


Abstract
The study aim was to assess the safety, biodistribution, tissue kinetics, and tumor uptake of the 99mTc-labeled neurotensin (NT) analog NT-XI. Methods: Four patients presenting ductal pancreatic adenocarcinoma were studied with 99mTc-NT-XI. Patients were followed by scintigraphy up to 4 h and by continued blood and urinary sampling until surgery 18–22 h after injection. Surgical tissue samples were analyzed for radioactivity uptake and NT receptor expression. Results: No side effects were observed on injection of 99mTc-NT-XI. Blood biologic half-lives α and β were 35 min (range, 17–62 min) and 230 min (range, 107–383 min), respectively. Repeated whole-body scintigraphy performed in 2 patients showed a single exponential decrease of whole-body activity with half-lives of 101 and 232 min. Tracer elimination was mainly renal, with 92% and 98% of activity counted in urine in the first 20 h. Kidney, liver, spleen, and bone marrow activity uptake was observed in all patients. Tumor was not visualized in the first 3 patients but could be localized by tomoscintigraphy in the pancreas head region of patient 4. In vitro tissue analysis showed high expression of NT receptor in the tumor of patient 4, correlated with the highest tumor radioactivity uptake and the highest tumor-to-fat radioactivity ratio. In vitro receptor expression was also positive in a second patient having a tumor characterized by very low cellularity; however, the remaining 2 tumors lacked NT receptor expression. Conclusion: Injection of 99mTc-NT-XI was well tolerated. The in vivo tumor uptake appeared specific as it was observed in the 1 patient with a pancreatic tumor that expressed high amounts of NT receptor. The results are compatible with preclinical animal results and in favor of further development of radiolabeled NT analogs for diagnosis or therapy of cancer.
Neurotensin (NT) receptor expression has been described in the central nervous system, the digestive tract, and different tumors. Of the 3 different receptor subtypes described, expression of subtype I, which shows high-affinity binding for NT, was observed in high frequency (75%) in ductal pancreatic adenocarcinoma (1,2). The situation is different in gastrointestinal cancer: Although colon cancer cell lines can express NT receptors (3), surprisingly, resected human gastrointestinal carcinomas are frequently devoid of NT receptors (4).
NT is a paracrine/endocrine peptide of 13 amino acids. Its carboxy-terminal part has been identified as the receptor-binding domain. NT-XI, used here, is a hexapeptide analog of the carboxy-terminus of NT covering the amino acid sequence 8–13. Compared with the natural peptide, 2 modifications have been introduced in NT-XI, resulting in increased stability: First, the natural peptide linkage between amino acids 8 and 9 has been replaced with a pseudopeptide linkage that is resistant to serum enzymes (5). Second, the natural isoleucine (amino acid 12) has been replaced with a tertiary leucine (Tle) (5).
The amino-terminus of NT-XI has been connected with an (NαHis)Ac group, allowing convenient and stable labeling with the 99mTc-tricarbonyl moiety (6). The same chemistry could allow coupling of therapeutic electron-emitting radioisotopes such as 186Re or 188Re to NT-XI. In this article, we use the short term 99mTc-NT-XI for the radiolabeled formulation of the NT analog: [99mTc(CO)3](NαHis)Ac-Lys-(ψCH2-NH)-Arg-Pro-Tyr-Tle-Leu.
99mTc-NT-XI has been shown to exhibit the same receptor affinity (dissociation constant [Kd] = 0.5 nmol/L) as the natural peptide (7). In comparison with other preclinically evaluated NT analogs (8), 99mTc-NT-XI has been shown to have a favorable tumor uptake and biodistribution in nude mice bearing HT-29 human colon carcinoma xenografts. These characteristics prompted our initial clinical evaluation of 99mTc-NT-XI.
MATERIALS AND METHODS
Patients
Four patients presenting ductal pancreatic adenocarcinoma on histologic examination were evaluated. Inclusion criteria included adequate renal and hepatic function (creatinine, ≤180 μmol/L; aspartate aminotransferase, ≤160 U/L). Patients gave their written informed consent to the study protocol that had been approved by the local Ethics Committee and the Swiss authorities (Swissmedic and Federal Office of Public Health, Section for Radioprotection). Injection of 99mTc-NT-XI was planned for the day preceding surgery.
NT Analog NT-XI and 99mTc Radiolabeling
NT-XI was synthesized by one of us. It covers the amino acid sequence 8–13 of native NT. Compared with the natural peptide, NT-XI presents 2 modifications: First, the natural peptide linkage between amino acids 8 and 9 has been replaced with a pseudopeptide linkage that is resistant to serum enzymes (5). Second, the natural isoleucine (amino acid 12) has been replaced with a tertiary leucine (Tle) (5).
Radiolabeling of NT-XI with 99mTc was performed using tricarbonyl chemistry as described (6) adopting the rules of good clinical practice. The amino-terminus of NT-XI has been connected with an (NαHis)Ac group (6). Chemicals were obtained from Fluka. The radiolabeling was done in 2 steps: Pertechnetate (generator eluate, 0.5–1 mL, 1 GBq) was first added to a mixture of 5.5 mg NaBH4, 4.0 mg Na2CO3, and 15 mg Na,K-tartrate under an atmosphere of CO. The solution was kept at 75°C for at least 15 min and then cooled to room temperature; the pH was adjusted to 6.0–6.5 with a mixture of HCl (1 mol/L) and phosphate buffer (0.6 mol/L). The 99mTc-tricarbonyl solution obtained was added to 0.03 mL of a 1 mmol/L NT-XI solution and heated again at 75°C for 1 h. Radiochemical purity was analyzed by high-performance liquid chromatography: column, LichroCART250-4 RP-18 (Merck); solvents: A = water (0.1% trifluoroacetic acid)/methanol = 85:15; B = acetonitrile/methanol = 95:5; flow, 1 mL/min; gradient: 0–7 min = 100% A; 7–20 min = 0%–100% B. The retention time (tR) of 99mTc-NT-XI = 17.95 min. All final injected preparations had a radiochemical purity of >96%. For each preparation, the binding capacity was tested in vitro using increasing concentrations of HT-29 cells (range, 6–200 × 104 cells) and 0.5 kBq 99mTc-NT-XI per well as described (9). The results (Kd = 0.6 ± 0.5 nmol/L) were compatible with the previously observed high affinity of 99mTc-NT-XI, including also a low nonspecific binding (∼1%).
Patient Injection and Data Collection
A defined activity of ∼400 MBq 99mTc-NT-XI, corresponding to ∼20 μg of peptide, was injected in patients under standard precautions, including frequent control of vital parameters. Starting with injection of radiopeptide, dynamic anterior and posterior abdominal scintigraphy of 30 min was recorded in the first 2 patients. It was followed by repeated static abdominal imaging and whole-body scintigraphies up to 4 h after injection. Patients 3 and 4 had anterior and posterior whole-body scintigraphy under standardized, controlled conditions immediately after radiotracer injection and 2 and 4 h after injection. Measurement of background activity and of a standard control radioactivity sample was performed with the same scanning parameters. Background-corrected whole-body activity and regions of interest of organs were determined on fused (geometric mean) anterior and posterior scintigraphies. Abdominal tomoscintigraphy was performed in 3 patients 3 h after tracer injection. Blood samples were obtained previous to and 5, 10, 15, 30, 45, and 60 min and 2, 4, and ∼20 h after injection. Complete urinary sampling until surgery was obtained from patients 2 and 3.
Tissue, blood, and urinary radioactivity was determined in a γ-counter together with a standard radioactivity sample allowing back-determination of tissue or body fluid activity in comparison with injected activity (percentage of injected dose per gram [%ID/g]).
Blood half-lives α and β were determined using nonlinear regression of measured activity in a 2-compartment model with (activity−1) weighting, according to the formula:
 In this equation, A1 is the fractional activity exhibiting half-life α = ln 2/λ1 and A2 is the fractional activity exhibiting half-life β = ln 2/λ2.
In this equation, A1 is the fractional activity exhibiting half-life α = ln 2/λ1 and A2 is the fractional activity exhibiting half-life β = ln 2/λ2.
Activity eliminated in the urine was determined in fractions collected between injection time until surgery. Whole-body and organ activities were fitted to a single exponential curve.
Surgery
Patients had surgery 18–22 h after radiotracer injection. Complete tumor resection was performed where clinically indicated. From the other patients, biopsies were obtained for histologic analysis and radioactivity determination. Normal tissue samples (including a standard fat sample from all patients) were removed according to clinical indication. Part of the tumor tissue was rapidly deep-frozen in liquid nitrogen for determination of NT receptor expression as described (1,4).
Preliminary Dosimetry
Preliminary dosimetry was performed with MIRDOSE3.1 (10) using Windows 95 (Microsoft) (MIRDOSE3.1 is not compatible with Windows versions later than Windows 98). Calculation was performed on data obtained from patients 3 and 4 based on repeated whole-body scintigraphies that allowed determination of residence times for whole body, liver, kidneys, and spleen up to 4 h after injection. Regions of interest were determined based on the geometric mean of anterior and posterior scintigraphies. Abdominal background activity was determined and subtracted for determination of spleen and kidney activity. Beyond 4 h, residence times were calculated on the basis of tissue half-lives set equal the whole-body half-life as determined from urinary elimination (patient 3) or by introducing the blood half-life β (patient 4). Bone marrow (1,120 g in the standard 70-kg human phantom) activity concentration was calculated in 2 ways by setting it equal either to spleen or to blood activity. The MIRDOSE3.1 (10) dynamic bladder model was used to calculate the residence time of urinary bladder content: The urinary elimination fraction was set = 1 (based on urinary collection data); the biologic half-time was determined from urinary elimination (patient 3) or from whole-body scintigraphy (patient 4). The bladder voiding interval was set at 3 h.
RESULTS
Four patients, 44–69 y old (Table 1), were included in the study after giving their written informed consent. Patients presented ductal pancreatic adenocarcinoma, with differentiation being low (1 patient), intermediate (1 patient), and high (2 patients; Table 1). No side effects were observed on injection of 99mTc-NT-XI or during the following week.
Patient Characteristics
Scintigraphy
Initial dynamic scintigraphy performed during 30 min in the first 2 patients and early whole-body scintigraphy in the next 2 patients did not reveal any particular radiotracer distribution. Tracer moved rapidly from the blood compartment immediately after injection into tissues. Kidney and, to a lesser extent, liver, spleen, and bone marrow uptake was observed in all patients. Whole-body scintigraphy 2 and 4 h after injection showed continued tracer elimination through the kidneys and remaining activity in the organs mentioned above. Significant digestive tract activity was observed in patients 2 and 4.
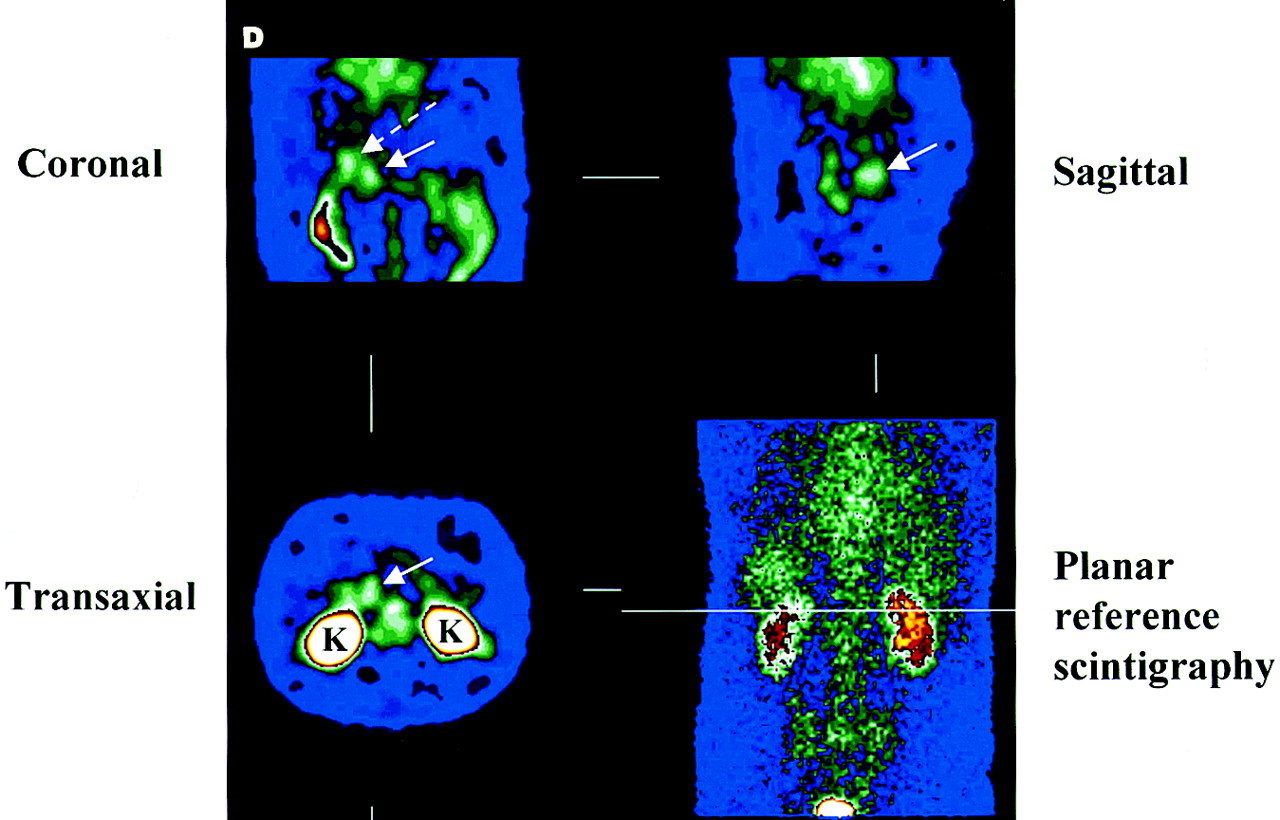
No tumor uptake was identified in the first 3 patients. In patient 4, a moderate tracer uptake in the epigastric region could be observed 2 and 4 h after injection (Figs. 1A–C). According to SPECT, the hyperactivity correlated with the known tumor site in the pancreatic head and the adjacent duodenum (Fig. 1D). Because of surgery, no scintigraphy beyond 4 h after injection could be obtained. Thus, nonspecific tissue activity, especially in the kidneys, was quite high according to the elimination profile of 99mTc-NT-XI and compromised reading of planar scintigraphies.


Whole-body anterior scintigraphies (anterior on left, posterior on right) recorded 0.2 h (A), 2 h (B), and 4 h (C) after injection and abdominal tomoscintigraphic sections (D) recorded 3 h after injection of patient 4. Solid arrow shows pancreatic head tumor; dashed arrow indicates duodenum. K = kidneys.
Determination of Tumor Receptor Density and Tracer Uptake
In vitro tissue analysis demonstrated high-density NT receptor expression in the tumor of patient 4 (Fig. 2). The highest 99mTc-NT-XI tumor radioactivity uptake of 9.1·10−4 %ID/g was measured in the surgical tissue samples of this patient, counted in vitro, as well as the highest tumor-to-fat radioactivity ratio of 20.3:1 (Table 2). The tumor-to-blood radioactivity ratios in the 4 patients might have been partially biased due to variable blood half-lives (Table 3). Lower tumor uptake of 99mTc-NT-XI was observed in patients 1–3. The in vitro NT receptor status was positive in 1 of these 3 patients having a tumor characterized by a very low cellularity. The remaining 2 patients had NT receptor–negative tumors (Fig. 2).

In vitro autoradiographic evaluation of NT receptor expression in tumor samples of patients 3 and 4. Tumor of patient 4 (A, C, and E) had very high density of NT receptors, whereas tumor of patient 3 (B, D, and F) was devoid of NT receptors. (A and B) Sections stained with hematoxylin–eosin. Arrows indicate ductal pancreatic cancer. Bars = 1 mm. (C and D) Autoradiograms show total binding of 125I-Tyr3-NT. Neoplastic pancreatic ducts (arrows) are strongly labeled in C but not in D. (E and F) Autoradiograms show absence of nonspecific binding in presence of 10−6 mol/L NT.
Tissue Radioactivity Uptake Determined in Surgical Tissue Specimen Obtained Between 18 and 22 Hours After Injection
Blood Biologic Half-Lives of 99mTc-NT-XI
Blood and Whole-Body Half-Lives of 99mTc-NT-XI
Blood biologic half-lives were determined by repeated blood sampling and fitting the count values to a 2-compartment model. The half-lives α and β in the 4 patients were of 35 min (range, 17–62 min) and 230 min (range, 107–383 min), respectively (Table 3; Fig. 3). It appears that for patients 2 and 3, late blood activity remained high compared with the predicted curve (Fig. 3), suggesting that a third compartment might exist. Because of limited blood sampling at late times, the third half-life could not be determined. However, this late fraction would probably represent <2% of initial activity and, therefore, remain negligible.
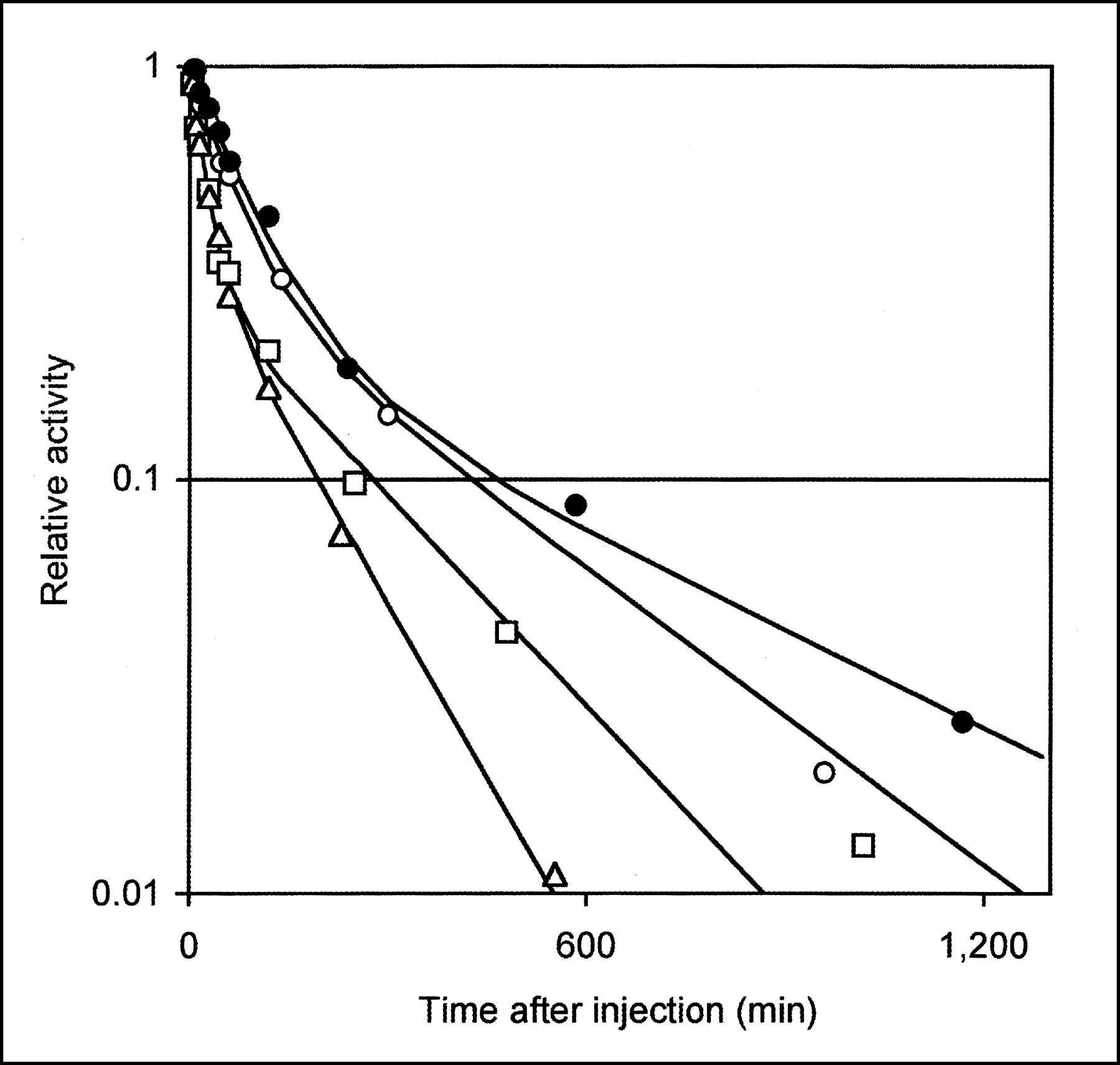
Relative blood time–activity curves, normalized to initial activity. Patient 1, ○; patient 2, □; patient 3, ▵; patient 4, •. Double exponential curves were fitted on 2-compartment model and biologic half-lives α and β were determined (Table 3).
Repeated whole-body scintigraphy was performed in patients 3 and 4 using standardized controlled conditions, including determination of background activity and of a standard radioactivity sample for all scintigraphies. This allowed calculation of the whole-body activity half-life. For the 2 patients, a single exponential curve with a biologic half-life of 101 and 232 min, respectively, was found. Urinary radioactivity was determined in fractions collected until surgery in 2 patients. Urinary activity represented 93% and 98% of injected activity, respectively, suggesting that renal filtration represents the predominant elimination pathway of 99mTc-NT-XI and its degradation products.
Preliminary Dosimetry
Preliminary dosimetry using MIRDOSE3.1 was performed for 2 patients (patients 3 and 4) based on controlled repeated whole-body scintigraphies. For a 70-kg patient (standard human phantom), an effective dose (ED) of 5.8 and 5.6 μSv/MBq was indicated, according to the data of the 2 patients, respectively. These results are comparable with those published by the International Commission on Radiological Protection radiation task group for other small 99mTc-labeled imaging agents such as citrate (ED = 6.1 μSv/MBq) or penicillamine (ED = 7.3 μSv/MBq) (11,12). The highest tissue radiation doses for the 2 patients were observed for urinary bladder (49 and 38 μGy/MBq), kidneys (10.3 and 10.5 μGy/MBq), and liver (2.1 and 3.0 μGy/MBq). If bone marrow activity concentration was set equal to blood activity, its radiation dose was calculated as 1.5 and 2.1 μGy/MBq, respectively, for the 2 patients. The dose would be higher with 1.9 and 3.2 μGy/MBq, respectively, if bone marrow activity concentration was set equal to that of spleen.
DISCUSSION
99mTc-NT-XI was selected for this initial clinical study on the basis of its conserved high binding affinity to the NT receptor and favorable results of stability and biodistribution observed in vitro and in preclinical animal studies. In the 4 patients, a moderate but significant radiotracer uptake has been observed in kidneys and, to a lesser degree, in liver, spleen, and bone marrow. This distribution is compatible with the preclinical animal results observed in tumor-bearing nude mice (7,13). Liver, kidney, and spleen activities probably represent nonspecific accumulation according to the preclinical animal data, because this uptake could not be inhibited by administration of excess amounts of unlabeled NT. Furthermore, this nonspecific activity was variable depending on the formulation of the NT analog (13,14).
Interestingly, the highest tumor radiotracer uptake of 9.1·10−4 %ID/g was observed in the tumor of patient 4. In vitro autoradiography showed high receptor expression of this tumor with a high cellularity. In the 3 other patients, less tumor radioactivity uptake was measured (1.9–3.9·10−4 %ID/g), leading to low tumor-to-normal fat and tumor-to-liver radioactivity ratios. Although patient 2 had tumor NT receptors expressed, as determined in vitro, it was, rather, the very low cellularity of this tumor that may have prevented its in vivo visualization and the low radioactivity uptake measured in the surgical tissue sample.
However, the favorable uptake of 99mTc-NT-XI in the tumor of patient 4 is counterbalanced by the observation of a significant radioactivity uptake in the intestinal tissue of this patient. According to scintigraphy, digestive tract radioactivity varied significantly among the 4 patients, with patients 2 and 4 showing significant uptake. This intestinal radioactivity uptake was observed in the 2 patients who had tumors with positive receptor expression. Though, theoretically, part of the intestinal activity could represent released 99mTc, the absence of significant thyroid activity in the 4 patients argues against this hypothesis. Therefore, intestinal radioactivity might represent specific uptake of 99mTc-NT-XI. The in vitro measurement of high concentrations of radioactivity in normal tissue samples of the stomach and duodenum of patient 4 is another argument in favor of the specificity of this uptake. Furthermore, preclinical animal studies have shown that intestinal uptake of another 99mTc-labeled NT analog could be inhibited by coadministration of excess amounts of unlabeled NT (8). In the absence of further data, the question of the frequency and relevance of intestinal tissue uptake of NT analogs remains open after this initial study in patients.
NT receptor expression has been also described for the central nervous system. Uptake of 99mTc-NT-XI in this organ was not observed. It is possible that 99mTc-NT-XI does not cross the blood–brain barrier.
CONCLUSION
The results of this initial study of a radiolabeled NT analog in patients show a remarkable analogy with preclinical in vitro and in vivo findings. First, the tumor uptake measured at ∼20 h after injection in the single patient for whom receptor positivity and high cellularity were shown was in the range of that expected from tumor xenograft experiments, taking into account the ∼3,000-fold difference in body weight between humans and mice (and, accordingly, a higher dilution of injected peptide in patients). Second, the half-lives of the radiopeptide in the whole body and the half-lives β in blood were in the range of 1.7–6.3 h, suggesting that the peptide had been stabilized efficiently with the 2 modifications introduced. Third, high nonspecific uptake of 99mTc-NT-XI was observed in the kidneys of mice, which, unfortunately, was also predictive for human application of this peptide. These data suggest that larger patient studies or studies with different radiolabeled NT analogs are indicated to further elucidate the relevance of uptake in tumor and in the digestive tract.
Acknowledgments
We gratefully acknowledge the expert support of this study by Prof. Pius August Schubiger, Paul Scherrer Institute, Villigen, Switzerland, and the Swiss Technology Institute of Zurich, Zurich, Switzerland, as well as Prof. Michel Gillet for advising the patients for this study. Furthermore, we acknowledge the technical assistance of Corinne Paschoud, Monique Bezençon, and Alain Blanc. This work was funded, in part, by the European study grant Biomed 2 project BMH4-CT98-3198 (BBW 96.0447-1).
Footnotes
Received Mar. 10, 2003; revision accepted Jun. 13, 2003.
For correspondence or reprints contact: Franz Buchegger, MD, Division of Nuclear Medicine, University Hospital of Lausanne, CH 1011 Lausanne, Switzerland.
E-mail: Franz.Buchegger{at}chuv.hospvd.ch
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Targeting Neuropeptide Receptors for Cancer Imaging and Therapy: Perspectives with Bombesin, Neurotensin, and Neuropeptide-Y Receptors
- Facile Preparation of a Thiol-Reactive 18F-Labeling Agent and Synthesis of 18F-DEG-VS-NT for PET Imaging of a Neurotensin Receptor-Positive Tumor
- Synthesis and biological activity of stable branched neurotensin peptides for tumor targeting
- First Evaluation of a 99mTc-Tricarbonyl Complex, 99mTc(CO)3(LAN), as a New Renal Radiopharmaceutical in Humans
- Candidates for Peptide Receptor Radiotherapy Today and in the Future