


Abstract
This retrospective study compared the effects of single and multiple administrations of 186Re-hydroxyethylidenediphosphonate (186Re-HEDP) on palliation and survival of prostate cancer patients presenting with more than 5 skeletal metastases. Methods: A total of 60 patients were divided into 3 groups. Group A (n = 19) consisted of patients who had received a single injection; group B (n = 19), patients who had 2 injections; and group C (n = 22), patients who had 3 or more successive injections. The 188Re-HEDP was prepared using non–carrier-added 188Re obtained from an in-house 188W/188Re generator after dilution with carrier perrhenate. Patients’ data available from the referring physicians—including prostate-specific antigen levels—were entered into a Windows-based matrix and analyzed using a statistical program. The Gleason scores were similar for all 3 groups. Results: Mean survival from the start of treatment was 4.50 ± 0.81 mo (95% confidence interval [CI], 2.92–6.08) for group A, 9.98 ± 2.21 mo (95% CI, 5.65–14.31) for group B, and 15.66 ± 3.23 (95% CI, 9.33–22.0) for group C. Although the 3 groups did not differ in Gleason score, the number of lost life-years was significantly lower in group C than in groups A and B. Pain palliation was achieved in 89.5% of group A, 94.7% of group B, and 90.9% of group C. Conclusion: Posttreatment overall survival could be improved from 4.50 to 15.66 mo by multiple-injection bone-targeted therapy with 188Re-HEDP, when compared with a single injection. Significant pain palliation was common and independent of administration frequency.
Bone metastases are frequent and encountered by all physicians treating oncologic patients (1). About 50% of prostate cancer patients will develop bone metastases, which are predominantly osteoblastic. The osteolytic type has the tendency to develop fractures resulting in serious morbidity. Chronic pain syndrome is the most important complication of bone metastases and has a negative impact on quality of life. Many of these patients are candidates for radionuclide therapy, since as many as 50% of patients are reported to receive only inadequate pain treatment by alternative methods (2).
Radionuclide therapy of bone metastases was first used decades ago by administration of 32P (3), which is incorporated in the DNA of rapidly proliferating bone marrow cells as well as in the trabecular and cortical bone structures. A relatively low 1:2 ratio of normal bone to metastatic tissue has been estimated (4). More recently, a variety of β-emitting radioisotopes has been investigated for therapy of bone metastases. The maximal β-energy of these radioisotopes is in the range of 0.8–2.3 MeV, with an average β-energy between 0.27 and 0.8 MeV (Table 1). 89Sr-chloride and ionic 90Y are both calcium analogs that are sequestered as cations by bone in relation to the intensity of osseous metabolism (5–9). 89Sr is excreted renally to 70%–90% and is eliminated from the vascular compartment within the first few hours (10). Except for bone uptake and excretion via the urinary system, there is no accumulation in any organ system. Accumulation of 89Sr in metastatic lesions is 5–20 times higher than accumulation in normal bone tissue. In one study, 90 d after administration, 20%–88% of the injected 89Sr activity was found around metastatic bone lesions (8). The effective half-life was calculated to be over 50 d, and thus 89Sr delivers low-dose-rate radiation.
Comparison of Bone-Seeking Radiopharmaceuticals
A different radiopharmaceutical option is to chemically attach radionuclides to phosphonate carrier molecules that are known to have a high osteoaffinity. Among these radiopharmaceuticals are, for example, 153Sm-ethylenediaminetetramethylenephosphonate (EDTMP) and 186Re-hydroxyethylidenediphosphonate (HEDP) (11,12). Like the above-mentioned radionuclides, these agents are also excreted mainly by the kidneys, and they disappear rapidly from the vascular compartment (13,14). Twelve hours after administration, 50% of the administered activity of 186Re-HEDP and 153Sm-EDTMP is eliminated renally. Uptake in the skeleton is between 20% and 30% of the injected dose for 186Re-HEDP and between 30% and 50% for 153Sm-EDTMP. Accumulation in metastatic lesions is between 3 and 20 times as high as in normal bone, and the effective half-lives of 188Re-HEDP and 153Sm-EDTMP are between 2 and 3 d. 188Re-HEDP has been used for pain palliation in patients with prostate cancer and bone metastases since the early 1990s (15,16). Retrospective results with 186Re-HEDP were published by Schoeneich et al. in 1997 (17).
188Re (half-life, 16.9 h) is a more attractive candidate than 186Re since it can be obtained in no-carrier-added form from a 188W/188Re generator and has a long useful shelf-life of several months. In 2003, Palmedo et al. published results obtained from a randomized phase II trial with 188Re-HEDP in patients with hormone-refractory prostate carcinoma (18) designed to compare the efficacy of multiple successive injections with that of a single administration of this agent. The effectiveness of 188Re-HEDP for pain palliation was better in the repeated-treatment group, with a response rate and time of response of 92% and 5.66 mo, respectively. In addition, 39% of patients with repeated treatments exhibited a decrease in prostate-specific antigen levels of more than 50% for at least 8 wk. These results were interpreted to indicate that repeated 188Re-HEDP therapy is beneficial in patients with prostate cancer and bone metastases (18).
The goal of the present study was to perform a retrospective follow-up analysis of the palliative and survival effects of single versus multiple successive administrations of 188Re-HEDP to prostate cancer patients presenting with multiple skeletal metastases.
MATERIALS AND METHODS
Patients
This retrospective study included 60 hormone-refractory patients. Group A comprised patients who had received only 1 therapy (n = 19); group B, patients who had received 2 therapies (n = 19); and group C, patients who had received 3 or more therapies (n = 22). All patients had bone pain and presented with more than 5 lesions documented by a bone scan. Because 188Re is not commercially available as an approved radiopharmaceutical, informed consent was required and the agent was ordered and compounded by a radiopharmacist (in-house production). We provided the referring physicians with a questionnaire asking if the patient was alive or deceased, and if deceased, whether the death was attributed to prostate carcinoma or other causes. Additionally, the questionnaire asked for the survival time after the last 188Re-HEDP therapy (and if the pain had decreased), the prostate-specific antigen (PSA) level, and the referring physician's objective impression about pain palliation.
Radiopharmaceutical Production
188Re-HEDP was prepared according to the method of Palmedo et al. (15), Knapp et al. (19), and Guhlke et al. (20). Especially important in the formulation of 188Re-HEDP is the use of carrier perrhenate, since the 188Re is obtained essentially carrier-free from a generator system by β-decay of 188W.
In contrast to 188Re is 186Re, which is produced in nuclear reactors through neutron capture of stable 185Re and thus by virtue of its mode of production is carrier-added. The presence of macroscopic amounts of stable rhenium in rhenium-HEDP preparations is decisive with respect to the form of the phosphonate chemical species (15). In carrier-added preparations, these species consist of rhenium–rhenium bonds that cannot be formed using carrier-free 188Re. As a consequence, the biodistribution and intravenous stability of carrier-added and no-carrier-added 188Re-HEDP show remarkable differences, and only the carrier-added composition accumulates to a high percentage in bone (20).
188Re was obtained from an 18.5-GBq (500-mCi) alumina-based 188W/188Re generator fabricated at the Oak Ridge National Laboratory, using 188W produced in the High Flux Isotope Reactor. Depending on the specific volume of activity required, the generator eluates (typically 20 mL of physiologic saline) were concentrated to a volume of 1.5 mL of physiologic saline using a convenient and useful online concentration method that has been reported elsewhere (19,20). For preparation of the 188Re-HEDP, 15 μL of a stable ammonium-perrhenate solution (26 mg of NH4ReO4/mL) in physiologic saline were added to the concentrated 188Re solution. This carrier-added 188Re-perrhenate solution was used for the labeling reaction by being added through a 0.22-μm sterile filter to a kit vial containing 8.3 mg of HEDP, 3.0 mg of gentisic acid, and 3.9 mg of stannous chloride dehydrate. The vials were then heated for 20 min at 90°–100°C and cooled to room temperature. For neutralization, 1.5 mL of a sterile solution of 39 mg of sodium acetate trihydrate were added, yielding a final pH of 4.5–5.5. Quality control of carrier-added 188Re-HEDP was performed using instant thin-layer chromatography silica gel strips (15).
According to a dose escalation study published earlier by Palmedo et al. in 2000 (15), a dose of 2,960–3,330 MBq (80–90 mCi) of 188Re-HEDP was administered to each patient. The interval between successive administrations of 188Re-HEDP was approximately 8 wk, and up to a maximum of 8 successive therapies per patient were applied.
Data Analysis
The data from patient records and the questionnaire were entered into a Windows Excel (Microsoft) data matrix and were then transferred and evaluated using the SPSS statistics program (version 16.0; IBM). The parameters that were evaluated included the absolute (n) and relative (%) frequency. In addition, the mean, SEM, median, minimum, and maximum values were calculated. Because a goal of this study was to compare the 3 therapy groups, nominal and ordinal figures were used to calculate nonparametric tests, using the χ2 test and the Kruskal–Wallis test. Survival was analyzed according to the Kaplan–Meier procedure and log-rank test, with the significance set to a value of P less than 0.05.
RESULTS
The 3 patient groups were similar in mean and median age (Table 2). Table 2 summarizes the Gleason score data for the 3 groups. At the time of diagnosis, the Gleason scores were comparable, and by evaluation of the prognostic factor according to Helpap, no differences were found. Table 2 also shows the mean age of the patients at the time of the first 188Re-HEDP therapy. The time span between diagnosis of prostate cancer and first therapy ranged from 5.7 y (group C) to 6 y (group B) to 7.5 y (group A) (Table 3), and this difference was not significant.
Patient Data
Results of 188Re-HEDP Therapy
Table 3 summarizes the pain palliation results; no significant differences between the 3 groups were observed.
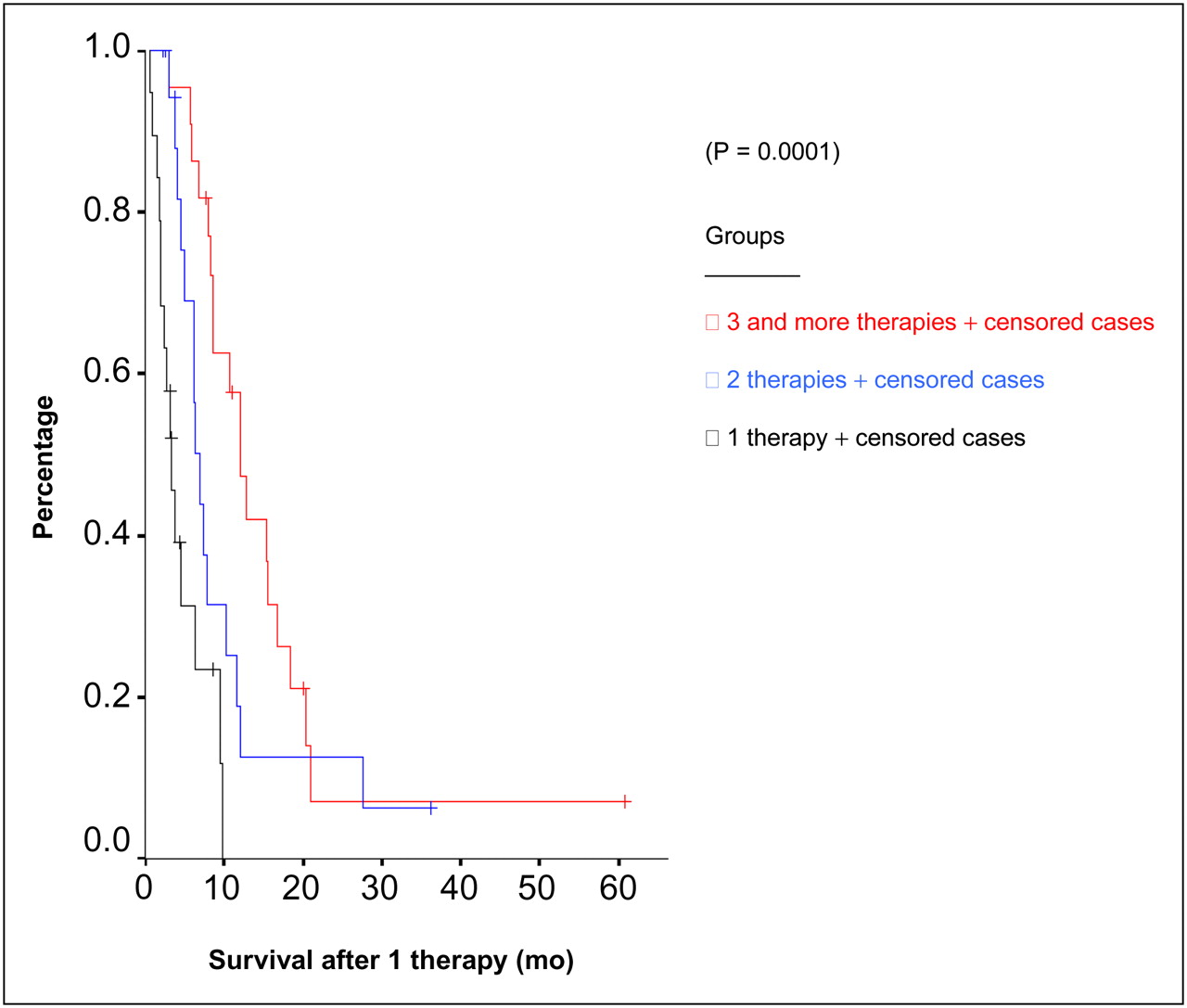
In contrast to Palmedo et al. (18), we did not observe any significant differences with respect to the course of PSA (Table 3). Table 4 presents the data on age at death and number of lost life-years, which was significantly lower in group C than in Groups A and B. Table 5 shows the survival results after diagnosis of prostate cancer. Mean survival after the initial therapy improved from 4.5 mo in group A to 9.98 mo in group B and 15.7 mo in group C. The results of survival after the initial rhenium therapy are also presented in Figure 1. As has already been described by Palmedo et al. (15), only reversible grade 2 thrombopenia and reversible grade 1 leukopenia were observed.
Age at Death and Lost Years of Life
Survival Data
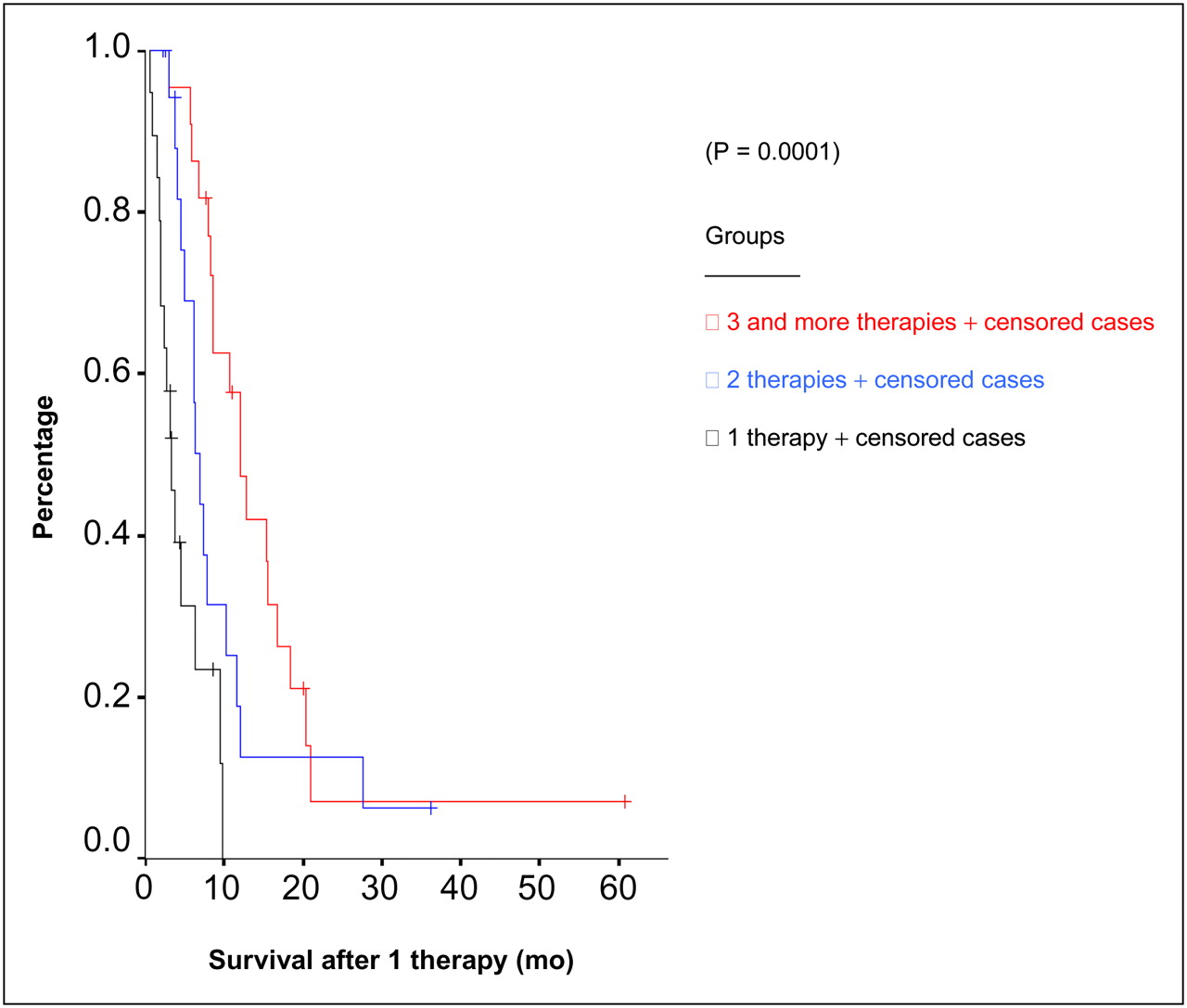
Survival of the 3 groups after first rhenium therapy (mo). Statistics are from Table 5.
DISCUSSION
In a comprehensive review of systemic metabolic radiopharmaceutical therapy in the treatment of metastatic bone pain, Paes and Serafini (21) have summarized the available literature data on various bone-seeking radiopharmaceuticals labeled with different therapeutic isotopes. For 89Sr-chloride, a response usually occurs within 6 wk, with a mean duration of 6 mo (22). A painful flair response is often seen in approximately 10%–20% of patients treated with 89Sr, and these patients experience better pain relief (23). A report by Finlay et al. (25) showed that 8%–77% of patient had a complete response to 89Sr. In general, 44% of patients had some degree of response to 89Sr treatment.
153Sm-lexidronam (153Sm-EDTMP [Quadramet]; EUSA Pharma) has increasingly been used during the last decade. In general, 153Sm provides effective palliation in 83.8% of patients with painful bone metastases (25).
186Re-HEDP, although initially developed at the University of Cincinnati, is not available in the United States for clinical use. This pharmaceutical was also withdrawn from the European market in 2010. Maxon et al. (27) concluded that pain improved significantly in 77% of patients after the initial injection. The PLACORHEN (Placebo-Controlled Rhenium) study (28) included 111 patients initially, and 79 were evaluated (43 treated, 36 placebo). The total response of patients treated with 186Re-HEDP varied from 0% to 96% (mean, 27%), and in the placebo group, the total response varied from 0% to 80% (mean, 13%). The number of patients requesting radiotherapy was higher in the placebo group (67%) than in the 186Re group (44%). Other studies (28,29) found response rates of 80% and 92%, respectively. The duration of pain relief ranged from 3 wk to 12 mo.
In a study by Lam et al. (31), 188Re-HEDP was combined with gemcitabine in hormone-refractory prostate cancer patients with bone metastases, in a phase 1 safety and toxicity study. It was concluded that capecitabine may safely be used in combination with 188Re-HEDP, in a dose of 2,500 mg/m2 per day and 37 mg/kg, respectively. The same investigators combined zoledronic acid and 153Sm-EDTMP in hormone-refractory prostate cancer patients and concluded that zoledronic acid treatment does not influence the uptake of the respective radiopharmaceutical (32). These and other studies reflect possible benefits of such combined therapeutic strategies.
The potential of long-term pain relief and possible therapeutic effects from these bone-seeking therapeutic radiopharmaceuticals is important. A group led by Sartor (23) reported the efficacy of repeated doses of 153Sm-EDTMP patients with metastatic bone pain. The pain scores and side effects were analyzed in 55 patients receiving 2 or more doses. Decreases in pain scores were observed in 70%, 63%, and 80% of patients at 4 wk after the first, second, and third administrations, respectively. Only minor decreases in platelet and white blood cell counts were seen, with a nadir at week 4 and recovery in 90% of patients by week 8. These data prove that repeated treatment with 153Sm-EDTMP is both safe and effective in patients with metastatic bone disease (33).
Maxon et al. (27) performed an open-label trial using a single intravenous administration of approximately 1,258 MB1 (34 mCi) of 186Re-HEDP. After the second treatment, 50% of patients showed an improvement in pain. After up to 5 treatments, a complete resolution of pain was found. Clinically unimportant decreases in white blood cell and platelet counts were observed, but no other toxicity was apparent.
Palmedo et al. (18) found that compared with single-injection therapy, repeated bone-targeted therapy with 188Re-HEDP administered to patients with advanced progressive hormone-refractory prostate carcinoma enhanced pain palliation and improved progression-free and overall survival. In the current study with 188Re-HEDP, we extended our data by adding a group of patients receiving 3 or more successive therapies. According to age and Gleason score, patients in the multiple-therapy group did not differ from those patients undergoing only 1 or 2 therapies. Mean survival after the first therapy could be improved from 4.50 to 9.98 mo and up to 15.66 mo. The data from groups A and B are comparable to the previously published results by Palmedo et al. (18), with median overall survival after 1 therapy of 7.0 mo, which could be extended to 12.7 mo after 2 therapies. Our study showed that the mean survival could be extended to up to 15.66 mo using 3 or more therapies. However, no significance was found in mean and median survival after diagnosis of the prostate cancer. Unexpectedly, group A showed the longest overall survival, compared with the other 2 groups. Although the 3 groups did not differ in Gleason score, at least at the time of the diagnosis of prostate cancer, no differences for the other 2 groups were found. In contradiction to this, the number of lost life-years was significantly lower in group C (3 or more therapies) than in groups A and B. One other explanation would be that patients with a better prognosis would survive long enough to undergo repeated treatment. The only possibility of evaluating this observation would be in a study in which all patients with painful bone metastases have the initial 188Re-HEDP treatment at the same time, as is of course not possible because of ethical considerations. Thus, large randomized and prospective studies would be needed to clearly define the benefits of repeated radionuclide therapy with 188Re.
We did not observe an antitumor effect (PSA) to the extent observed by Palmedo et al. (18), probably because all patients in their series had a fixed follow-up. In our patients, PSA had been determined only at relatively long intervals. Therefore, in our patients with longer survival, the PSA decreases were not as pronounced as in patients who had regular follow-up, including PSA determinations, for at least 3 mo. Because 188Re-HEDP is not commercially available, in-house production is required, which is cost-effective because of the multiple-month useful shelf-life of the 188W/188Re generator system. But even without clarification of the situation with respect to survival, patients receiving 188Re-HEDP treatment will benefit from bone pain palliation. The group of patients treated had therapy-refractory bone metastases for which no other treatment modality is available.
CONCLUSION
Compared with single-injection bone-targeted therapy, repeated bone-targeted treatment with 188Re-HEDP improved posttreatment overall survival from 4.50 to 15.66 mo in patients with progressive hormone-refractory prostate cancer. Significant pain palliation was achieved in about 90% of the study cohort. With respect to the unpredictable course of the disease, randomized, prospective studies are needed to achieve a comparable data basis in these patients and to define the benefits of repeated therapy.
DISCLOSURE STATEMENT
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
This study was in part supported by the Alexander von Humboldt Foundation, and one of the authors is a former von Humboldt fellow. Research at the Oak Ridge National Laboratory (ORNL) is supported by the U.S. Department of Energy (DOE) under contract DE-AC05-00OR22725 with UT-Battelle, LLC. No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Oct. 5, 2011.
- © 2011 by Society of Nuclear Medicine
REFERENCES
- Received for publication May 23, 2011.
- Accepted for publication August 17, 2011.





{kind=link}