


Abstract
186Re-1,1-hydroxyethylidene diphosphonate (etidronate) can be used for the palliative treatment of metastatic bone pain. A randomized, placebo-controlled study using 186Re-etidronate was conducted on end-stage prostate cancer patients with metastatic bone pain. Methods: Pain relief was assessed using an electronic diary containing questions reflecting the multidimensional character of chronic pain. The diary was marked twice daily for a maximum of 14 wk (2 wk before and 12 wk after the injection). Pain response was determined using a specific decision rule in which pain intensity, medication index, and daily activities were the core determinants. A positive response day was defined as a day on which pain intensity was reduced ≥25% compared with baseline values, while medication index and daily activities were at least constant, or on which pain intensity was reduced < 25% and medication index or daily activities improved ≥25%, without worsening of the remaining factor. The total response (%) was defined as the number of positive response days divided by the number of days of follow-up. Results: Of the 111 included patients, 79 were evaluable (43 186Re-etidronate, 36 placebo). Thirty-two patients were excluded from the analysis because of incomplete datasets. The total response of the patients treated with 186Re-etidronate varied from 0% to 96% (mean, 27%, or 23/84 d). In the placebo group, the total response varied from 0% to 80% (mean, 13%, or 11/84 d; Mann-Whitney U test, P < 0.05). The number of patients who requested radiotherapy was higher in the placebo group (67%) than in the 186Re-etidronate group (44%) (relative risk, 1.51; Fisher’s exact test, P = 0.069). Conclusion: This randomized controlled trial confirmed that, compared with placebo, 186Re-etidronate resulted in a significantly longer pain response in the treatment of bone pain from metastasized prostate cancer.
In The Netherlands, prostate cancer is diagnosed in nearly 20% of all male cancer patients annually, especially those older than 60 y. Autopsy series have reported that up to 85% of patients with advanced prostate and breast cancer had evidence of skeletal metastases at the time of death (1,2). Multiple painful bone metastases are a frequent problem in these patients. Initially, the primary palliative treatment options are the use of conventional nonsteroidal antiinflammatory drugs or narcotics and local-field radiotherapy. Allen et al. (3) reported that complete pain relief occurred in 42% of patients and partial relief in 35% after receiving local-field external-beam radiotherapy. However, synchronous multiple bone metastases secondary to prostate cancer are not uncommon and are subsequently less suitable for local-field radiotherapy.
Alternatively, systemic radionuclide therapy using bone-seeking agents can be used to treat painful metastases. The advantage of targeted radionuclide therapy is that all affected areas are treated simultaneously, with relative sparing of the surrounding tissue. Early experience was gained with 32P-phosphate, but one of the major drawbacks to routine use of 32P-phosphate has been the considerable myelosuppressive toxicity (4). More recently, several studies have reported good pain relief with different radiopharmaceuticals, including 89Sr-chloride, phosphonates labeled with 153Sm, and hydroxyethylidene diphosphonate labeled with 186Re-etidronate (Table 1) (5–10).
Radiopharmaceuticals for Palliative Treatment of Painful Bone Metastases
186Re-Etidronate is a combined β- and γ-emitter with a maximum β-emission of 1.07 keV. It has a 9% abundant γ-ray of 137 keV, which is suitable for imaging as well. 186Re-etidronate, with its relatively short physical half-life of 3.8 d, may produce a faster onset of pain relief and a higher dose rate than are possible for radionuclides with a longer half-life. Another consideration is that 186Re-etidronate is also suitable for repetitive treatment (11,12).
However, few studies have investigated the palliative treatment of painful bone metastases with radiopharmaceuticals in a double-blind, randomized, placebo-controlled fashion and using a computer-assisted, standardized, objective method of pain assessment. Therefore, this study was undertaken to assess the efficacy of 186Re-etidronate in endocrine-refractory prostate cancer patients with metastatic bone pain in a placebo-controlled trial.
MATERIALS AND METHODS
The Placorhen study (acronym for Placebo Controlled Rhenium Study) was performed at the University Medical Center Utrecht, Utrecht, The Netherlands, to evaluate 186Re-etidronate for the palliative treatment of painful bone metastases. This study was double-blind and placebo-controlled and had the following objectives: evaluation of the efficacy of 186Re-etidronate in prostate cancer patients with metastatic bone pain, using strict criteria to assess treatment response with a validated multidimensional pain model (13), and evaluation of the number of patients requiring additional external-beam radiotherapy.
Study protocols were approved by the Institutional Review Board of the University Medical Center Utrecht. All patients gave written informed consent. Patients were randomly allocated to receive either 186Re-etidronate or a placebo intravenously. Randomization was performed by the hospital pharmacist using a predetermined randomization list from the Center for Biostatistics, University of Utrecht, Utrecht, The Netherlands. He was the only person during the entire study who knew what therapy was prepared and given.
Inclusion Criteria
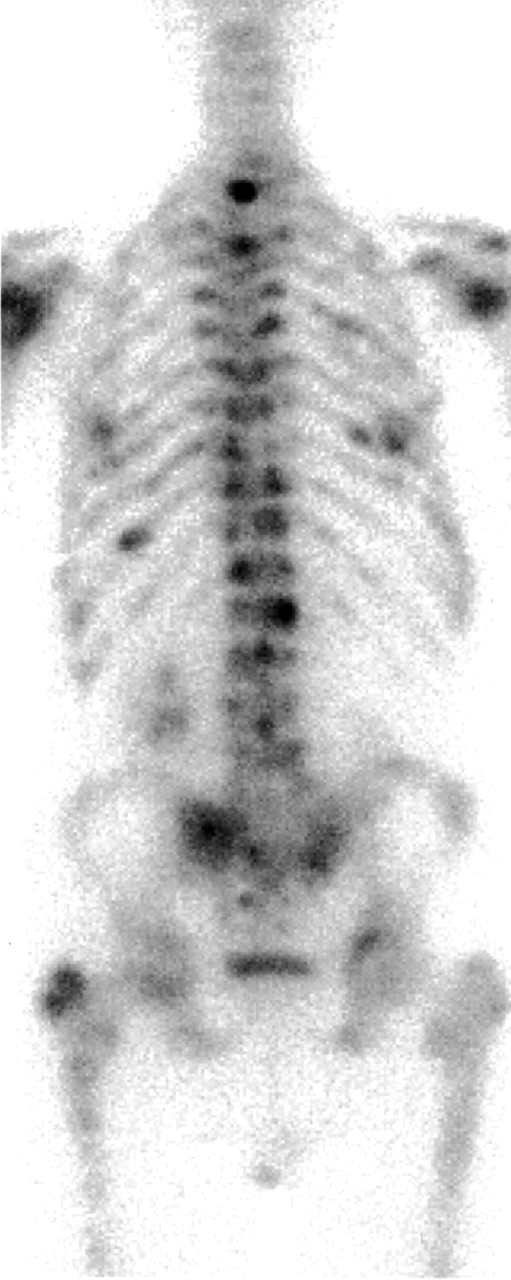
All patients needed to have histologically or cytologically proven prostate cancer with symptomatic bone metastases no longer responding to any medical or surgical endocrine manipulation treatments. All patients had scintigraphic and radiologic evidence of at least 4 bone metastases (Fig. 1). Each patient had adequate hematologic function, with a leukocyte count > 4.0 × 109/L, a platelet count > 150 × 109/L, and an adequate renal function (plasma creatinine levels < 130 μmol/L). Performance status, measured according to the scale of Karnofski et al. (14), had to be ≥60%, and estimated life expectancy had to be >3 mo.

Scintigraphy of prostate cancer patient with multiple bone metastases.
Patients with bone metastases from malignancies other than prostate cancer were not included in this study. Other reasons for patient ineligibility were rapidly progressive or life-threatening metastatic disease, overt central nervous system metastasis producing spinal cord compression, congestive heart failure (American Heart Association grade III/IV), significant arrhythmia or complete bundle branch block, active uncontrolled infection, participation in other clinical trials within 30 d before therapy, an immediate threat of mechanical complications such as spinal cord compression or impending hip fracture, diphosphonate therapy within 3 wk before treatment, or a change in or termination of hormone therapy (including corticosteroids) < 2 wk before treatment.
Treatment
All patients were hospitalized during the day of administration in an isolated room at the Department of Nuclear Medicine, University Medical Center Utrecht. The radioactive material was 186Re-etidronate (Mallinckrodt Medical BV, Petten, The Netherlands) supplied in 2-mL vials, and the placebo contained a solution of isotonic sterile saline in 2-mL vials. The administration was performed by a bolus injection through a running intravenous saline drip. The infusions were identical in appearance after preparation to ensure blinding. Other study personnel, as well as the patient and investigators, remained unaware of the treatment assigned during the entire study. The preparation of 186Re-etidronate was reported in detail previously (15). Doses were calculated for all patients according to de Klerk et al. (16). The administered dosage in this study varied from 1,295 to 2,960 MBq (35–80 mCi). Repeated treatment was not allowed because this was not ethical for those patients who had received a placebo without sufficient pain relief.
Patients were informed that additional radiotherapy could be requested at any time during the entire 12-wk study, based on the personal experience of the patient’s pain index. No standard instructions were given on alteration of the intake of analgesics.
Pain Assessment
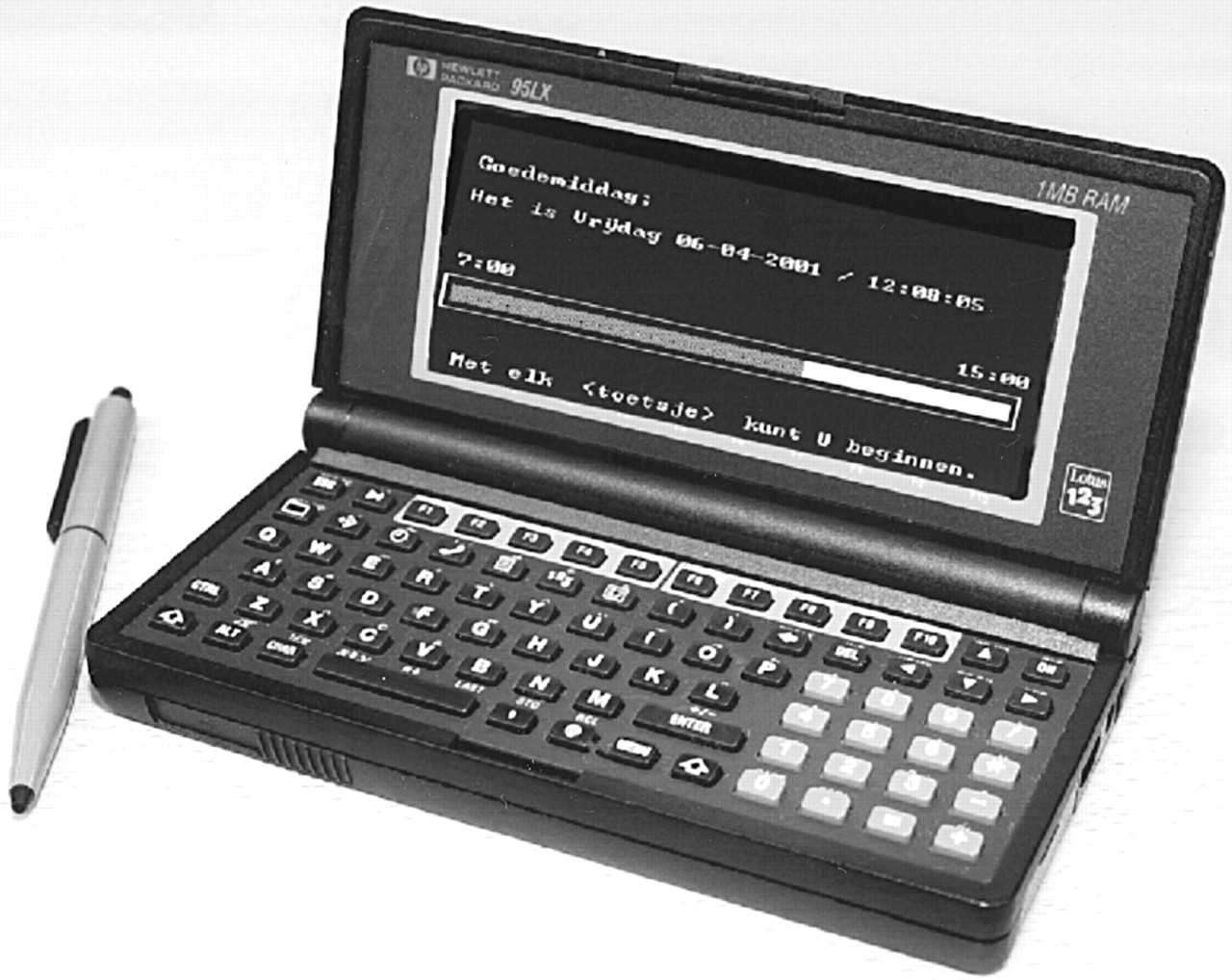
The patient assessed pain twice daily using an electronic palm-top computer diary known as a personal digital assistant (Fig. 2). Data collection started 2 wk before treatment and continued until 84 d (12 wk) after treatment or until the request for radiotherapy. Patients were instructed to make entries in their electronic diary every morning and evening at predetermined times for pain assessment at home during the entire study. Because cancer pain is a multidimensional phenomenon, the personal digital assistant asked questions related to the patients’ “sensoric” pain and the patients’ “behavioral” dimension of pain. The visual analog score can be explained by a ruler with a scale from 0 mm (no pain) to 100 mm (unbearable pain) to assess the pain intensity. The sensoric pain intensity was entered into the personal digital assistant using this scale. The behavioral aspect of pain was evaluated by multiple validated questions about the patients’ daily activities (16). Because analgesic intake directly influences pain intensity, a validated medication index was used to register daily pain medication intake (17,18). This analgesic conversion table was published earlier by our group (19).
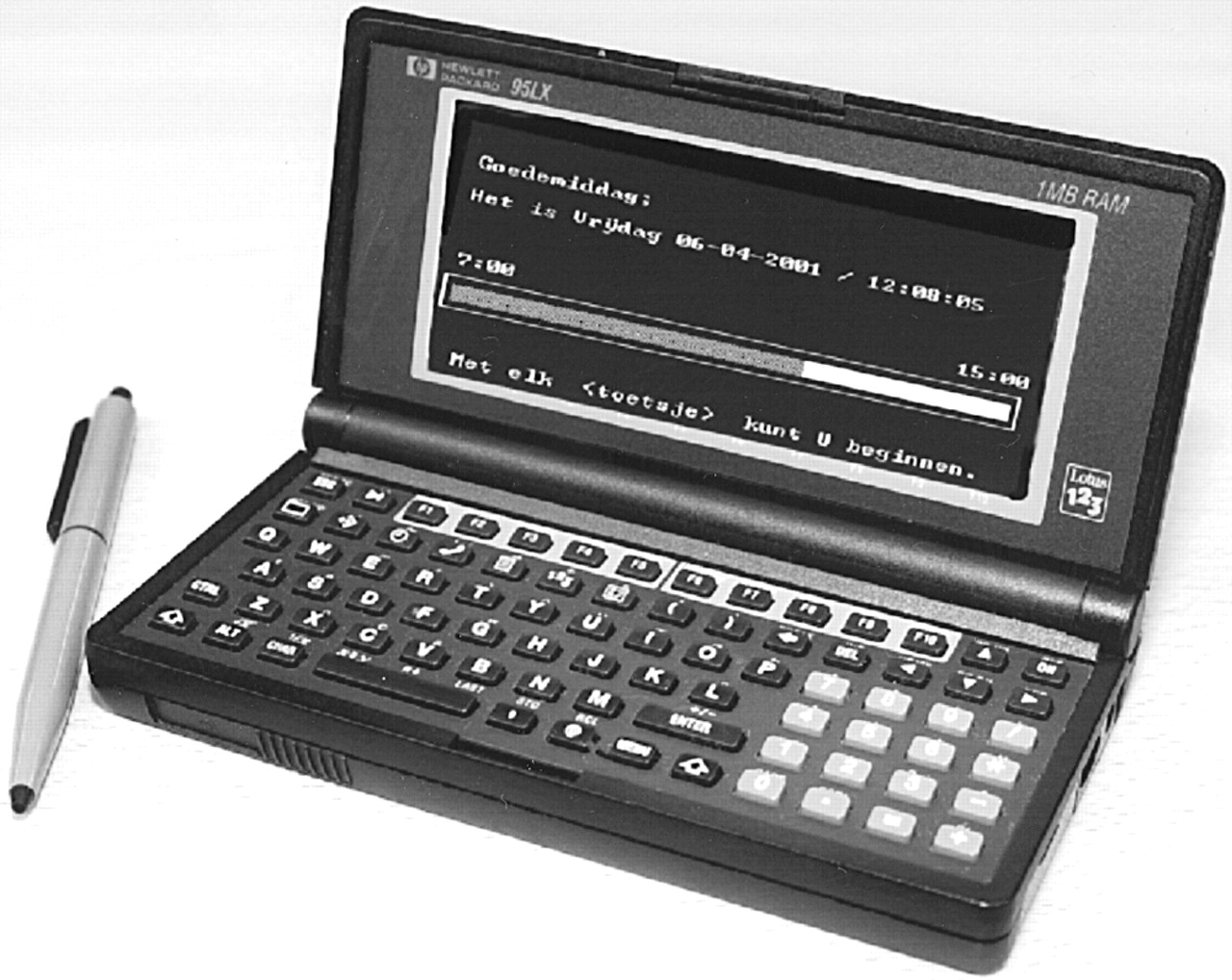
Electronic palm-top computer diary (personal digital assistant).
To assess the baseline levels of pain intensity, medication index, and daily activities, the median scores were calculated from the data collection that occurred 2 wk before treatment. Patients were seen by a single clinician in the outpatient ward every 3 wk during the 3 mo after treatment.
The primary endpoint was the number of positive response days, assessed by the electronic pain diary during the 84-d follow-up after injection. A positive response day was defined as a day on which pain was reduced ≥25% compared with the median baseline pain index value, while the medication index and daily activity score remained constant or increased, or on which pain was reduced <25% and the medication index or daily activity score improved ≥25% compared with baseline levels, without worsening of the remaining factor. Secondary endpoints were survival or a request for additional external radiotherapy because of persistent or intolerable pain.
Additional Clinical Data
The bone scan index as described by Blake et al. (20) was determined for every patient before therapy to provide an index of the extent of metastatic disease. The latest prostate-specific antigen levels before therapy were recorded as well. Serum bone alkaline phosphatase levels were obtained at baseline. Hematologic samples were drawn at 3-wk intervals.
Statistical Analysis
Data were analyzed using SPSS software (version 9.0; SPSS Inc., Chicago, IL) for Windows (Microsoft, Redmond, WA). Descriptive statistics, the Fisher exact test for comparison of independent samples, and the Student t test were used to assess pretreatment differences between treatment groups. The Mann-Whitney test was used to compare the proportional response days (fraction of positive response days in the total days after therapy) between both treatment groups. The visual analog score, daily activities, and medication index were also analyzed separately using repeated-measures ANOVA. The time of request for radiotherapy during follow-up was evaluated with a Cox proportional hazards model. P < 0.05 was considered to indicate statistical significance.
RESULTS
From August 1993 until September 1999, 131 men were eligible and randomized for this single-center study (Fig. 3). Twenty patients did not receive any drug (placebo or rhenium) because of withdrawal or acute readmission to the hospital for various reasons. Thus, a total of 111 patients were enrolled in this study. Another 32 patients (16 placebo and 16 rhenium patients) who did receive any treatment were excluded from further statistical analysis because of incomplete datasets at baseline or insufficient (<50% follow-up data available) follow-up scores during the 12 wk after therapy. Finally, 79 men (36 patients [46%] in the placebo group and 43 patients [54%] in the 186Re-etidronate group) were evaluable for analysis.

Placorhen study flowchart of randomized patients in placebo and rhenium groups.
All patients had histologically proven prostate cancer. Patient characteristics and pretreatment baseline scores are given in Table 2. There were no statistical differences in age, height, weight, bone scan index, or prostate-specific antigen values between the 2 treatment groups. The mean Karnofski score was 86 in the rhenium group and 87 in the placebo group. Five patients (all in the rhenium group) died—after 6, 7, 9, and 11 wk (2 patients)—during the 12-wk follow-up. Death was caused by clinical deterioration of the patient’s condition (in 4 patients) or by euthanasia (in the 1 patient who requested it). The number of deaths was not statistically different between the 2 groups (Fisher exact test, P = 0.06).
Patient Characteristics and Baseline Scores in 186Re-Etidronate Group Compared with Placebo Group
Univariate analysis did not show any correlation between bone scan index or prostate-specific antigen values at baseline and clinical response in either group. Pretreatment pain intensity scores were statistically not different between the treatment groups. The mean baseline (2 wk before therapy) pain intensity score ± SD according to the visual analog score was 45.3 ± 24.8 in the rhenium group and 43.2 ± 23.0 in the placebo group.
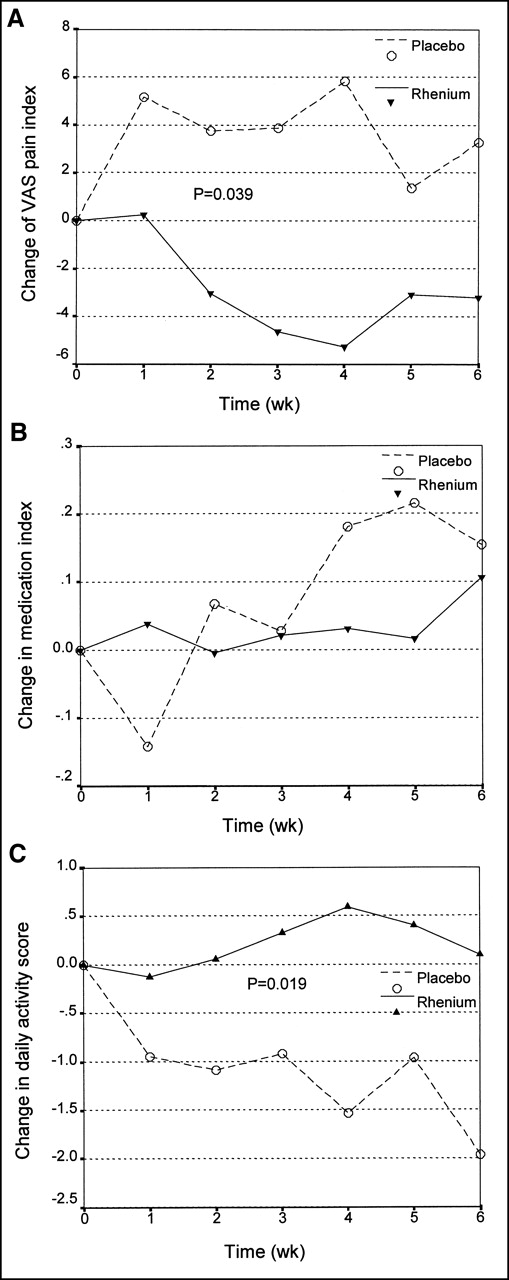
The course of the pain index, medication index, and daily activity score in the placebo and rhenium groups before therapy and after 2, 4, and 6 wk after therapy is depicted in Figure 4. The change in the pain index after treatment was significantly different (P = 0.039) between the treatment groups. In the placebo group, the mean pain index increased during the study, whereas the mean pain index score in the rhenium group decreased. The mean visual analog score at baseline (2 wk before injection) was not correlated with the percentage of response. The change in the daily activity score between the treatment groups was also significantly (P = 0.019) in favor of the rhenium group. The mean daily activities in the placebo group gradually decreased, whereas the daily activities in the rhenium group remained stable or increased during follow-up. No difference in medication index was noted between the treatment groups during follow-up.

Change in visual analog score (A), medication index (B), and daily activity (C) in placebo group and rhenium group during follow-up. VAS = visual analog score; 0 = time at baseline.
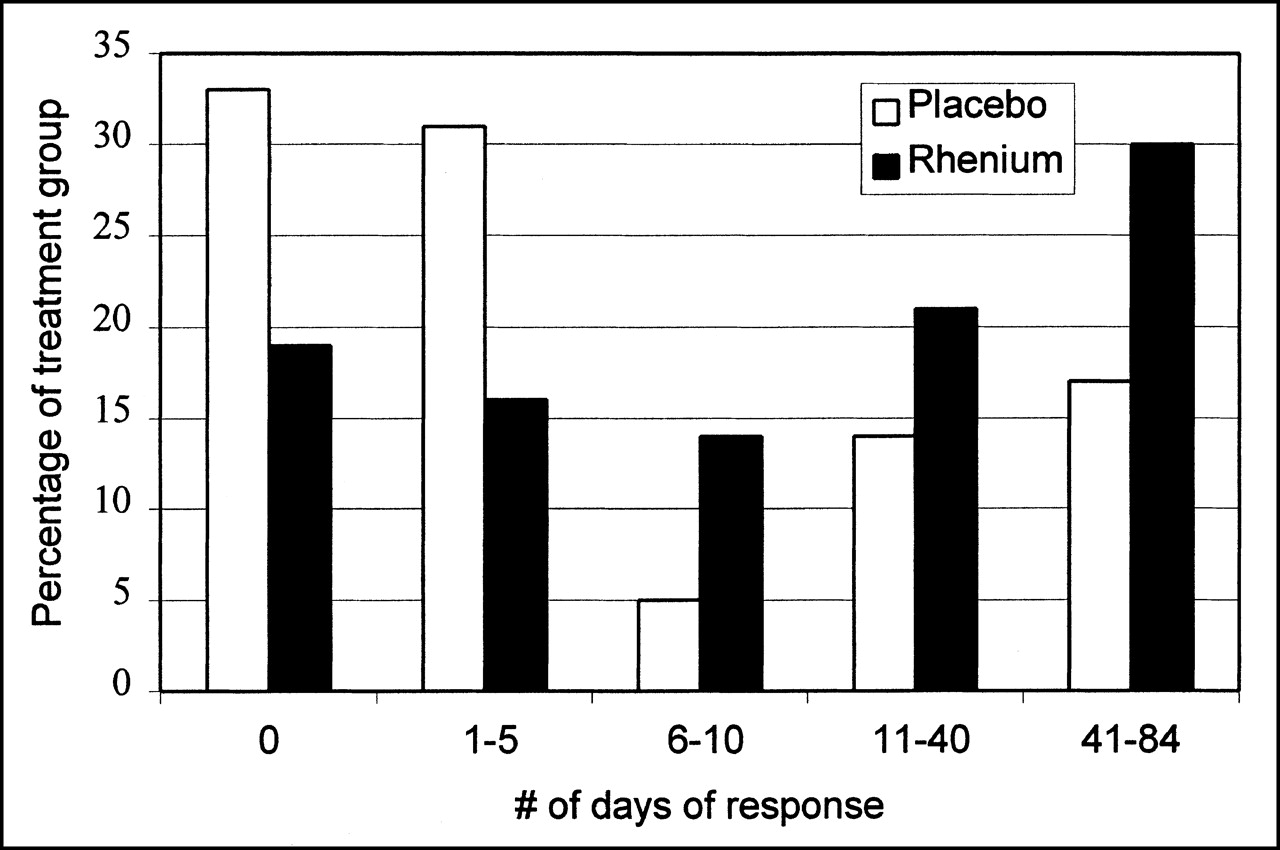
The individual percentage of response days in both patient groups varied from 0% to 96% in the rhenium group and from 0% to 80% in the placebo group. The mean percentage of days of response after 6 and 12 wk of follow-up was significantly greater in the rhenium group (27%, or 23/84 d; 95% confidence interval [CI], 16.6–37.1) than in the placebo group (13%, or 11/84 d; 95% CI, 5.8–20.0; Mann-Whitney test, P < 0.05) (Table 3). The difference in distribution of percentage of response days in the placebo group and the rhenium group allows for another interpretation, shown in Figure 5. Most patients in the placebo group reported fewer than 5 or no response days during the 12-wk follow-up. If the number of patients who reported ≥5 d were grouped and defined as responders, 28 of 43 (65%) responded in the rhenium group, whereas 13 of 36 (36%) responded in the placebo group (relative risk, 1.80; Fisher exact test, P = 0.01).

Distribution of patients in relation to therapy and number of response days.
Fraction of Response Days in Relation to Total Number of Days After Therapy
The mean time to onset of response could not be estimated because the pain scores sometimes fluctuated every day during the entire period in both groups. Therefore, it was impossible to assess the mean duration of response for the same reason. There was a nonsignificant trend toward a lower number of requests for radiotherapy by rhenium-treated patients (relative risk, 1.51; 95% CI, 0.87–2.84; Fisher exact test, P = 0.069). The number of patients who requested radiotherapy was 19 of 43 (44%) in the rhenium group, compared with 24 of 36 (67%) in the placebo group. The interval from treatment until request for radiotherapy was also analyzed with the likelihood ratio; this difference did not reach statistical significance (P = 0.09; hazard ratio, 1.67; 95% CI, 0.91–3.03), although a trend was again observed in favor of the rhenium group (Fig. 6). The curves during the first 3 wk after treatment were similar for both groups, but thereafter the placebo group had more requests for radiotherapy.

Kaplan-Meier curves of treatment groups in relation to time to request for radiotherapy.
The median survival interval was 262 d (95% CI, 232–292) in the placebo group and 213 d (95% CI, 138–288) in the group that received active treatment. The difference in Kaplan-Meier survival curves was not statistically significant.
DISCUSSION
Most clinical studies using 186Re-etidronate to relieve pain from bone metastases have reported response rates of up to 87% (19,21–30). One small, randomized, placebo-controlled study with 186Re-etidronate has been performed thus far, by Maxon et al. (31), and comprised only 13 evaluable patients. Maxon et al. confirmed that the prompt response in approximately 80% of the patients was significantly greater in the rhenium group. Our results also show a significantly better response with 186Re-etidronate, although our study was markedly different in sample size and pain assessment.
The biggest problem is that pain assessment is often subjective and complex because of its multidimensional character. Pain is also never constant, making frequent, perhaps daily, pain assessment mandatory. Most investigators ask their patients retrospectively at predetermined intervals, for example, after 6 and 12 wk, what their pain relief was—a far less reliable method. Our findings for daily pain assessment have confirmed that cancer patients do not have constant pain relief for weeks or even longer, as other investigators have suggested. Therefore, we decided to separately evaluate whether each registered day was a response or nonresponse day according to standardized criteria. The finally reported proportional-response days during the 84-d follow-up cannot be compared with the results from any other publication.
Earlier studies relied heavily on the researcher’s own interpretation of pain relief, with subjective response scores ranging from “slight improvement” to “definitely better.” Effects on pain were evaluated by “patient’s subjective reports at undefined intervals” in a double-blind, placebo-controlled, randomized study of 89Sr therapy of skeletal metastases of prostate carcinoma by Buchali et al. (32). The often-cited Study by the Radiation Therapy Oncology Group used a pain score (0–9) obtained through a subjective semiquantitative assessment of individual verbal response (0 = none to 3 = severe) multiplied by a semiquantitative score for frequency of pain (0 = no pain to 3 = pain most of the time). Although use of analgesic medications was often noted, most investigators did not mention whether alteration in medication index influenced response rate. Tong et al. (33) also assessed a narcotic score in similar ways, but this score was only a secondary response measure. Thus, an increase in pain medication did not influence their final response results. Quilty et al. (34), from the United Kingdom Metastron Investigators’ Group, reported some pain relief in two thirds of 284 patients randomized to either radiotherapy or 89Sr. Unfortunately, pain was assessed at 4-wk intervals only by means of a retrospective interview by the physician.
Thus, to compare different studies, one should use validated, standardized pain assessment methods. These should also include adjustment for major variables such as medication index and daily activities, because of their close correlation with pain and pain reduction. Both our group and Sciuto et al. (30) have used a multidimensional model integrating pain reduction, activities of daily living, and medication index to outline objective criteria for response (19,27, 30,35). Thus, a reduction of pain would not be considered a response if the patient were spending more time in bed.
Another problem is the variety of criteria and methods used to define a responder. Most studies consider a pain reduction of >25%, compared with the baseline value, to be a significant improvement and thus a response. If we had decided that a responder was any patient who reported, for example, >5 d of improved pain index according to our 3-dimensional pain model during the 12-wk follow-up, we could also have concluded that 65% (28/43 patients) were responders in our rhenium group whereas only 36% responders (13/36 patients) were found in the placebo group. These numbers would be well comparable to those reported in the literature.
Our study had some flaws as well. Worsening of the patient’s clinical condition and hospital readmission because of disease progression were 2 reasons that 20 patients did not receive any treatment from this study and may reflect the preterminal stage of some referred patients. Another 32 patients were considered not evaluable because of incomplete baseline or follow-up data. We decided to exclude from analysis these 32 of 111 patients (29%) who had <50% data during the 12-wk follow-up. The study by Maxon et al. (31), a 186Re-etidronate double-blind crossover comparison with placebo, also had 35% nonevaluable patients. Lewington et al. (36), in their randomized placebo-controlled trial with 89Sr, had a similar 34% of patients that were not evaluable. The large Study of the Radiation Therapy Oncology Group, evaluating the efficacy of radiotherapy for palliation of symptomatic osseous metastases, considered 25% of the 1,016 included patients to be nonevaluable (33).
The introduction of an electronic device to collect pain-related data twice daily in this elderly population may have induced the relatively high number of missing data. However, we believe that the use of an electronic pain diary was the most objective and standardized way to measure pain indices at the time of interest. Patients were thus not influenced by the time of evaluation, their physician, or any hospital surrounding. It is well known that such strategies as in-hospital interviews by the investigative physician concerning the outcome of a drug or treatment may influence the study results. In our study, retrograde registration of pain indices that the patient himself had forgotten was prohibited by the electronic pain diary. This feature eliminated any retrograde data manipulation and allowed online data registration, in contrast to posttherapy evaluation by the physician at predetermined intervals. The use of an electronic pain diary has been validated by de Wit et al. (37), who concluded that it is a feasible tool for cancer patients to assess and document chronic pain at home.
Comparison of studies using 186Re-etidronate and studies using other radiopharmaceuticals remains difficult, if not impossible, because of methodologic impairment and the various pain assessment methods available thus far. However, 2 comparative studies with 186Re-etidronate, 188Re-etidronate, and 89Sr have been published recently. Theoretically, the shorter physical half-life (16.9 h) of 188Re-etidronate compares favorably with 186Re-etidronate and 89Sr, but clinical reports on therapeutic effects are limited (38). Neither of the 2 reported studies (39,40) showed any difference in efficacy and toxicity, either in the initial treatment or in retreatment.
CONCLUSION
The Placorhen study on 186Re-etidronate for the treatment of painful bone metastases from prostate cancer showed that efficacy was significantly better in the treated group than in the placebo group. This result was achieved using an electronic pain diary, strict pain assessment, and objective pain response criteria based on a multidimensional pain model.
Acknowledgments
The authors thank Ruth van Wijngaart and Freekje Bar for their secretarial assistance and data management and Jan de Groot for the illustrations. This investigation was supported by Mallinckrodt Medical BV.
Footnotes
Received Sep. 12, 2001; revision accepted Apr. 25, 2002.
For correspondence or reprints contact: Shiuw H. Han, MD, PhD, Department of Nuclear Medicine, Albert Schweitzer Hospital, Albert Schweitzerplaats 25, 3318 AT Dordrecht, The Netherlands.
E-mail: shiuw.han{at}planet.nl
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Treatment with bone-seeking radionuclides for painful bone metastases in patients with lung cancer: a systematic review
- Palliation and Survival After Repeated 188Re-HEDP Therapy of Hormone-Refractory Bone Metastases of Prostate Cancer: A Retrospective Analysis
- High-Linear Energy Transfer Irradiation Targeted to Skeletal Metastases by the {alpha}-Emitter 223Ra: Adjuvant or Alternative to Conventional Modalities?
- Therapy Tolerance in Selected Patients With Androgen-Independent Prostate Cancer Following Strontium-89 Combined With Chemotherapy
- Bone-Seeking Radionuclides For Therapy