


Abstract
99mTc-Tetrofosmin is a recently introduced radioactive isotope for the assessment of myocardial perfusion. Data regarding the prognostic value of stress imaging using this isotope are scarce. The aim of this study was to assess the prognostic value of dobutamine-atropine 99mTc-tetrofosmin SPECT for the prediction of late cardiac events in patients with known or suspected coronary artery disease. Methods: A total of 721 consecutive patients with limited exercise capacity underwent dobutamine-atropine stress 99mTc-tetrofosmin SPECT. Follow-up was successful in 719 of 721 patients (99.7%). Twenty-eight patients who underwent early revascularization were excluded. Results: Myocardial perfusion abnormalities were detected in 381 patients (55%) and included fixed defects in 190 patients (27%) and reversible defects 191 patients (28%). During a mean follow-up period of 37 ± 17 mo, there were 150 deaths (22%), of which 62 (41%) were attributed to cardiac causes. Nonfatal myocardial infarction occurred in 23 patients (3%), and late (>3 mo) coronary revascularization was performed on 21 patients (3%). The cardiac death rate was 1%/y in patients with a normal scan and 5.1%/y in patients with an abnormal scan (P < 0.0001). In a multivariable Cox proportional-hazards model, the presence of abnormal perfusion was independently associated with an increased risk of cardiac death, after adjusting for clinical and stress test data (hazard ratio, 8.2; 95% confidence interval, 3.2–21). Conclusion: Dobutamine-atropine stress 99mTc-tetrofosmin SPECT is a useful imaging method for distinguishing patients at high and low risk of future cardiac events. The presence of perfusion abnormalities provides incremental prognostic information to clinical, stress electrocardiographic, and hemodynamic data.
Pharmacologic stress myocardial perfusion imaging is a useful alternative to exercise stress in patients with limited exercise capacity (1–3). For many years, 201Tl was the most widely used radioactive isotope in conjunction with pharmacologic stress testing for the diagnosis and risk stratification of coronary artery disease (CAD) (1). The use of 99mTc-labeled agents provides the advantages of improved image quality, increased consistency of image analysis, and a larger injectable dose because of a shorter half-life compared with 201Tl (2–4). 99mTc-Labeled agents (sestamibi and tetrofosmin) share similar pharmacokinetic properties. These radiopharmaceuticals are distributed within the myocardium in proportion to the regional cardiac blood flow. After intravenous injection, a relatively rapid clearance of the tracer from the blood and extracardiac structures occurs with minimal redistribution from the myocardium. Although several studies have revealed the diagnostic value of 99mTc-tetrofosmin SPECT (5–11), the data to define the prognostic value of stress imaging with 99mTc-tetrofosmin are limited. In a recent study (12), the extent of reversible perfusion abnormalities during dipyridamole infusion was lower with tetrofosmin than with sestamibi. It was concluded that the data relating to the prognostic value of 99mTc-sestamibi in the literature should not be empirically extrapolated to 99mTc-tetrofosmin imaging because of these differences. In addition, few studies have shown a reduced sensitivity of tetrofosmin imaging in patients with intermediate stenotic lesions due to a low extraction fraction and early plateau phase (13). These findings may have important prognostic implications in patients with normal tetrofosmin perfusion studies. In these cases CAD may be missed. Recent studies have shown that hyperemia induced by a dobutamine-atropine stress test is of a magnitude at least equal to hyperemia induced by vasodilator stress agents such as dipyridamole (14). The aim of this study was to assess the prognostic value of dobutamine-atropine 99mTc-tetrofosmin SPECT in patients with known or suspected CAD.
MATERIALS AND METHODS
Patient Selection
Between 1994 and 2000, 721 consecutive patients with limited exercise capacity were referred for dobutamine-atropine stress 99mTc-tetrofosmin SPECT for evaluation of suspected or known CAD. Follow-up was successful in 719 of 721 patients (99.7%). Twenty-eight patients who underwent coronary revascularization within 3 mo of scintigraphy were excluded from analysis. In these patients, the decision to revascularize may be influenced by test results. Consequently, the prognostic data reported are based on 693 patients. All patients gave informed consent before testing. The Hospital Ethics Committee approved the protocol.
Clinical Data
Before the dobutamine stress test, a structured interview and clinical history, including assessment of cardiac risk factors, were obtained. Hypertension was defined as a blood pressure of ≥140/90 mm Hg or treatment with antihypertensive medication. Diabetes mellitus was defined as a fasting glucose level of ≥7.8 mmol/L or the need for insulin or oral hypoglycemic agents. Hypercholesterolemia was defined as a total cholesterol of ≥6.4 mmol/L or treatment with lipid-lowering medication.
Dobutamine Stress Test
The dobutamine-atropine stress test was performed as described (7). Dobutamine was administered intravenously, starting at a dose of 5 μg/kg/min for 3 min, then 10 μg/kg/min for 3 min, increasing by 10 μg/kg/min every 3 min up to a maximum dose of 40 μg/kg/min. If the test endpoint was not reached at a dobutamine dose of 40 μg/kg/min, atropine (up to 2 mg) was given intravenously. Blood pressure, heart rate, and electrocardiography were monitored continuously. Test endpoints were achievement of target heart rate (85% of maximum age-predicted heart rate), horizontal or downsloping ST-segment depression of >2 mm, ST-segment elevation of >1 mm in patients without previous myocardial infarction, severe angina, systolic blood pressure fall of >40 mm Hg, blood pressure of >240/120 mm Hg, or significant arrhythmia. Metoprolol was available to reverse the (side) effects of dobutamine or atropine if these did not revert spontaneously after termination of dobutamine infusion.
SPECT
Approximately 1 min before the termination of the stress test, an intravenous dose of 370 MBq 99mTc-tetrofosmin was administered. For resting studies, 370 MBq tetrofosmin were injected at least 24 h after the stress study. Image acquisition was performed with a triple-head gamma-camera system (Prism 3000 XP; Picker International, Cleveland, OH). For each study, 6 oblique (short axis) slices from the apex to the base and 3 sagittal (vertical long axis) slices were defined. Each of the 6 short-axis slices was divided into 8 equal segments. The septal part of the 2 basal slices was excluded from analysis because this region corresponds to the fibrous portion of the interventricular septum and normally exhibits reduced uptake. Therefore, 47 segments were identified (3 long axis and 44 short axis). The interpretation of the scan was performed semiquantitatively by visual analysis assisted by analysis of the circumferential profiles. Stress and rest tomographic views were reviewed side by side by an experienced observer who was unaware of each patient’s clinical data. A reversible perfusion defect was defined as a perfusion defect on stress images that partially or completely resolved at rest in ≥2 contiguous segments or slices in the 47-segment model. A fixed perfusion defect was defined as a perfusion defect on stress images in ≥2 contiguous segments or slices, which persists on rest images in the 47-segment model. An abnormal study was considered in the presence of a fixed or reversible perfusion defect (or both). To assess the severity of perfusion abnormalities, the left ventricular myocardium was divided into 6 segments: anterior, inferior, septal anterior, septal posterior, posterolateral, and apical. Each of the 6 major left ventricular segments was scored using a 4-grade scoring method (0 = normal, 1 = slightly reduced, 2 = moderately reduced, 3 = severely reduced or absent uptake). The perfusion defect score was derived by the summation of the score of the 6-myocardial segments at stress (SSS) and at rest (SRS). The difference was expressed as the summed difference score (SDS).
Patient Follow-Up
Follow-up data were obtained in 2000. The mean follow-up period was 37 ± 17 mo. The present status was determined by contacting the patient’s general practitioner or by review of hospital records. The date of the last review or consultation was used to calculate the follow-up time. Outcome events were overall death, cardiac death, nonfatal myocardial infarction, and late (>3 mo) coronary revascularization. Cardiac death was defined as death caused by acute myocardial infarction, significant cardiac arrhythmias, or refractory congestive heart failure. Sudden death occurring without another explanation was included as cardiac death. Nonfatal myocardial infarction was defined by cardiac enzyme levels and electrocardiographic changes.
Statistical Analysis
Data were expressed as mean value ± SD or number and compared using the Student t test or χ2 test. Univariate and multivariate Cox proportional-hazards regression models were used to identify independent predictors of late cardiac events. Variables were selected in a stepwise forward selection manner with entry and retention set at a significance level of 0.05. The risk of a variable was expressed as a hazard ratio with a corresponding 95% confidence interval. The incremental value of myocardial perfusion scintigraphy over the clinical variables in the prediction of events was performed according to 2 models. In model 1, the only scan variable entered was the presence of an abnormal scan. In model 2, the presence of a fixed defect or reversible defect was included separately. The probability of survival was calculated using the Kaplan-Meier method, and survival curves were compared using the log-rank test. P < 0.05 was considered statistically significant.
RESULTS
Demographics and Stress Test Results
Clinical characteristics are presented in Table 1. During the dobutamine-atropine stress test, there was a significant increase of heart rate (from 77 ± 17 to 133 ± 17 beats per minute; P < 0.0001) and systolic blood pressure (from 144 ± 23 to 155 ± 32 mm Hg; P < 0.0001). The highest dobutamine dose was 10 μg/kg/min in 1% of the patients, 20 μg/kg/min in 16%, 30 μg/kg/min in 17%, and 40 μg/kg/min in 66%. Atropine was added in testing 258 patients (37%); it was administered more frequently in testing patients who received β-blocker therapy (150/253 [59%]) than in patients who did not (108/440 [25%]; P < 0.001). The test was inconclusive (failure to achieve the target heart rate in the absence of perfusion abnormalities) in 7% of the patients. The cardiac event rate in patients who did not achieve the target heart rate did not differ from the event rate in patients with a complete test (P = 0.48). No relationship was found between the achieved final stage of dobutamine infusion and subsequent cardiac death or infarction.
Baseline Characteristics
Side effects during dobutamine-atropine stress were short ventricular tachycardia (<10 complexes) in 23 patients (3.3%), atrial fibrillation in 7 patients (1.0%), severe hypotension (decrease in systolic blood pressure of >40 mm Hg) in 7 patients (1.0%), and severe hypertension (blood pressure of >240/130 mm Hg) in 5 patients (0.7%). Minor side effects were chills in 52 patients (7.5%), headache in 46 patients (6.6%), and nausea in 38 patients (5.5%). No patient experienced a myocardial infarction or ventricular fibrillation.
SPECT and Follow-Up Results
Myocardial perfusion abnormalities were present in 381 of the 693 patients (55%) and included fixed defects alone in 190 patients (27%) and reversible defects in 191 patients (28%). These defects were completely reversible in 61 patients (9%) and partially reversible in 130 patients (19%). There were 150 deaths (22%) during follow-up, of which 62 were attributed to cardiac causes. Nonfatal myocardial infarction occurred in 23 patients (3%), and late coronary revascularization (>3 mo) was performed on 21 patients (3%).
Univariate Analysis
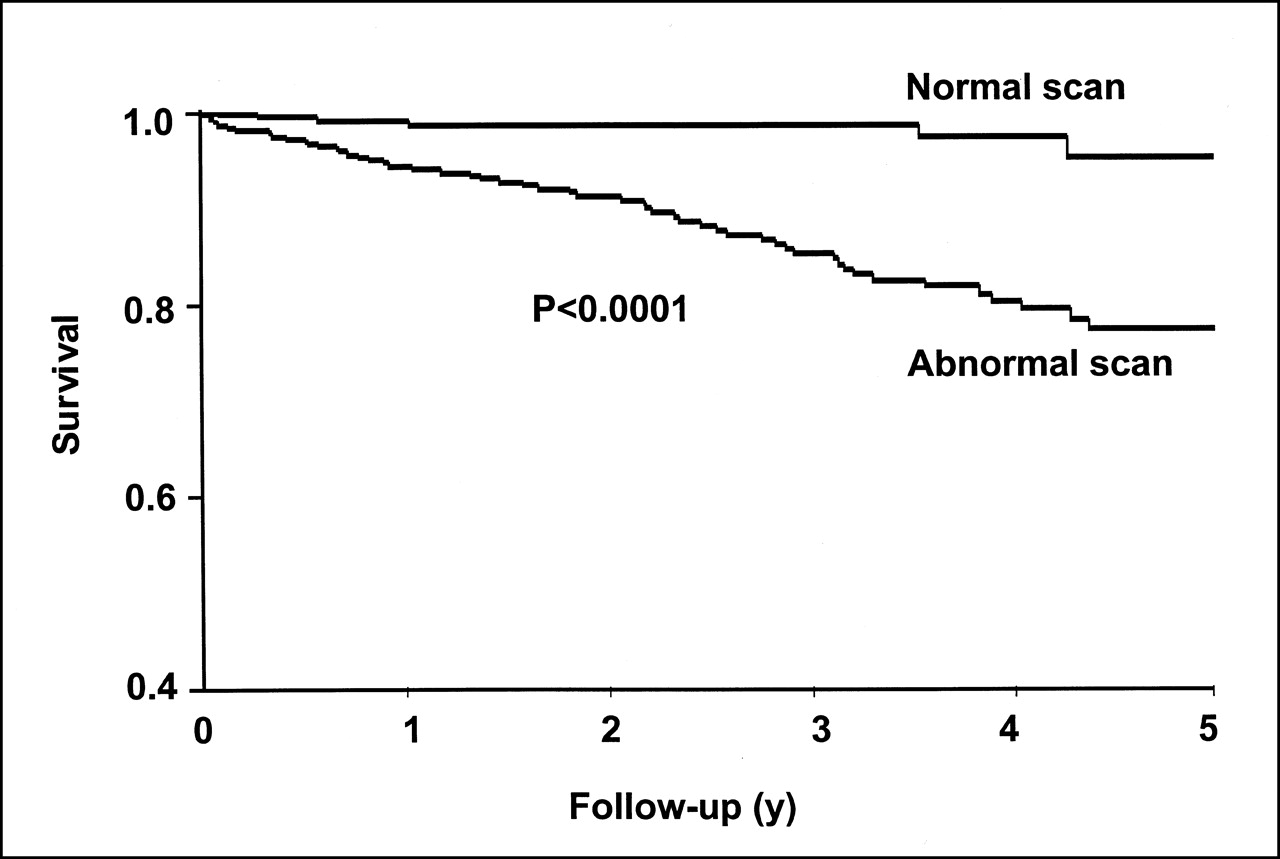
The cardiac death rate (adjusted for number of patients at risk) was 1%/y in patients with normal scans versus 5.1%/y in patients with abnormal scans during the 5-y follow-up period (P < 0.0001) (Fig. 1). Patients with a normal 99mTc-tetrofosmin SPECT scan had a hard-event rate (cardiac death or myocardial infarction) of 1.5%/y compared with 5.5%/y in those with abnormal scans (P < 0.0001). Univariate predictors of endpoints of interest are shown in Table 2. The most powerful predictor for cardiac death, cardiac death or (re)infarction, coronary revascularization, and all events was abnormal perfusion. Moreover, the extent and severity of the defect (expressed by the SSS, SRS, and SDS) were related to cardiac death or nonfatal myocardial infarction.

Kaplan-Meier curves for cardiac death during follow-up in patients with normal and abnormal 99mTc-tetrofosmin SPECT scans.
Univariate Predictors of Late Cardiac Events
Multivariate Analysis
A stepwise logistic regression model showed that an abnormal scan was the strongest independent predictor of cardiac death. Multivariate predictors of cardiac death are presented in Table 3. The addition of the perfusion parameters to the clinical variables was performed according to 2 models. In the first model (Table 3, model 1) the presence of an abnormal scan was added to the clinical characteristics, stress electrocardiographic data, and hemodynamic data. In model 2 the presence of a fixed or reversible perfusion defect was added separately. The presence of an abnormal scan (model 1) provided incremental prognostic value over clinical, stress electrocardiographic, and hemodynamic data (log-likelihood, −324 to −305; P < 0.0001). Model 2 also offered incremental prognostic information compared with the clinical, stress electrocardiographic, and hemodynamic parameters (log-likelihood, −324 to −313; P < 0.0001).
Multivariate Predictors of Cardiac Death
DISCUSSION
99mTc-Tetrofosmin is currently used in many nuclear laboratories in the United States and in Europe. Because of considerations of sensitivity in moderately stenotic lesions and the possibility of underestimating perfusion abnormalities, studies of the prognostic information obtained by imaging with this tracer are important to clarify—whether the physician can rely on the results of the test in planning further management of patients—particularly in deferring further diagnostic evaluation or interventions in patients with a negative study.
To our knowledge, this is the first study to assess the prognostic value of dobutamine 99mTc-tetrofosmin imaging. This study showed that dobutamine-atropine 99mTc-tetrofosmin SPECT provided incremental prognostic value over clinical data, for distinguishing patients with high and low risk of future cardiac events. A normal perfusion scan was related to a good prognosis and identified the patient subset at low risk for cardiac death (cardiac death rate, 1%/y). This event rate is comparable with that in the general population (15). Conversely, the cardiac death rate was 5.1%/y in patients with abnormal scan results (P < 0.0001).
The most important predictor of late cardiac events was an abnormal perfusion scan, which increased the risk for cardiac death by 8-fold. Fixed and reversible perfusion abnormalities provided incremental independent prognostic information. Survival curves continued to diverge over time, indicating that the prognostic value of 99mTc-tetrofosmin SPECT was maintained during the entire follow-up period.
In contrast to the limited experience with prognostic applications of 99mTc-tetrofosmin myocardial perfusion imaging, multiple studies (16–21) have reported the prognostic value of imaging with 99mTc-sestamibi, the perfusion agent that was introduced earlier. Most of these studies, with patient populations that were comparable with our study, showed that normal perfusion scintigraphy was related to a very low probability of future cardiac events. Nevertheless, most of these studies showed that the event rate was relatively higher in patients with normal pharmacologic stress compared with normal exercise stress perfusion imaging, probably attributed to the referral of patients with a higher risk status to pharmacologic stress testing (22). Stratmann et al. (16) reported the prognostic value of exercise 99mTc-sestamibi SPECT in 521 patients with a median follow-up period of 13 mo. Patients with normal sestamibi images had a hard-event rate (cardiac death or myocardial infarction) of 0.5%/y compared with 7%/y for those with abnormal sestamibi scans. Heller et al. (17) reported hard-event rates of 1.4% and 7.4% during a 12.8-mo follow-up period for subjects with normal and abnormal dipyridamole 99mTc-sestamibi scintigraphy, respectively. Berman et al. (18) reported a hard-event rate of 0.2% in patients with normal or equivocal exercise 99mTc-sestamibi studies and 7.5% in patients with abnormal results over a follow-up period of 20 mo. Geleijnse et al. (19) reported that, in 392 patients, hard cardiac-event rates were 0.8%/y and 6.8%/y in subjects with normal and abnormal dobutamine 99mTc-sestamibi SPECT scintigraphy, respectively. A recent study of Hachamovitch et al. (20) applied a dual-isotope protocol (rest thallium and exercise sestamibi) in 2,113 patients. The event rates were 0.3%, 4.7%, and 10% over the 19-mo follow-up period for subjects with a normal study, mildly abnormal study, and severely abnormal study, respectively.
Our study implies that dobutamine tetrofosmin scintigraphy can differentiate patients into low-risk and high-risk categories, with event rates after a normal study comparable with that reported in patients undergoing sestamibi imaging. The observed limitations of tetrofosmin with regard to the low extraction fraction and estimation of the extent of hypoperfusion were reported with vasodilator stress and, therefore, similar findings may not apply with exercise or exercise simulating stress modalities such as dobutamine. In a recent study by Galassi et al. (23), 459 patients underwent exercise tetrofosmin SPECT. During follow-up perfusion, 15 cardiac deaths occurred, compared with 62 in our study, probably reflecting the higher risk status in patients who were unable to perform exercise stress test.
Several studies have shown a relationship between the extent and severity of 99mTc-sestamibi perfusion defects and the prognosis. In our study, this issue was addressed, and the extent and severity of 99mTc-tetrofosmin perfusion defects were expressed by the SSS and SRS and evaluated as a continuous variable. The univariate analysis showed that SSS and SRS were predictors of cardiac death, cardiac death or (re)infarction, and all cardiac events. Furthermore, the SSS was a predictor for late coronary revascularization. A recent study by Hachamovitch et al. (20) reported that the extent and severity of reversible defects present on dual-isotope SPECT scans (as measured by the SDS) provided important prognostic information. In line with this, our study shows that the SDS, which represents the amount of stress-induced ischemia, is a strong predictor of the need for coronary revascularization and all future cardiac events. Nevertheless, in univariate and in multivariate analyses, the most powerful predictor of cardiac events was an abnormal scan (Tables 2 and 3).
Previous studies have revealed the safety and feasibility of high-dose dobutamine-atropine stress testing (24–28). Consistently, dobutamine-atropine stress testing was accomplished in this study without serious side effects: No sustained ventricular tachycardia, ventricular fibrillation, myocardial infarction, or death occurred. Side effects were generally well tolerated and rarely required termination of the study (24–28).
Although the feasibility of the test was high, 7% of patients had an inconclusive test (failure to achieve the target heart rate or to show a perfusion abnormality). The feasibility and perhaps the prognostic value could have been even higher if β-blocker therapy was routinely discontinued before the stress test.
CONCLUSION
Dobutamine-atropine stress 99mTc-tetrofosmin SPECT is a useful imaging method for distinguishing patients at high and low risk of future cardiac events. The presence of perfusion abnormalities provides incremental prognostic information in addition to clinical, stress electrocardiographic, and hemodynamic data. Patients with normal perfusion studies have a low rate of cardiac death (1%). The presence of abnormal perfusion was associated with an 8-fold increase in the risk of cardiac events.
Acknowledgments
The authors thank the general practitioners for their assistance in the patient follow-up.
Footnotes
Received Aug. 29, 2001; revision accepted Jan. 31, 2002.
For correspondence and reprints contact: Don Poldermans, MD, PhD, Department of Cardiology, Thoraxcenter, Room Ba 300, Erasmus Medical Center Rotterdam, Dr. Molewaterplein 40, 3015 GD Rotterdam, The Netherlands.
E-mail: poldermans{at}hlkd.azr.nl
REFERENCES
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Risk Stratification With Electrocardiographic-Gated Dobutamine Stress Imaging
- Prognostic Value of Dobutamine Stress Myocardial Contrast Perfusion Echocardiography
- Prognostic Stratification Using Dobutamine Stress 99mTc-Tetrofosmin Myocardial Perfusion SPECT in Elderly Patients Unable to Perform Exercise Testing
- Dobutamine Stress Myocardial Perfusion Imaging in Coronary Artery Disease