FDG-6-phosphate is dephosphorylated by glucose-6-phosphatase, it is unable to leave the cell. Furthermore, it has been shown that most actively proliferating tumor cells have low levels of glucose-6-phosphatase (22, 23). On the basis of these observations, an increased ratio of hexokinase to glucose-6-phosphatase may result in a gradual accumulation of 18F-FDG-6-phosphate. In contrast, most normal tissues express greater levels of glucose-6-phosphatase than malignant cells, whereas mononuclear cells and fibroblast cells, which represent the major cell populations in chronic inflammation, also have a relatively a low ratio of hexokinase to glucose-6-phosphatase (24). However, different blood vessel density and flow can have a dramatic influence on 18F-FDG uptake (25). Thus, dual-time imaging and the retention of 18F-FDG can more accurately reflect the ratio of hexokinase to glucose-6-phosphatase, indicating cell proliferation potential (26,27).
Traditionally, a single time point SUV of 2.0–3.0 has been proposed as the optimal threshold for separating malignant from benign lung lesions (28,29). However, there is considerable overlap between SUV results of malignant and benign lesions, causing difficulty in correctly interpreting 18F-FDG PET data (30,31). As our results indicated, there is a wide range of 18F-FDG uptake (SUVs = 6.82 ± 4.36) among malignant lesions, whereas high SUVs in benign lesions have also been observed, such as for sarcoidosis or amyloidosis, which have SUVs as high as 10. Previous reports, along with our results, have shown that inflammatory and infectious lesions or benign variations can simulate malignant lesions in terms of SUV results (6–8). Consequently, SUVs at single time points alone may not be reliable enough to characterize malignant lesions with various pathologies. Therefore, an investigation of alternative methods using 18F-FDG PET for differentiation of malignancy from benign lesions is warranted.
It is known that 201Tl SPECT can differentiate between benign and malignant tumors (12,13). Because 201Tl accumulations are seen in malignant tumors on both early and delayed scans—however, not seen on delayed scans of benign tumors—the retention of 201Tl on delayed scans is strongly suggestive of malignancy (13). However, we found that 201Tl SPECT had a limitation in sensitivity for small lesions, and findings for both 18F-FDG PET and 201Tl SPECT showed that a positive RI gave false-positive results for the same 6 benign lesions (mycobacterosis). Few reports that have compared 18F-FDG PET and 201Tl SPECT, although Higashi et al. (32) recently found no significant differences between them regarding specificity for the differentiation of malignant and benign pulmonary nodules. From their results and our data, the conventional 18F-FDG PET imaging (early imaging) cannot provide sufficient accuracy to overcome the present situation; therefore, we recommend that RI-SUV results of 18F-FDG PET should be used for the diagnosis of unknown lesions because they are able to distinguish well-differentiated carcinoma from benign tumors (Fig. 3). However, another problem that must be resolved is how to distinguish active granulomatous diseases, such as tuberculosis, from malignancy (8) because they had SUV levels from 3 to 5 (4.97 ± 2.3) and an RI-SUV of 41.2%. These levels were higher than those of well-differentiated carcinoma and lower than those of poorly differentiated carcinoma. We believe that an understanding of these data as well as the results of thoracic CT scans will improve the potential accuracy for diagnosis of tuberculosis.
CONCLUSION
Our results provide further evidence that 18F-FDG PET is an important noninvasive method for the differentiation of malignant and nonmalignant lesions. This imaging technique, dual-time-point 18F-FDG PET imaging, has been found to be extremely helpful before surgery in patients with otherwise unclear thoracic nodules and nodal involvement.
Acknowledgments
We gratefully acknowledge the support by Prof. Yasuhisa Fujibayashi and the radiopharmaceutical chemistry group at Biomedical Imaging Research Center for their valuable assistance in preparing 18F-FDG.
Footnotes
Received Jul. 17, 2002; revision accepted Oct. 24, 2002.
For correspondence or reprints contact: Yoshiki Demura, MD, Third Department of Internal Medicine, Fukui Medical University, 23 Matsuoka-cho, Fukui Pref 910-11, Japan.
E-mail address: DEM2180{at}aol.com
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Efficacy and Limitations of F-18-fluoro-2-deoxy-D-glucose Positron Emission Tomography to Differentiate Between Malignant and Benign Bone and Soft Tissue Tumors
- Prognostic Value of Dual-Time-Point 18F-FDG PET for Idiopathic Pulmonary Fibrosis
- Interim FDG-PET in Hodgkin lymphoma: a compass for a safe navigation in clinical trials?
- Prognostic Implication of Dual-Phase PET in Adenocarcinoma of the Lung
- The Effectiveness of 18F-FDG PET/CT Combined with STIR MRI for Diagnosing Nodal Involvement in the Thorax
- Evaluation of Dual-Time-Point 18F-FDG PET for Staging in Patients with Lung Cancer
- Dual Time Point 18F-FDG PET Imaging Detects Breast Cancer with High Sensitivity and Correlates Well with Histologic Subtypes
- Dual-Time-Point 18F-FDG PET for the Evaluation of Gallbladder Carcinoma
- Potential of Dual-Time-Point Imaging to Improve Breast Cancer Diagnosis with 18F-FDG PET
- The Role of PET Scan in Diagnosis, Staging, and Management of Non-Small Cell Lung Cancer
- 18F-FDG PET of Gliomas at Delayed Intervals: Improved Distinction Between Tumor and Normal Gray Matter