


Abstract
To preserve the oral organs and functions in patients with head and neck carcinoma, accurate determination of the appropriate treatment after neoadjuvant chemotherapy and radiotherapy is of critical importance. We evaluated the diagnostic accuracy of 18F-FDG PET relative to that of other conventional imaging modalities in the assessment of therapeutic response after combined intraarterial chemotherapy and radiotherapy as an organ preservation protocol. Methods: The study was prospectively performed on 23 consecutive patients with head and neck squamous cell carcinoma who completed the treatment regimen and underwent 2 18F-FDG PET studies before and after neoadjuvant chemoradiotherapy. 67Ga scintigraphy (only before therapy) as well as MRI and CT (both before and after therapy) were also performed. All images were blindly and independently interpreted without knowledge of histologic findings. The level of confidence in image interpretation was graded by means of a 5-point rating system (0 = definitely no tumor to 4 = definite tumor). Results: Before treatment, 18F-FDG PET detected primary tumors in all 23 patients and was more sensitive (100%) than MRI (18/23; 78.3%), CT (15/22; 68.2%), and 67Ga scintigraphy (8/20; 40%), with a confidence level of 3 or 4 as a positive tumor finding. After chemoradiotherapy, residual tumors were histologically confirmed in 4 patients (pathologic complete response rate, 19/23; 82.6%). Although posttreatment 18F-FDG PET showed almost equal sensitivity (4/4; 100%) compared with MRI (3/3; 100%) or CT (3/4; 75%), its specificity (17/19; 89.5%) was superior to MRI (7/17, 41.2%) and to CT (10/17; 58.8%) for primary lesions. Regarding metastases to neck lymph nodes, only specificity for posttreatment images was calculated because no metastasis was confirmed in any patients after treatment. Six subjects had 18F-FDG PET-positive lymph nodes, which had pathologically no tumor cells and suggested an inflammatory reactive change after therapy. Therefore, the specificity of posttreatment 18F-FDG PET (17/23; 73.9%) was almost identical to that of MRI (17/20; 85%) and CT (16/21; 76.2%) for neck metastasis. With combined chemoradiotherapy monitored with 18F-FDG PET, 8 patients avoided surgery and the remaining 15 patients underwent a reduced form of surgery. Conclusion: 18F-FDG PET facilitates differentiation of residual tumors from treatment-related changes after chemoradiotherapy, which may be occasionally difficult to characterize by anatomic images. 18F-FDG PET has a clinical impact for the management of patients with head and neck cancers after neoadjuvant chemoradiotherapy by optimizing surgical treatment for each patient and contributes to the improvement of the patient’s quality of life.
In the treatment of resectable head and neck cancer, preservation of organs and functions such as speech, swallowing, and mastication as well as cosmetic appearance is of critical importance. To reduce functional damage caused by surgery, neoadjuvant chemotherapy and radiotherapy have become a primary treatment for head and neck cancer (1–5). Hence, precise determination of the most effective anticancer therapies before surgery is of great importance in clinical decision making regarding individual patients. Previously, the effect of anticancer treatment has been evaluated mainly on the basis of the morphologic changes that are imaged using CT and MRI. Because the size of the tumor after therapy is not directly related to the viability of the tumor, these imaging techniques have limitations in assessing therapeutic effects. In addition, neoadjuvant chemoradiotherapy can produce severe mucositis, edema, scarring, and granulation tissue, which might interfere with the detection of persistent disease using conventional diagnostic methods.
PET using 18F-FDG has been confirmed to be a noninvasive, reliable diagnostic imaging tool for various kinds of malignancies, including head and neck cancers, allowing for a functional assessment of the tumor (6,7). FDG is a glucose analog, and accumulation of FDG in the cells is proportional to glucose consumption. Increased uptake of FDG, associated with increased glycolytic activity in cancer cells, can be imaged and quantified by means of PET (8,9). 18F-FDG PET has an advantage over other imaging modalities to detect the change of glucose metabolism that is closely related to the viability of cancer cells.
We have previously shown the clinical value of 18F-FDG PET for monitoring response to combined intraarterial chemotherapy with radiotherapy (4). The purpose of this study was to compare the diagnostic accuracy of 18F-FDG PET with that of other conventional imaging modalities (CT, MRI, and 67Ga scintigraphy) before and after combined intraarterial chemotherapy and radiotherapy as an organ preservation protocol for the management of head and neck cancer.
MATERIALS AND METHODS
Patients
The study was prospectively performed on 23 consecutive patients with head and neck cancer (18 men, 5 women; mean age, 63.8 y; age range, 47–85 y), who completed the treatment regimen described below and underwent 2 18F-FDG PET studies before and after treatment (Table 1). The clinical staging was based on the International Union Against Cancer TNM classification (10) and the American Joint Committee on Cancer TNM classification (11). The 18F-FDG PET study was performed on all patients before biopsy to eliminate the influence of biopsy on PET results. Thirteen of 23 patients were in stage III or stage IV. Seventeen patients had a well-differentiated squamous cell carcinoma (SCC) and the remaining 6 patients had a moderately differentiated SCC. The study protocol was approved by the Ethical Committee of Fukui Medical University, and all patients gave written informed consent.
Patient Characteristics and Imaging Results Evaluated for Primary Tumors Before Treatment
All 23 patients received our neoadjuvant chemoradiotherapy as an organ preservation protocol, which consisted of 2 courses of intraarterial chemotherapy, including tetrahydropyranyl adriamicin, 5-fluorouracil, and carboplatin, combined with radiotherapy (30–40 Gy) (4). In 7 subjects with advanced tumors crossing the midline, the catheter was placed bilaterally.
All patients underwent serial 18F-FDG PET just before and >4 wk (mean, 38 d) after the combined chemoradiotherapy. As for the conventional imaging modalities, MRI (before, n = 23; after, n = 20) and CT (before, n = 22; after, n = 21) were performed before and after treatment. In addition, 67Ga scintigraphy was done in 20 patients before treatment. All examinations, including biopsies, were performed within 2 wk of each PET study.
After the second PET study following neoadjuvant chemoradiotherapy, therapeutic effects were evaluated histologically using surgical or biopsy specimens and classified as pathologic complete response ([PCR] no viable tumor cells) or as residual disease (residual tumor cells) for the primary site.
18F-FDG PET
All PET imaging procedures in this study were exactly the same as in our previous study (4). FDG was produced using an automated FDG synthesis system (NKK, Tokyo, Japan) using a small cyclotron (OSCAR3; Oxford Instruments, Oxon, U.K.) (12). PET scanning was performed using an Advance system (General Electric Medical Systems, Milwaukee, WI) (13). Transmission scans were obtained for 10 min using a standard rod source of 68Ge/68Ga for attenuation correction of the emission images.
The subjects, in a fasting state, were administered 244–488 MBq (6.6–13.2 mCi) 18F-FDG from the cubital vein over 10 s. In 5 patients, static images were obtained for 20 min, starting at 40 min after injection. Eighteen patients underwent dynamic PET scanning for 60 min. For these patients, we added dynamic frames from 40 to 60 min after injection to generate static images that were used for the analysis of this study. Plasma glucose levels were measured in all patients.
Conventional Imaging
CT scans were obtained using a standard CT scanner (HiSpeed Advantage RP; GE Yokogawa Medical Systems, Tokyo, Japan). We obtained contiguous transaxial images from the thoracic inlet to the base of the skull at 4- to 5-mm intervals with a slice thickness of 4–5 mm. All patients underwent both plain and contrast-enhanced scanning using 100 mL contrast material (iopamidol, 300 mg/mL; Daiichi Seiyaku, Tokyo, Japan) injected intravenously.
MR images were obtained using a 1.5-T superconducting MRI scanner (Signa 1.5T; GE Yokogawa Medical Systems). All MR studies included fast spin echo T1- and T2-weighted images. Contrast-enhanced images were obtained after an intravenous injection of Gd-diethylenetriamine pentaacetic acid (0.1 mmol/kg). In addition, postcontrast fat-suppression T1-weighted images were obtained using a presaturation pulse technique using chemical-shift selective sequence (14). The same fat-suppression technique was used for the fast spin echo T2-weighted images. Transaxial, coronal, and sagittal images were obtained.
Whole-body planar 67Ga images were obtained using a dual-head gamma camera (RC-2500IV; Hitachi, Tokyo, Japan) 48 h after an injection of 111 MBq 67Ga citrate.
Image Analysis
Three experienced examiners visually and semiquantitatively interpreted pre- and posttreatment 18F-FDG PET, CT, and MRI as well as pretreatment 67Ga scintigraphy independently. At the time of image interpretation, relevant correlative information concerning the histopathologic findings was not available. To compare the diagnostic accuracy of 18F-FDG PET with that of the other conventional imaging modalities, these images were carefully evaluated for the detection and delineation of the primary lesions and metastases to regional lymph nodes. A level of confidence in image interpretation was graded by using a 5-point grading system (0 = definitely no tumor, 1 = probably no tumor, 2 = equivocal, 3 = probable tumor, 4 = definite tumor). For each image, we adopted the median of the grading scale values assigned by the 3 readers. In this study, we defined the confidence level of 3 and 4 as a positive tumor finding.
Finally, the results of pre- and posttreatment images for primary lesions were correlated with those of the histologic evaluation, which served as the gold standard. For regional lymph nodes, only posttreatment images were evaluated because there was no histologic confirmation of metastasis before treatment. Final diagnosis for the presence or absence of metastases to lymph nodes after chemoradiotherapy was obtained by the histopathologic findings from surgical specimens or through the follow-up of the clinical course for >1 y.
For quantitative evaluation, regions of interest (round in shape and 5 mm in diameter) were placed over the area of highest 18F-FDG uptake in the tumor on the static images. The 18F-FDG uptake value was corrected for the injected dose and patient body weight to obtain the standardized uptake value (SUV).
Statistical analysis was performed using the Wilcoxon signed rank test and paired Student t test (2-tailed). P < 0.05 was considered to be statistically significant. The confidence interval for a proportion was calculated according to the Wilson procedure with a correction for continuity (15).
RESULTS
Pretreatment Images
All pretreatment 18F-FDG PET images demonstrated a focus of high 18F-FDG uptake corresponding to the known primary tumor. On the basis of the 5-point grading system, 18F-FDG PET was assigned to grade 4 in 22 of 23 tumors (Table 1). The average grade for 18F-FDG PET (3.96) was significantly higher than that for MRI (3.0), CT (2.77), and 67Ga scintigraphy (1.4). Moreover, 18F-FDG PET detected small superficial tumors on the tongue, lower lip, or mandibular gingiva in 5 patients that were not detected by MRI, CT, or 67Ga scintigraphy (Fig. 1).

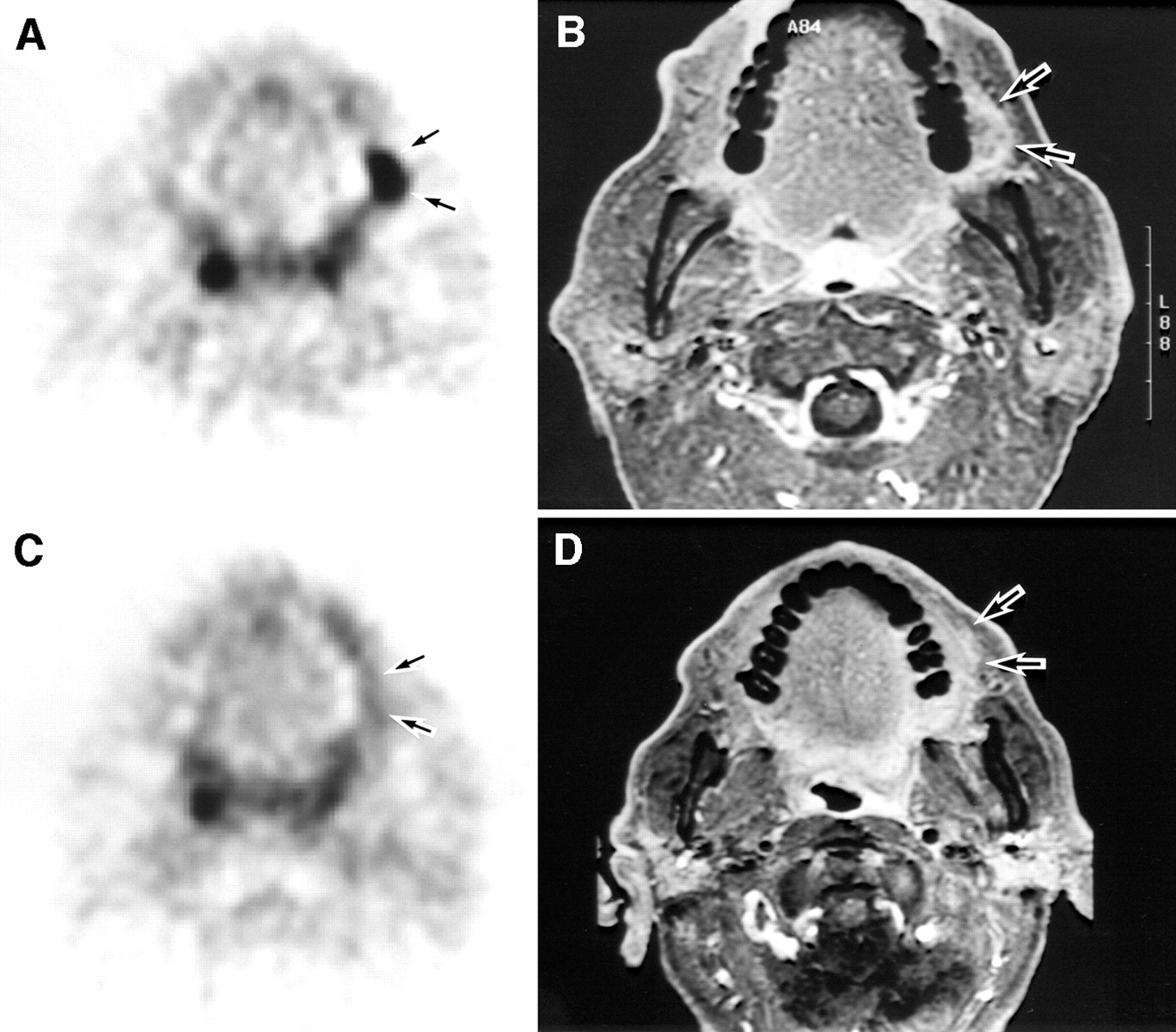
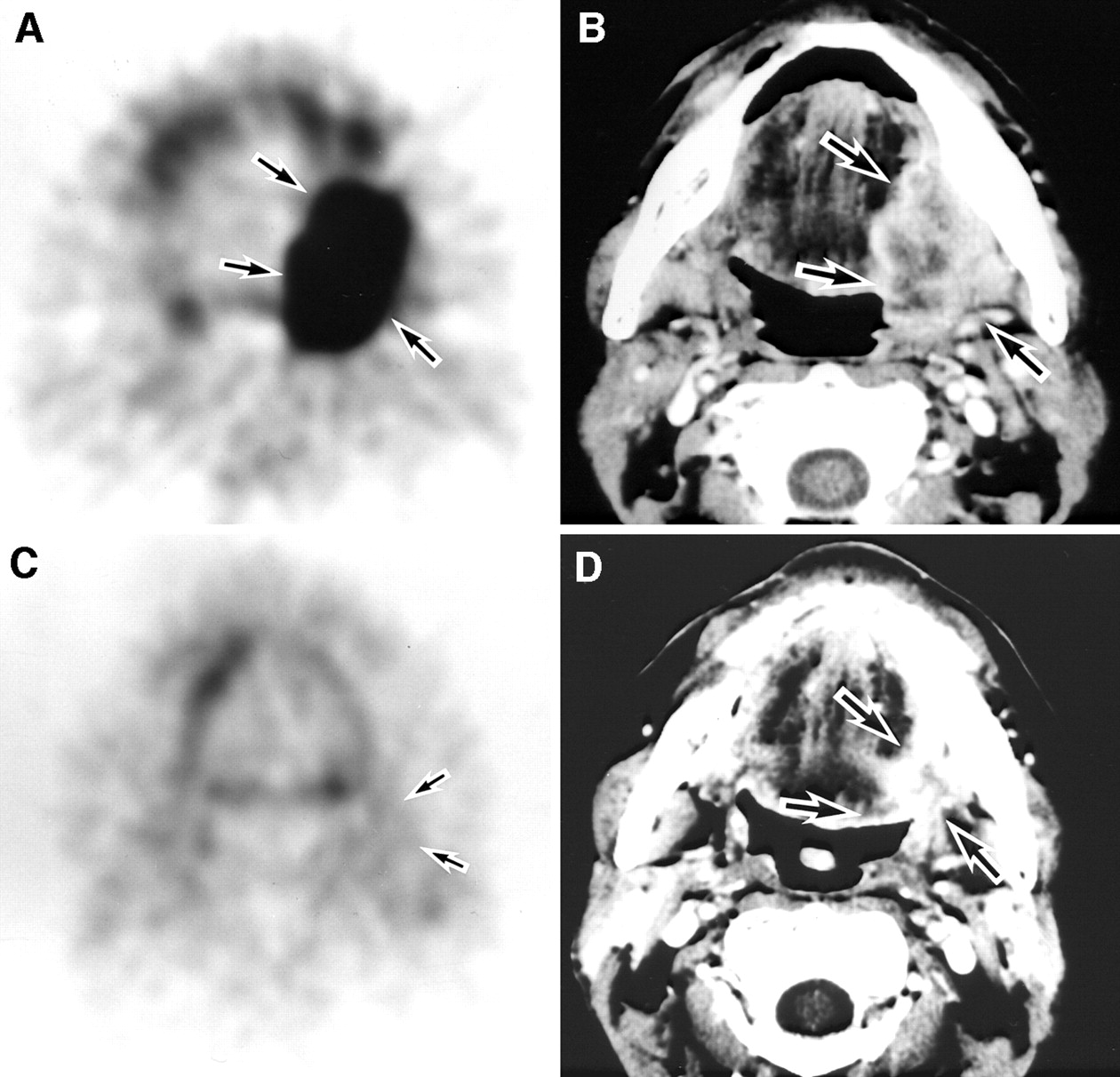
Pretreatment and posttreatment 18F-FDG PET (A and C) and corresponding MR (B and D) images of 63-y-old man with squamous cell carcinoma on left buccal mucosa. (A) 18F-FDG PET image shows intense focal accumulation of 18F-FDG (SUV = 5.59 mg/mL) in tumor before therapy (arrows). (B) Tumor is also visualized on postcontrast fat-suppression T1-weighted MR image (B) but not on CT image. (C) After chemoradiotherapy, 18F-FDG PET image reveals normalization of 18F-FDG uptake (arrows; SUV = 2.80 mg/mL), consistent with histologic finding of no viable tumor cells (PCR). (D) MR image still shows contrast enhancement in tumor although it is reduced in size (arrows), which may suggest residual tumor (false-positive). On basis of PET findings, patient avoided surgery. He has remained tumor free for >4 y.
When we consider the confidence level of 3 and 4 as a positive tumor finding, 18F-FDG PET is more sensitive (sensitivity, 23/23; 100%) than MRI (18/23; 78.3%), CT (15/22; 68.2%), or 67Ga scintigraphy (8/20; 40%) in detecting pretreatment primary head and neck cancer (Table 2).
Sensitivity of Pretreatment Images for Primary Tumors
Posttreatment Images and Histologic Findings for Primary Lesions
After chemoradiotherapy, all primary lesions showed an obvious decrease in size not only on visual inspection but also on CT and MRI. The histologic evaluation revealed PCR in 19 of 23 patients (PCR rate, 82.6%) without viable tumor cell in any section, which was confirmed by the fact that no patient developed a local recurrence in >3 y. The remaining 4 patients had residual tumor cells (Table 3).
Histologic Findings and Imaging Results Evaluated for Primary Tumors and Lymph Nodes After Treatment
Regarding the posttreatment images of the primary lesions in the 4 patients with residual tumor, the average grades for 18F-FDG PET, MRI, and CT were 3.25, 3.0, and 3.0, respectively. Therefore, 18F-FDG PET had an equal sensitivity (4/4; 100%) compared with that of MRI (3/3; 100%) or CT (3/4; 75%). However, the specificity of posttreatment 18F-FDG PET (17/19; 89.5%) was superior to that of MRI (7/17; 41.2%) and CT (10/17; 58.8%) (Table 4; Figs. 1 and 2).
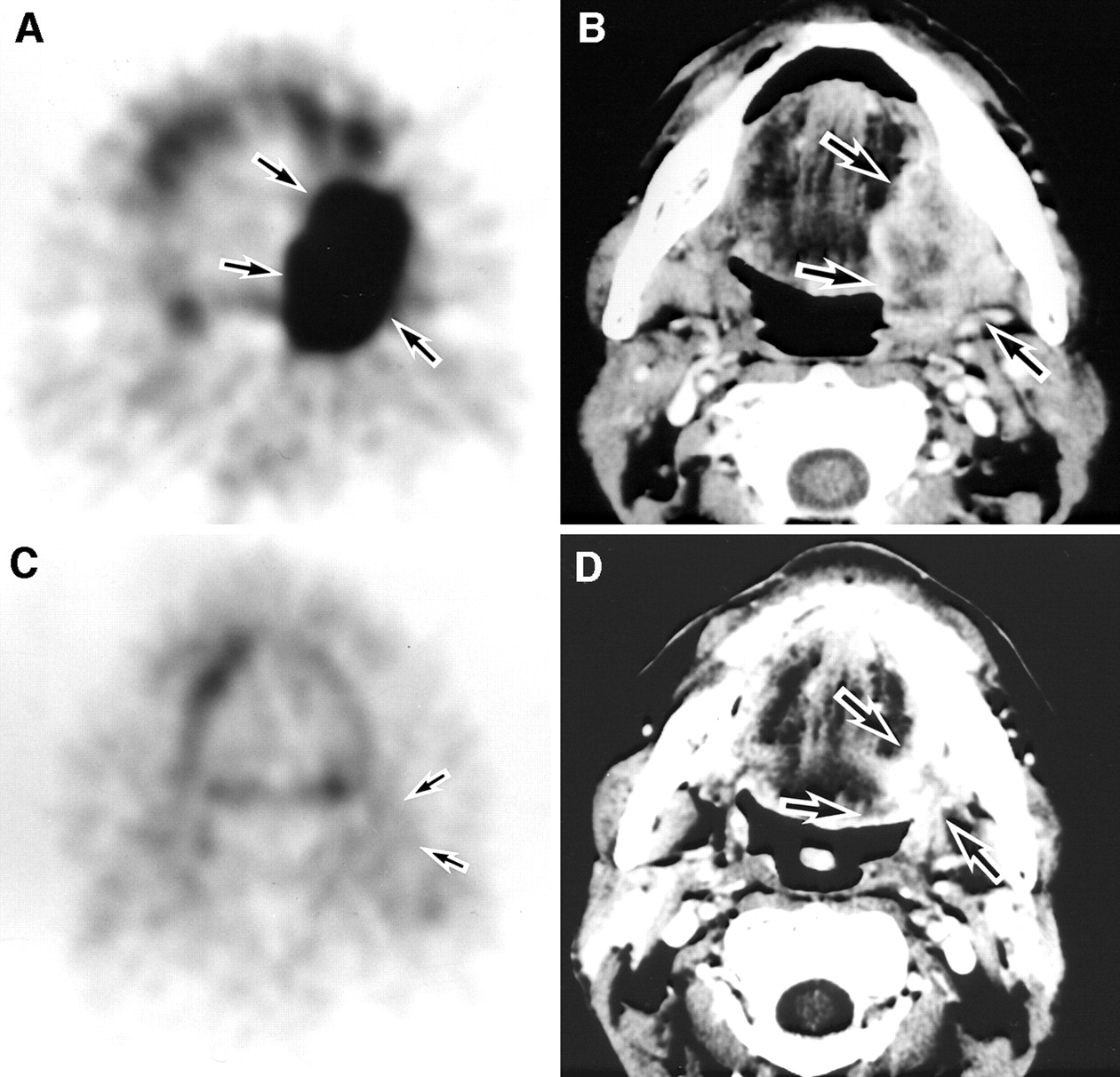
Pretreatment (A and B) and posttreatment (C and D) images of 60-y-old man with large squamous cell carcinoma (T4 N2a M0) on left mandibular gingiva. Pretreatment 18F-FDG PET image (A) shows focus of high 18F-FDG accumulation (SUV = 12.77 mg/mL) on left mandible (arrows), consistent with postcontrast CT (arrows, B) findings. After chemoradiotherapy, tumor disappeared on visual inspection with slight induration. (C) Posttreatment 18F-FDG PET image shows no abnormal 18F-FDG accumulation (arrows; SUV = 3.11 mg/mL), consistent with histologic finding (PCR). (D) CT image shows remarkable reduction in tumor size but does not exclude residual tumor because of contrast enhancement (arrows). According to 18F-FDG PET findings, patient successfully underwent functional neck dissection and marginal resection of mandible, requiring neither continuous resection of mandible nor reconstructive surgery.
Sensitivity and Specificity of Posttreatment Images for Primary Tumors and Lymph Nodes
Posttreatment Images for Neck Lymph Nodes
Posttreatment images showed positive finding in 6 of 23 patients for 18F-FDG PET, 3 of 20 for MRI, and 5 of 21 for CT, although no metastasis to neck lymph nodes was confirmed pathologically. Therefore, the specificity of posttreatment 18F-FDG PET (17/23; 73.9%) was almost identical to that of MRI (17/20; 85%) or CT (16/21; 76.2%) for the neck region (Table 4). Although 8 patients showed positive findings for metastases to lymph nodes before treatment, 7 of them showed no focal 18F-FDG uptake after treatment. Five of 6 patients with a focal 18F-FDG uptake in the neck region after treatment did not have any focal abnormality before treatment. Although these findings were assigned as false-positive, a focal 18F-FDG uptake seemed to be caused by an inflammatory reactive change after treatment (Fig. 3). There was no recurrence in neck lymph nodes for the follow-up period of >3 y. In 2 of 6 patients, no metastasis was pathologically confirmed in specimens obtained by neck dissection.
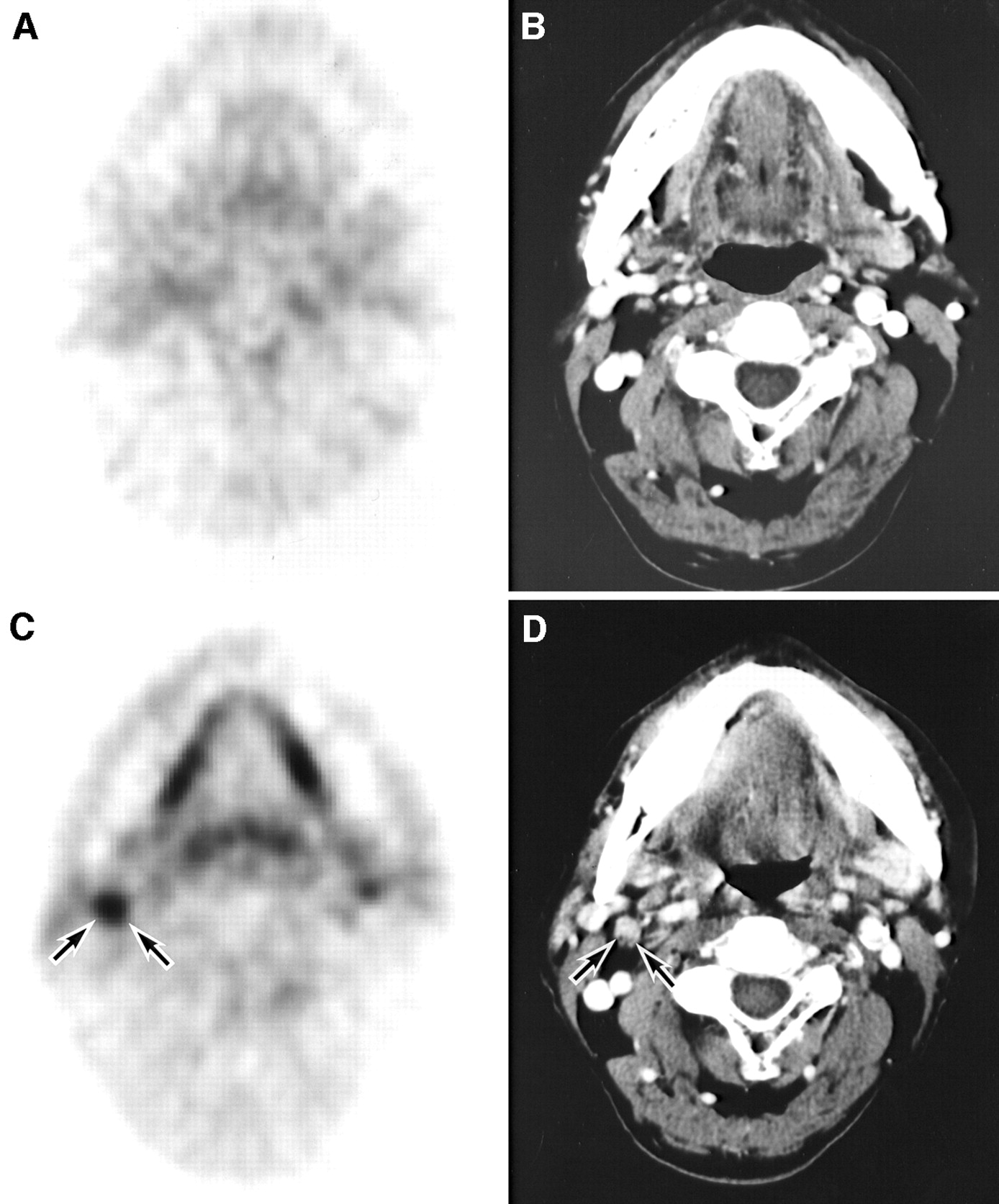
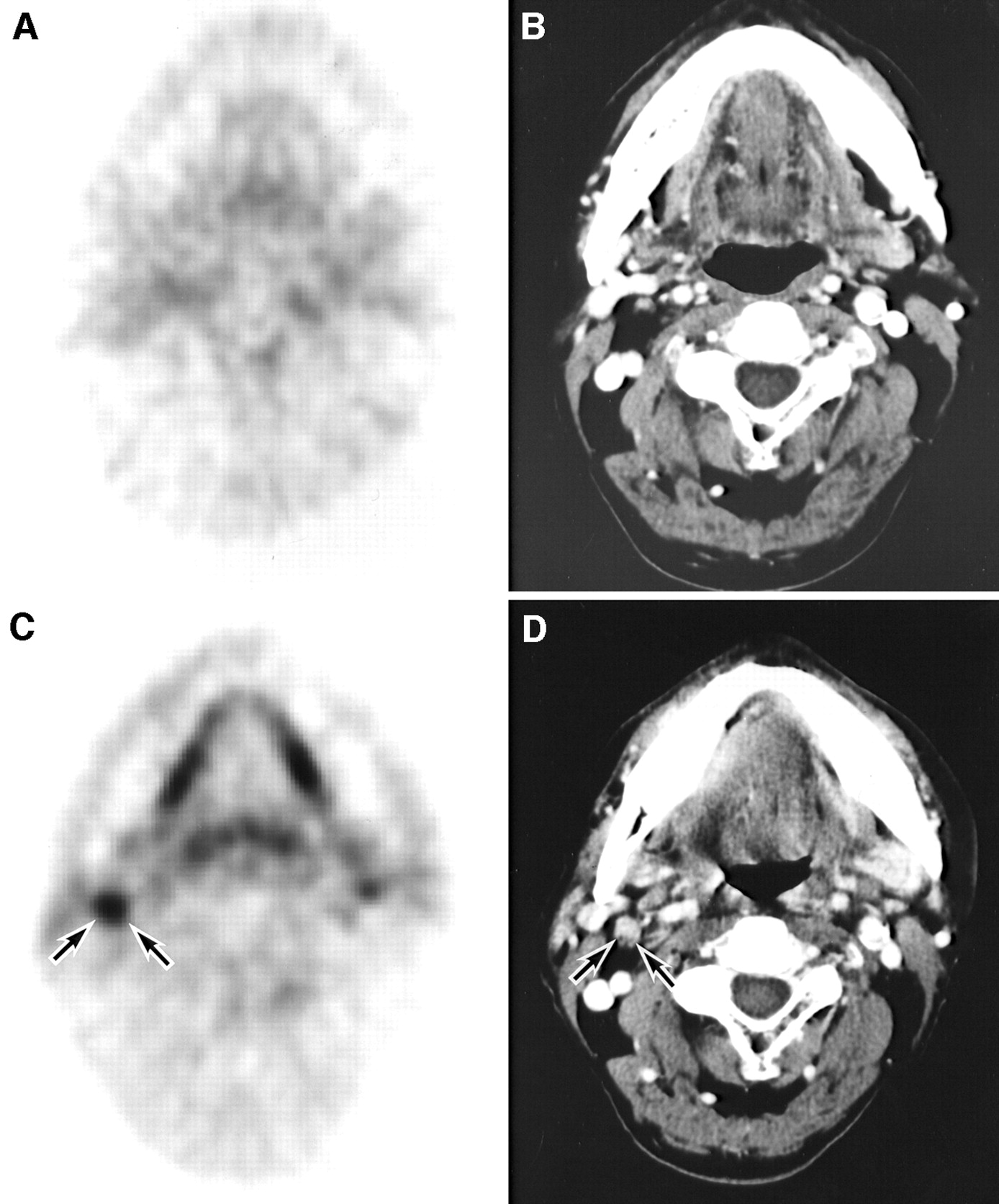
Pretreatment (A and B) and posttreatment (C and D) neck images of 78-y-old man with squamous cell carcinoma (T2 N0 M0) on floor of mouth. Pretreatment PET (A) and corresponding postcontrast CT (B) images demonstrate no metastasis to neck lymph nodes. (C) After chemoradiotherapy, neck lymph nodes were not palpable and posttreatment PET image shows abnormal 18F-FDG uptake in neck region (arrows, false-positive) probably due to inflammatory and reactive change. (D) Posttreatment CT image shows small lymph node (<1 cm; arrows, true-negative) in neck region, suggesting no metastasis. Patient was confirmed to have no metastasis in neck by clinical follow-up for >3 y.
18F-FDG Findings and Further Treatment
The mean SUV for the primary tumors significantly decreased from 9.15 ± 4.79 mg/mL (range, 4.07–26.10 mg/mL) to 3.60 ± 1.55 mg/mL (range, 1.12–8.32 mg/mL) (P < 0.01). Lesions with residual tumor cells had a posttreatment SUV of 5.54 ± 1.63 mg/mL, whereas those without tumor cells had an SUV of 3.19 ± 1.15 mg/mL. There were no viable tumor cells in the lesion with a posttreatment SUV of <4 mg/mL. With this cutoff level of 18F-FDG PET after combined chemoradiotherapy, 8 patients avoided surgery and the remaining 15 patients underwent a reduced form of surgery. No local recurrence was observed at a maximum follow-up of 7 y (mean, 4 y 4 mo; range, 3–7 y) except for 1 patient (rT1 N0 M0), who died of local recurrence (survival period, 3 y 10 mo). Three patients died of distant metastasis (survival periods, 1, 1, and 6 y) and 1 patient died of pneumonia (survival period, 1 y). The remaining 18 patients (78.2%) now survive free of cancer. The 3-y survival rate was 87%.
DISCUSSION
The clinical utility of 18F-FDG PET has been well established in the detection and staging of head and neck cancers (6,7). However, few studies have reported the sensitivity of 18F-FDG PET in detecting malignant tumors compared with that of conventional diagnostic modalities—for example, functional images, such as 67Ga and bone scintigraphy, as well as anatomic images, such as CT and MRI. Our study demonstrated that 18F-FDG PET was more sensitive (sensitivity, 100%) with a high confidence level (grade 4, n = 22; grade 3, n = 1) than was MRI (78.3%), CT (68.2%), and 67Ga scintigraphy (40%) in detecting pretreatment primary tumors of the head and neck region, probably because of the high metabolic activity of the tumor (16,17). Previous reports (18–21) showed that 18F-FDG PET had a higher sensitivity (range, 78%–100%) than did CT and MRI (57%–82%), which is in agreement with our data.
Both 67Ga and bone scintigraphy have been widely used for detection of distant or bone metastases as well as primary tumors. Although 67Ga scintigraphy detected relatively large primary tumors in 8 of 20 patients, evaluation of tumor extent was not possible. We did not perform 67Ga SPECT, although it would improve the diagnostic accuracy. In contrast, 18F-FDG PET clearly visualized the tumor extent that fully corresponded to CT or MRI findings. Furthermore, 18F-FDG PET detected small tumors that were not detected by CT or MRI but were apparent by visual inspection. As for the whole-body evaluation, we have previously shown that whole-body 18F-FDG PET images had a clinical impact on the management of patients with head and neck cancer by reliably detecting secondary primary malignancies as well as distant metastases (22). 18F-FDG PET with whole-body imaging would replace the conventional functional imaging modalities of 67Ga and bone scintigraphy.
18F-FDG PET has been used to monitor response to therapies in patients with head and neck cancers (4,23–30). To our knowledge, however, no report has described prospectively the diagnostic value of 18F-FDG PET in patients with head and neck cancer as a functional imaging modality in comparison with CT and MRI as morphologic modalities before and after treatment with a consistent regimen of combined intraarterial chemotherapy and radiotherapy as an organ preservation protocol. Four of 23 patients demonstrated residual tumors after the therapy. 18F-FDG PET had almost equal sensitivity (4/4; 100%) compared with CT (3/4; 75%) or MRI (3/3; 100%). However, in the remaining 19 patients with no viable tumor cells, the specificity of posttreatment 18F-FDG PET (17/19; 89.5%) was superior to that of CT (58.8%) and MRI (41.2%). A high false-positive rate was shown on posttreatment CT (7/17) and MRI (10/17). Therefore, CT or MRI does not reliably differentiate posttreatment tissue changes from the residual tumor. The floor of the mouth, the parapharyngeal space, the base of the tongue, and the cheek were the areas that were particularly difficult to assess using anatomic images because posttreatment fibrosis, diffuse edematous swelling, and granulation tissue demonstrated such contrast enhancement that we could not differentiate the persistent residual tumor. This will be a problem especially when we make a decision regarding further treatment on the basis of anatomic images after chemoradiotherapy. 18F-FDG PET correctly identified residual tumors independent of their size and site and was also superior to anatomic imaging modalities in excluding residual tumors. We concluded that increased 18F-FDG uptake on PET images obtained >4 wk after treatment strongly indicated the presence of residual tumor, whereas the absence of 18F-FDG uptake suggested that no viable tumor remained.
Assessment for possible metastases to the neck lymph nodes is important in determining further treatment for each patient. Precise assessment of the neck region may avoid unnecessary surgery in patients without metastases to lymph nodes. Several studies (31–34) showed that 18F-FDG PET detected metastases to neck lymph nodes at a high sensitivity (range, 72%–91%) and specificity (82%–99%) in patients with head and neck carcinoma. But these patients underwent neither chemotherapy nor radiotherapy preoperatively, which might affect 18F-FDG uptake in the tumor. In our study, neck lymph nodes were histopathologically evaluated after combined intraarterial chemotherapy and radiotherapy, and no metastasis was confirmed in any patients, including 8 patients with suspected N (+) status by the pretreatment evaluation with imaging modalities. This finding may indicate the efficacy of our organ preservation regimen in treatment of metastases to the neck lymph nodes as well as the primary tumor (PCR rate, 82.6%). This is probably due to the high concentration of anticancer drugs in neck lymph nodes provided by intraarterial chemotherapy, together with concomitant neck irradiation. However, 18F-FDG PET after treatment demonstrated a focal 18F-FDG uptake in the neck region of 6 patients, which was assigned as a false-positive finding. For the primary lesions, there were only 2 false-positive cases after therapy. As a result, specificity of posttreatment 18F-FDG PET (17/23; 73.9%) was not better than that of MRI (17/20; 85%) or CT (16/21; 76.2%) for the neck region (Table 4). A focal 18F-FDG uptake in these patients was probably attributable to the reactive or inflammatory process in the neck lymph nodes, which might persist for a longer period than that in primary sites after intraarterial chemoradiotherapy. Follow-up 18F-FDG PET 3 mo after therapy showed no abnormal uptake in the neck of patients with false-positive findings and there was no recurrence in neck lymph nodes for >3 y.
The use of functional information obtained by 18F-FDG PET for therapeutic planning is promising. Familiarity with the complex anatomy of the head and neck is essential for accurate interpretation of 18F-FDG PET images because functional images alone often do not provide sufficiently detailed anatomic information describing the surrounding normal structures that is necessary for therapeutic planning. Although 18F-FDG PET provides information not available by means of MRI or CT, it cannot replace these anatomic modalities. In our facility, image coregistration between 18F-FDG PET and CT or MRI has been available recently and has been used clinically in selected cases (35). We conclude that serial 18F-FDG PET and MR or CT images are essential for the management of head and neck cancer treated by an organ preservation protocol such as combined intraarterial chemotherapy and radiotherapy.
Precise evaluation of the presence or absence of residual viable tumor is particularly important to the preservation of oral organs and functions by avoiding surgery or performing a reduced form of surgery after neoadjuvant chemoradiotherapy. In our previous study, we showed the significance of quantitative analysis of 18F-FDG PET in patients with head and neck cancer before and after the same intraarterial chemotherapy and radiotherapy (4). The SUV before the therapy is useful for predicting the response to the treatment, whereas the SUV after the therapy is useful for diagnosing the presence or absence of residual tumor. This study confirmed these findings regarding the SUV and further indicated the significance of the diagnostic values of 18F-FDG PET by comparing it with anatomic images. We attempted to determine further treatment on the basis of the 18F-FDG PET data. In 8 patients assigned a complete response with posttreatment SUVs of <4.0, we were able to avoid surgery. The remaining 15 patients underwent a reduced form of surgery with clinical advantages of a lower risk of damaging esthetics and a greater preservation of oral functions. The follow-up data at 3 y after the treatment revealed no local recurrence in all patients, which confirmed the validity of our use of 18F-FDG PET in determination of further treatment after neoadjuvant chemoradiotherapy. Furthermore, the 3-y survival rate was 87%. These results indicate that 18F-FDG PET is a powerful tool for accurate assessment of the therapeutic effect, which is essential for planning further treatment with reducing the risk of surgery and preserving appearance and functions. In this way, 18F-FDG PET can contribute to the improvement of the quality of life of patients with head and neck cancers.
CONCLUSION
Neoadjuvant intraarterial chemotherapy combined with radiotherapy is an effective presurgical treatment for reducing a risk of surgery and preserving oral functions in patients with head and neck cancer. 18F-FDG PET has a clinical impact on patient management by facilitating differentiation of residual tumors from treatment-related changes after the chemoradiotherapy, which is sometimes difficult to characterize by means of anatomic images. 18F-FDG PET will contribute to the improvement of the quality of life of patients with head and neck cancers by aiding in the selection of the optimal treatment option for each patient.
Acknowledgments
This study was supported in part by a Grant-in-Aid for Scientific Research (C11671982) from the Ministry of Education, Science, Sports and Culture, Japan.
Footnotes
Received Apr. 26, 2002; revision accepted Sep. 17, 2002.
For correspondence or reprints contact: Yoshimasa Kitagawa, DDS, PhD, Department of Dentistry and Oral Surgery, Fukui Medical University, Matsuoka, Fukui 910-1193, Japan.
E-mail: ykitagaw{at}fmsrsa.fukui-med.ac.jp
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Computed Tomography of Lymph Node Metastasis Before and After Radiation Therapy: Correlations With Residual Tumour
- The Value of PET Compared to MRI in Malignant Head and Neck Tumors
- Added Value of Baseline 18F-FDG Uptake in Serial 18F-FDG PET for Evaluation of Response of Solid Extracerebral Tumors to Systemic Cytotoxic Neoadjuvant Treatment: A Meta-Analysis
- Fluorodeoxyglucose-Positron-Emission Tomography Imaging of Head and Neck Squamous Cell Cancer
- 18F-FDG PET as a Routine Posttreatment Surveillance Tool in Oral and Oropharyngeal Squamous Cell Carcinoma: A ProspectiveStudy
- Does 18F-FDG PET/CT Improve the Detection of Posttreatment Recurrence of Head and Neck Squamous Cell Carcinoma in Patients Negative for Disease on Clinical Follow-up?
- False-positive positron emission tomography appearance with 18F-fluorodeoxyglucose after definitive radiotherapy for cancer of the mobile tongue
- Clinical Role of 18F-FDG PET/CT in the Management of Squamous Cell Carcinoma of the Head and Neck and Thyroid Carcinoma