


Abstract
In patients with gastroenteropancreatic (GEP) neuroendocrine tumors, we investigated the usefulness of somatostatin receptor scintigraphy (SRS) in the detection of liver metastasis, which represents the most important prognostic factor in these tumors, and in the management of affected patients. Methods: We enrolled 149 patients with GEP tumors, 69 during initial staging and 80 in follow-up. All patients underwent whole-body scanning at 4 and 24 h, followed by abdominal planar and SPECT imaging after intravenous injection of 250 MBq 111In-pentetreotide. The patients had previously been submitted to 2 of 3 conventional imaging procedures (CIP), such as CT, MRI, and ultrasound of the abdomen within 1 mo before SRS; on the basis of liver CIP data, the patients had been classified into 3 groups as follows: no evidence of liver metastases, the presence of resectable metastases, or the presence of nonresectable metastases. Results: Liver metastases were histologically proven in 65 cases. SPECT identified malignant lesions in 60 of 65 patients with metastases (sensitivity, 92.3%), planar imaging identified malignant lesions in 38 of 65 patients (sensitivity, 58.5%), and CIP identified malignant lesions in 52 of 65 patients (sensitivity, 80%). Only SPECT demonstrated liver involvement in 13 patients, whereas CIP showed liver involvement in 5 other cases. Moreover, SPECT was significantly more sensitive than planar imaging and CIP in identifying patients with single lesions. Neither SPECT nor planar imaging showed false-positive results in patients with no evidence of liver metastases, including 21 patients with hemangiomas (specificity, 100%), 12 of which were false-positive on CIP (specificity, 85.7%). SPECT per-lesion sensitivity (92.4%) was significantly higher than that of planar imaging (52.4%) and CIP (79.4%). Moreover, SPECT correctly changed patient classification and, thus, management in 28 of 149 patients (18.8%), whereas planar imaging changed classification in 13 patients (8.7%), identifying new or additional metastases not evident on CIP or excluding metastases on CIP of patients with false-positive findings, thus avoiding unnecessary surgery; however, SPECT classification was incorrect in 3.3% of patients, and planar imaging was incorrect in 17.4%. Conclusion: 111In-Pentetreotide SRS is a useful diagnostic tool in the detection of liver metastases in GEP tumor patients. In particular, SPECT proved to be significantly more sensitive and accurate than both planar imaging and CIP. Moreover, SPECT was also the most reliable procedure to obtain correct patient classification, thus guiding the most appropriate therapeutic strategy.
Gastroenteropancreatic (GEP) neuroendocrine tumors are rare neoplasms that may grow slowly, thus permitting long survival (1). Nevertheless, these tumors can be malignant and metastases do occur, which can be the first manifestation of the disease, seriously affecting patient prognosis (2–4). The most common metastases are in the liver and decrease the 5-y survival rate (5–7).
At present, tumor progression is becoming the main determinant in long-term survival of GEP tumor patients, given the very important, positive results obtained with the recent advances in medical therapeutic strategies directed at the control of hormone excess status; in the past, the latter represented the most important factor affecting survival (8,9).
Both the presence and the extent of liver metastases must be carefully evaluated to obtain a correct staging of GEP tumor patients and to guide the most appropriate therapeutic approach. In particular, if the metastases are limited to the liver, cytoreductive surgery can represent a potentially curative treatment when the metastases are still resectable (10); however, this surgical procedure is ineffective in nonresectable metastases for which other treatments are used, such as interferon-α and somatostatin analog therapy, chemotherapy, hepatic arterial embolization or chemoembolization, and even liver transplantation (5,11–13).
Conventional imaging procedures (CIP), such as CT, ultrasound, and MRI, represent the most available diagnostic methods to detect GEP tumors and their metastases, also guiding biopsies. In particular, MRI is considered the most sensitive radiologic method for liver metastases (5); however, liver metastases from GEP tumors, particularly if small in size, are sometimes difficult to localize by CIP (14).
Recently, somatostatin receptor scintigraphy (SRS) using the somatostatin analog 111In-pentetreotide as radiotracer has proven to be an important diagnostic tool for GEP tumors with an elevated density of somatostatin receptors (15–20) also demonstrating high sensitivity in identifying liver metastases (21,22). In the detection of the latter, in particular, SRS has been reported to be more sensitive than CIP by some authors (21), localizing lesions not detected by the latter procedures; however, these results have not been confirmed by others (23). With regard to SRS acquisition methods, controversial data have been described on the superiority of SPECT with respect to planar imaging (22,24), even though SPECT is generally considered to be more sensitive in the detection of focal lesions, particularly if small in size, given its better contrast resolution and its capacity to also give cross-sectional scintigraphic images (22).
The aim of this study was to further evaluate the usefulness of 111In-pentetreotide SRS as a diagnostic tool in GEP tumors, focusing on the detection of liver metastases. We also investigated whether SPECT SRS could give more useful information than either planar imaging or the other nonradioisotopic CIP, both in the diagnosis of liver metastases and in the therapeutic management of affected patients.
MATERIALS AND METHODS
Patients
One hundred forty-nine patients (73 males, 76 females; age, 11–81 y) were studied. In all patients, the definitive diagnosis of GEP tumors was obtained on the basis of specific biologic symptoms and secretion pattern, when present, and by histopathology and immunohistochemical analysis, as reported in Table 1.
Histologic Classification in 149 Patients with Ascertained GEP Tumors
Sixty-nine patients underwent SRS for an initial diagnosis and staging of primary tumors during the first admission, whereas 80 patients with previously ascertained GEP tumors were studied during follow-up. Before SRS, 56 of these 80 patients had been treated with both surgical procedures and medical therapies, and 3 patients with disseminated metastases, including in the liver, and serious clinical conditions had only undergone medical therapy; 41 of these 59 patients were still under octreotide treatment, which was withdrawn 3–14 d before scintigraphy in 36 cases, whereas 5 patients continued therapy because of their serious clinical conditions. The remaining 21 of these 80 patients had undergone only surgical procedures. All patients who underwent surgery for the primary tumor were submitted to liver exploration and intraoperative ultrasound during the operation; the negative data by these procedures were considered the gold standard for true-negative results in these cases.
Within a month before scintigraphy, all patients had been submitted to at least 2 of 3 CIP, including abdominal CT, ultrasound, and MRI; 5 or more liver lesions per patient observed by CIP were counted as 5. On the basis of CIP results in the liver, but also considering the presence of other ascertained distant metastases, the patients were initially classified into 3 groups: patients with apparently no evidence of liver metastases (NEM), patients with resectable metastases (RM), and patients with nonresectable metastases (NRM). The metastases were considered nonresectable on the basis of both the number of lesions (numerous and disseminated in both hepatic lobes) and their location (porta hepatis, confluence of hepatic veins entering into inferior vena cava); moreover, surgery was not considered feasible when too extensive in patients with serious clinical conditions and other distant metastases, even if metastases were considered resectable.
Before SRS, all patients were on a 3-d low-residue diet and the day before a laxative was administered, both continued for 48 h, according to the manufacturer’s recommendations. This protocol was followed to ensure bowel cleaning and thus avoid any interfering background radioactivity of the intestinal contents.
Radiopharmaceutical
After an incubation period of 30 min, the lyophilized preparation of 111In-pentetreotide (Mallinckrodt Medical, Petten, The Netherlands) in a single vial was diluted with 1–2 mL of 0.9 saline solution, and ∼250 MBq were then injected intravenously into each patient immediately after checking the specific purity by thin-layer chromatography. The labeling efficacy exceeded 95% in each preparation. The patients were encouraged to drink amply after the injection of the radiopharmaceutical to support the bowel cleaning process and renal elimination. No adverse reaction was observed in the whole series.
SRS
Images were obtained with a single-head circular large-field-of-view rotating gamma camera ([camera A] Starcam 2000; General Electric Medical Systems, Milwaukee, WI) or with a double-head gamma camera ([camera B] Helix; Elscint, Haifa, Israel), both of these equipped with medium-energy collimators. Two 20% energy windows were centered on the 111In photon peaks (173 and 247 keV).
First, a whole-body scan from anterior and posterior views with a speed of 10 cm/min was always performed at 4 and 24 h after radiotracer injection. For the study of the liver, immediately after whole-body scanning, 15-min planar views were obtained over the superior abdomen in anterior, posterior, and lateral projections, using a 128 × 128 word matrix. SPECT was then performed over the upper abdomen using different acquisition and processing parameters according to the 2 different gamma cameras. With gamma camera A, sixty 60-s images were acquired at a 6° angular step with a 64 × 64 matrix; the images were prefiltered using a Wiener filter and then reconstructed with a ramp filter. With gamma camera B, sixty 30-s images were acquired for each head at a 3° angular step with a 64 × 64 matrix using the body-contouring system to ensure the minimum distance between the patient and the collimator during rotation; the images were processed by the backprojection filter method with a count-optimized Metz filter without attenuation correction. A step-and-shoot mode was used with both gamma cameras and the images were obtained in transaxial, coronal, and sagittal slices. Delayed planar and SPECT images of the upper abdomen were also obtained at 48 h after injection in those cases in which a high abdominal background at 4 and 24 h was present. For these delayed examinations, the acquisition time was increased from 15 to 20 min for planar imaging and remained unchanged for SPECT when using gamma camera A, whereas sixty 45-s image acquisitions for each head at a 3° angular step were obtained when using gamma camera B.
Both planar and SPECT images were interpreted independently by 3 nuclear medicine physicians who were unaware of the results of any prior investigations; there was disagreement only over 2 SPECT examinations, which were resolved by consensus. Written informed patient consent was always obtained before scintigraphy.
The additional value of SPECT and planar liver SRS with respect to CIP in patient management was investigated as well as that of SPECT compared with planar imaging. Patient classification by CIP and its possible change according to SPECT and planar SRS results were determined initially by 2 different teams of nuclear medicine, surgery, and radiology specialists who rechecked together the results for the definitive classification.
Diagnosis of Liver Metastasis
The diagnosis of liver metastasis suspected on the basis of the imaging studies was defined histologically by percutaneous CT or ultrasound-guided liver biopsy or during laparotomy or surgery. Liver tissue excised during surgery was submitted to histopathologic analysis by hematoxylin and eosin staining to ascertain metastases; the specimens were also studied immunohistochemically to define their neuroendocrine origin.
Statistical Analysis
111In-Pentetreotide planar and SPECT SRS images and CIP images were classified as true-positive, true-negative, false-positive, or false-negative by considering histology or surgical exploration and intraoperative ultrasound of the liver as the gold standard. The sensitivity, specificity, and accuracy for the detection of liver metastasis were calculated on this basis. The sensitivity was calculated for the recognition of any liver metastasis in each patient.
The McNemar test was used to assess the statistical significance of the difference between the sensitivity, specificity, and accuracy of planar and SPECT SRS and CIP imaging in the detection of liver metastases both per patient and per lesion. The statistical significance of the differences in sensitivity of the 3 procedures was calculated taking into account all GEP tumor patients. The differences were also calculated in patients with metastases after subdividing the lesions according to their number (single or multiple). The χ2 test, or Fisher exact test when appropriate, was used to assess the statistical significance of differences in the sensitivity of each single procedure after subdividing the metastases according to their number (single or multiple). The results were considered significant when P < 0.05.
RESULTS
The presence of liver metastases was definitively ascertained by histologic examination in 65 of 149 GEP tumor patients (43.6%), as reported in Table 2, which illustrates the individual data of the 65 patients with metastases. In 23 cases the metastases were identified in the phase of initial staging and in 42 cases the metastases were identified during follow-up. In 21 patients the diagnosis was obtained by transcutaneous CT or ultrasound-guided biopsy and in the remaining 44 patients the diagnosis was obtained during laparotomy or surgery.
Individual Clinicopathology, Scintigraphy, and CIP Imaging Data in 65 GEP Patients with Liver Metastases
The results of both planar and SPECT 111In-pentetreotide SRS and of CIP in the detection of liver metastasis, also illustrated in Table 2, show that SPECT was true-positive in 60 of the 65 patients (92.3%) and planar imaging was true-positive in 38 of 65 patients (58.5%), whereas CIP identified metastases in 52 of 65 patients (80%). Only SPECT detected liver metastases in 13 of the patients (6 in the phase of initial staging and 7 during follow-up), whereas only CIP were positive in 5 different patients (1 in the phase of initial staging and 4 during follow-up). The latter 5 cases resulted the only false-negative cases on SPECT.
Planar imaging never identified patients with metastases undetected by SPECT or CIP and, thus, all 38 patients who were true-positive on planar imaging were also true-positive on both SPECT and CIP, whereas planar imaging was false-negative in 9 patients who were true-positive on both SPECT and CIP. Planar imaging was also always false-negative when SPECT (5 cases) or CIP (13 cases) was false-negative.
The 65 patients with metastases were also classified for management of liver metastasis on the basis of both planar and SPECT SRS and CIP data, as shown in Table 2: 13 of the patients were falsely considered NEM on CIP, 5 on SPECT, and 25 on planar imaging. The presence of other extrahepatic and distant sites of metastases in 19 patients is also reported in Table 2.
SPECT showed the highest per-patient sensitivity and accuracy values compared with both planar imaging and CIP, as illustrated in Table 3, which reports the overall sensitivity, specificity, accuracy, and positive and negative predictive values obtained by the 3 procedures in the 149 patients with GEP tumors (65 with and 84 without metastases). The differences were statistically significant only with respect to planar imaging for sensitivity and with respect to both CIP and planar imaging for accuracy (McNemar test). Neither SPECT nor planar imaging showed false-positive results in patients without metastases, including the 21 patients with proven hemangiomas, which were false-positive on CIP (CT or MRI) in 12 cases. Moreover, the metastases were also classified as single (22 patients) and multiple (43 patients); the sensitivity values of SPECT, planar imaging, and CIP are reported in Table 4, which also shows the statistical differences in the sensitivity, both mutually comparing the 3 procedures (McNemar test) and considering each procedure separately (χ2 test). SPECT was significantly more sensitive with respect to planar imaging and CIP in identifying the single lesions but not the multiple lesions; The CIP sensitivity was significantly higher than that of planar imaging for both single and multiple lesions. One patient with a single metastasis identified only on SPECT is reported in Figure 1 (patient 15). Moreover, SPECT did not show any significant difference in the sensitivity in detecting single as opposed to multiple lesions, whereas the sensitivity of both planar imaging and CIP was significantly higher in the detection of multiple with respect to single lesions.

Patient 15 with ileal carcinoid, who previously underwent surgery and who developed single liver metastasis ascertained on histologic examination. Lesion is visible on SPECT SRS (single arrow) on transaxial, sagittal, and coronal views (A), whereas planar SRS and CIP (B, both CT and MRI) were negative.
SPECT and Planar SRS and CIP Imaging: Overall Results in 149 Patients with GEP Tumors (65 With Metastases and 84 Without Metastases)
SPECT and Planar SRS and CIP Results in 65 Metastatic GEP Tumor Patients Classifying Metastases According to Number (Single or Multiple)
CIP or histologic information globally showed 185 liver metastases in 65 patients and 32 benign lesions, all hemangiomas, in an additional 21 patients. SPECT and planar SRS and CIP sensitivity, specificity, positive and negative predictive values, and accuracy were also evaluated according to the number of lesions, and the statistical differences between these parameters were also calculated (McNemar test), as illustrated in Table 5. SPECT had the highest per-lesion sensitivity, with statistical significance with respect to both planar imaging and CIP, revealing 74 metastatic lesions more than planar imaging in 43 of 65 patients and 24 lesions more than CIP in 32 of 65 patients, whereas only CIP visualized 14 lesions more than SPECT in 6 of 65 patients; a GEP tumor patient with multiple liver metastases, in whom SPECT showed more lesions than both CIP and planar imaging (patient 36), is shown in Figure 2. CIP detected 50 metastases more than planar imaging in 25 patients, whereas the latter identified only 4 lesions more than CIP in 2 patients. Furthermore, both SPECT and planar imaging were true-negative in all 32 hemangiomas ascertained in 21 patients, whereas CIP was false-positive in 18 of these hemangiomas found in 12 of the patients. The hemangiomas that were false-positive on CIP were all ≤2 cm in size, except 2, which were 3 cm.

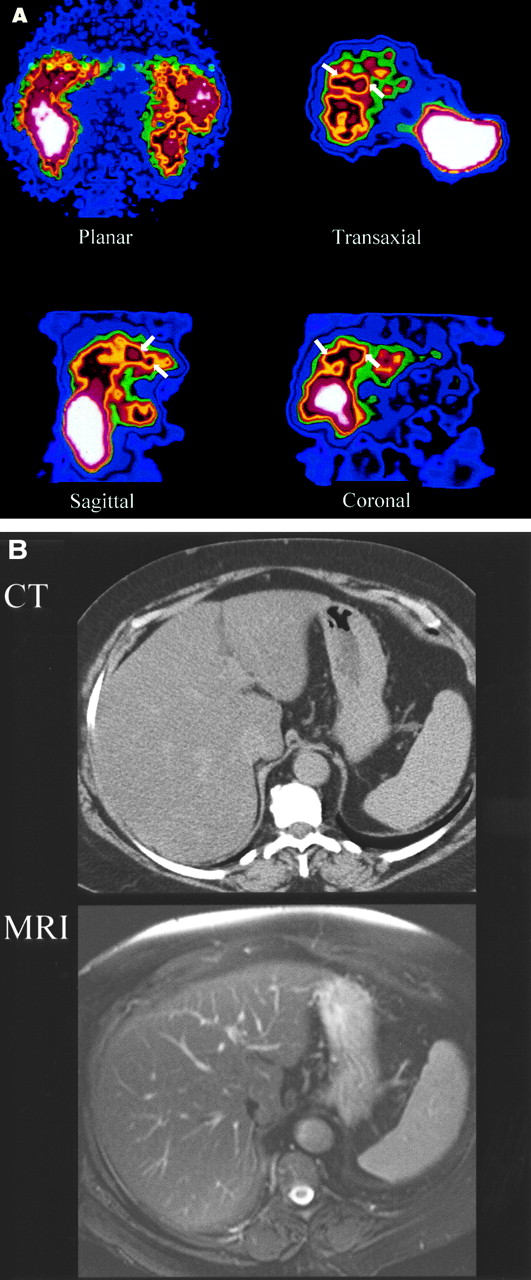
Patient 36 with pancreatic gastrinoma in whom abdominal SPECT SRS (A) reveals 2 liver metastases (single arrow), both visible on sagittal and coronal views. Only 1 liver metastasis is visible on transaxial view. Only 1 lesion is visualized by both planar imaging and MRI (B, double arrows). On CT view, negative for metastasis, primary tumor is visible.
SPECT and Planar SRS and CIP Overall Results in 217 Liver Lesions (185 Metastases and 32 Hemangiomas)
SPECT also revealed the exact number of metastases in 59 of 65 patients (90.8%), planar imaging in 15 of 65 patients (23%), and CIP in 38 of 65 patients (58.4%). The smallest liver metastasis visualized by SPECT was 7 mm in diameter. No difference in the number of liver metastases was observed when the images acquired at 4 h were compared with those acquired at 24 h; however, the latter resulted clearer, more detailed images with a better tumor/background ratio in all cases.
Regarding the role of SRS on patient management in the liver study, this procedure was able to modify or even completely change the therapeutic strategy in 28 of the 149 GEP tumor patients (18.8%) on SPECT and in 13 of these same patients (8.7%) on planar imaging.
Before SRS, on the basis of CIP data, the 65 patients with metastases had been classified as NEM in 13 patients, RM in 24 patients, and NMR in 28 patients, as reported in Table 2; in 19 of the NMR classifications, other distant metastases were also ascertained, contributing to the classification. Moreover, 12 patients with hemangiomas had been classified incorrectly on CIP as RM.
SPECT, but not planar imaging, localized previously undetected liver lesions in 13 patients who were falsely classified as NEM on CIP, thus modifying their classification: 11 of the 13 patients had a single metastasis and 2 of the 13 patients had 2 metastases each in the same lobe; all 13 patients were reclassified as RM and could be submitted to potentially curative surgery. One of these latter patients with 2 liver metastases ascertained only on SPECT is reported in Figure 3 (patient 56). SPECT detected additional liver metastases that became nonresectable in 3 additional patients who were initially classified as RM on CIP (detected by planar imaging in only 1 case); these patients were thus reclassified as NRM, changing the therapeutic approach. Both SPECT and planar SRS were false-negative in 5 patients with ascertained liver metastases; the primary tumor was a nonfunctioning islet cell carcinoma in 4 patients and a carcinoid in 1 patient. Moreover, 1 of these 5 patients had a single 6-cm liver lesion, 2 other patients had 2 lesions each (size range, 1–2.5 cm), and the remaining 2 patients had 3 lesions (size range, 1.2–2 cm) and >5 lesions (size range, 2–5 cm), respectively. In 3 of these patients the primary tumor had not been studied by SRS before the tumor excision, whereas in the remaining 2 patients the SRS had negative findings. None of these 5 patients had undergone antitumoral medical treatments before this study. According to planar imaging and SPECT SRS, these 5 patients were classified falsely as NEM, and only CIP correctly classified 1 of them as RM and 4 as NRM. SPECT confirmed the CIP classification in the remaining 44 of 65 patients with metastases. Planar imaging gave an incorrect patient classification in 26 of the patients with metastases, 5 of whom were correctly classified only on CIP, 15 only on SPECT, and 6 on both SPECT and CIP. In only 1 case, planar imaging and also SPECT gave the correct classification, which was incorrect on CIP. Furthermore, the 12 previously mentioned patients with ascertained liver hemangiomas, which were true-negative on SPECT and on planar imaging, who had been falsely classified as RM on CIP, had their classification changed to NEM, thus avoiding liver resection.

Patient 56 with rectal carcinoid in whom abdominal SPECT SRS (A) shows 2 liver metastases in 1 lobe (single arrow) on transaxial, sagittal, and coronal views, whereas planar SRS and CIP (B, both CT and MRI) are negative. Patient, who was classified as having NEM according to CIP data, was reclassified by SPECT SRS as having resectable metastases (RM) and underwent potentially curative surgery.
Thus, following the above classification in the 149 patients of our study (80 in follow-up and 69 in initial staging), 22 of the 42 patients in follow-up with liver metastases underwent partial liver resection, to which were also added 12 of the 23 patients in initial staging of the disease with ascertained liver metastases (the latter during surgery for the primary tumor performed on all 23 patients). In the above 34 patients who underwent liver resection, surgery was preceded by laparotomy in 17 patients and by percutaneous biopsy in 5 patients. These 34 patients included the 13 patients in whom only SPECT ascertained metastases and in 6 patients in whom the surgery was preceded by laparotomy. The remaining 38 of 80 patients in follow-up were considered true-negative because they had been classified previously as NEM according to liver exploration and intraoperative ultrasound during surgery for primary tumor and were persistently without clinical evidence of the disease and negative on both scintigraphy and CIP. The remaining 46 of 69 patients in initial staging, all negative on scintigraphy and 34 also negative on CIP, were considered true-negative for liver metastases because surgery for the primary tumor, performed on all of these patients, excluded metastatic liver lesions. Surgery was preceded by laparotomy or percutaneous lesion biopsy in 12 of these patients to ascertain hepatic hemangiomas, which were false-positive for metastasis on CIP.
DISCUSSION
The liver represents the most frequent site of metastases in GEP tumors, and survival decreases markedly in patients with liver involvement when compared with those with nonmetastatic liver disease (2,4). Moreover, the number of metastases appears to further affect survival, as reported by Weber et al. (9), who have revealed in a large series of GEP patients that those with an elevated number of metastases have a significantly worse 10-y survival rate (16%) with respect to patients with limited metastatic liver disease (79%).
Thus, the use of a very sensitive imaging procedure should be recommended to detect liver metastases from GEP tumors. In addition, this procedure should also have high resolution to determine with a close approximation the number of lesions and their distribution in the hepatic lobes for both a better prognostic stratification and a more correct therapeutic approach. An early diagnosis is crucial because cytoreductive surgery can be curative when metastases are still resectable (10) and also controls symptoms of hormone hypersecretion, whereas this surgical procedure is ineffective in diffuse metastatic liver involvement and, thus, other therapeutic strategies must be considered in these conditions (5,11–13,24).
In this study we used 111In-pentetreotide SRS as a diagnostic tool because it has demonstrated high values of sensitivity in the detection of both primary GEP tumors and their metastases, including those in the liver (21,22). Some authors (21,25) have reported the sensitivity of 111In-pentetreotide SRS, and in particular of SPECT, in liver metastases as higher than that of CIP (21,22), at present the most available methods, whereas sensitivity has been found to be similar for both procedures by others (24). Furthermore, in a small series of patients with gastrointestinal carcinoids, we observed previously that more liver metastatic sites were detected on SPECT compared with CIP and also planar imaging (22), whereas other authors (24) found that in 160 GEP tumors, 12 of 21 metastases missed by 111In-pentetreotide SPECT, but revealed by planar imaging, were found in the liver, thus excluding the idea that SPECT can substitute for planar imaging in detecting metastatic liver disease from GEP tumors.
The results of this study, performed in a large series of patients with liver metastases from different types of GEP tumors, indicate the higher sensitivity of 111In-pentetreotide SPECT with respect to planar imaging, thus confirming our previous data on carcinoid tumors. SPECT identified liver metastases in 92.2% of cases, with only 5 false-negative cases, also false-negative on planar imaging, but positive on CIP, with regard to patients with multiple lesions ranging from 1 to 5 cm, except 1 case with a single lesion of 6 cm. In these false-negative cases, lesion size would seem to have little importance and the interference from drugs can also be excluded because these patients had not been treated with antitumoral medical therapy before SRS. A low receptor density of metastases or the presence of other receptor subtypes not detectable by 111In-pentetreotide are more likely to be factors responsible for false-negative SPECT findings, as also hypothesized by other authors for different neuroendocrine tumors (26–29).
SPECT demonstrated a significantly higher sensitivity both per patient and per lesion than planar imaging, which globally missed 22 patients with metastases and 74 liver metastases more than SPECT; SPECT was also more sensitive than CIP, but the combined use of the 2 latter procedures achieved 100% per-patient sensitivity, thus suggesting their complementary use in detecting patients with liver metastases from GEP tumors; moreover, CIP was more sensitive than planar imaging, the latter revealing more lesions than CIP in only 2 patients, in 1 of whom it gave more additional diagnostic information for therapeutic strategy. SPECT was also significantly more sensitive than planar imaging and CIP in identifying the patients with a single liver metastasis, distinguishing between metastatic and nonmetastatic disease in >95% of patients with only 1 lesion, whereas no difference was ascertained when SPECT was compared with the other 2 procedures in patients with multiple lesions. Thus, SPECT seems to play a very important role in the early diagnosis of liver metastases when still in a curative phase. Our study also seems to demonstrate that SPECT can give more useful prognostic information because it determined the exact number of lesions in 90.8% of patients, whereas planar imaging and CIP did so in 23% and 58.4%, respectively.
Furthermore, both SPECT and planar 111In-pentetreotide SRS were always true-negative in patients without liver metastases, including those with hemangiomas. Such lesions, which are relatively frequent in patients with GEP tumors, resulted in false-positive findings on CIP in 12 of 21 patients with hemangiomas, thus reducing the CIP specificity; all CIP false-positive hemangiomas except 2 were ≤2 cm in size. These results seem to indicate that both planar and SPECT SRS could be more reliable tools than CIP in differentiating liver metastases from small-size hemangiomas, as also reported by other authors (14,30).
On the other hand, SPECT, besides presenting a higher sensitivity, also demonstrated a significantly higher accuracy with respect to both CIP and planar imaging, whereas no difference was ascertained between the 2 latter methods; thus, the lower number of false-negative results and the higher accuracy of SPECT when compared with planar imaging suggest that SPECT is to be preferred to planar imaging in the diagnostic protocol of liver metastases from GEP tumors even though the 2 procedures showed the same specificity values.
In addition, SPECT achieved the important goal of correctly modifying or completely changing the therapeutic strategy in 18.8% of patients, whereas planar imaging only changed the therapeutic strategy in 8.7% of patients, all correctly classified by SPECT. Moreover, SPECT was the only imaging procedure to detect, in some cases, previously unsuspected single liver lesions and multiple lesions in 1 lobe, so that the patients could be reclassified correctly as RM instead of NEM; SPECT also identified additional lesions in 3 further cases (planar imaging in 1 case) involving >1 lobe and thus classified as NRM patients who were previously considered as RM according to the CIP results. Moreover, SPECT, and also planar imaging, was true-negative in patients who were falsely classified as having metastases on CIP, thus avoiding unnecessary surgical procedures. The above percentage of our patients appropriately classified by both planar and SPECT 111In-pentetreotide SRS with respect to CIP represents the direct measure of gain of the former procedures. On the other hand, patient classification was incorrect on SPECT in 3.3% of cases, SPECT having missed the liver metastases ascertained only by CIP, whereas planar imaging underestimated or missed metastatic disease in 17.4% of patients.
Thus, in this study, 111In-pentetreotide SPECT proved to be the most effective procedure for a correct classification of patients with liver metastasis, crucial for the most suitable treatment and, thus, the most reliable tool for guiding therapy and avoiding unnecessary invasive therapeutic procedures. However, only the combined use of SPECT and CIP achieved correct classification in all patients, thus suggesting that these procedures should be used together for this purpose.
Finally, according to our results, both SPECT and planar images acquired at 24 h always showed a better tumor/background ratio in respect of those acquired at 4 h, permitting a sharper visualization of metastases, and the same number of lesions, thus suggesting that the 4-h acquisition might not be necessary in the detection of liver metastases from GEP.
CONCLUSION
Our data indicate that 111In-pentetreotide SRS is a useful diagnostic tool in the detection of liver metastases in GEP tumor patients. In particular, SPECT proved significantly more sensitive and accurate than planar imaging with the same high specificity, thus suggesting that it should be preferred. Furthermore, SPECT, more than planar imaging, seems able to give additional information in the cases in which CIP underestimates the extension of liver metastases or even misses the metastatic disease; SPECT, as well as planar imaging, can exclude metastases in patients with small-sized hemangiomas.
Thus, SPECT 111In-pentetreotide SRS can be considered one of the choice methods in the diagnostic protocol of liver metastases from GEP tumors; moreover, it appears to be very reliable for the correct classification of affected patients and the most appropriate therapeutic strategy.
Footnotes
Received Jun. 10, 2002; revision accepted Oct. 9, 2002.
For correspondence or reprints contact: Giuseppe Madeddu, MD, Department of Nuclear Medicine, University of Sassari, Viale San Pietro 8, 07100 Sassari, Italy.
E-mail: prof.madeddu{at}tin.it
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Evaluation of a Correction Method for 111In-Pentetreotide SPECT Imaging of Gastroenteropancreatic Neuroendocrine Tumors
- Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours (NETs)
- Gluc-Lys([18F]FP)-TOCA PET in Patients with SSTR-Positive Tumors: Biodistribution and Diagnostic Evaluation Compared with [111In]DTPA-Octreotide
- Factors Predicting Tracer Uptake in Somatostatin Receptor and MIBG Scintigraphy of Metastatic Gastroenteropancreatic Neuroendocrine Tumors
- Guidelines for the management of gastroenteropancreatic neuroendocrine (including carcinoid) tumours
- Detection of Liver Metastases From Endocrine Tumors: A Prospective Comparison of Somatostatin Receptor Scintigraphy, Computed Tomography, and Magnetic Resonance Imaging