


Abstract
Information on the prognostic value of noninvasive stress imaging techniques in the elderly is relatively scarce. This study assessed the prognostic value of dobutamine stress 99mTc-tetrofosmin SPECT for the prediction of mortality and cardiac events in elderly patients. Methods: Clinical information and SPECT results were analyzed for 272 consecutive patients ≥ 65 y old (mean age, 71 ± 5 y; range, 65–87 y) with limited exercise capacity. Follow-up was complete in 270 patients (99.3%); 23 underwent revascularization within 60 d of the scintigraphy and were excluded. Abnormal findings were defined as the presence of a fixed or reversible perfusion defect. A summed stress score was obtained to estimate the extent and severity of perfusion defects. The incremental prognostic value of SPECT over clinical data was evaluated according to 3 multivariate models, which included any SPECT abnormality, the presence of a fixed or reversible defect, and the summed stress score. Results: During the follow-up (3.3 ± 1.4 y), 59 patients died (29 cardiac deaths), 16 had a nonfatal infarction, and 49 underwent late revascularization. Abnormal scan findings were present for 140 patients (57%). The annual event rates for total mortality, cardiac death, and cardiac death or nonfatal infarction were, respectively, 3.2%, 0.2%, and 0.7% when scan findings were normal and, respectively, 9.5%, 4.3%, and 8% when scan findings were abnormal (all P < 0.0001). Multivariate analysis showed that abnormal scan findings, the presence of a fixed or reversible defect, and the summed stress score provided incremental prognostic information over clinical data. The presence of abnormal scan findings was independently associated with an increased risk for total mortality, cardiac death, and cardiac death or nonfatal infarction (respectively, hazard ratio 3.4 [95% CI, 1.8–6.5], 12.1 [95% CI, 2.9–51.5], and 9.0 [95% CI, 2.8–29.6]). Conclusion: Dobutamine stress 99mTc-tetrofosmin SPECT provides incremental prognostic information for the prediction of total mortality and cardiac events in elderly patients.
The population of the Western world is aging, and the proportion of elderly patients in cardiovascular practice will further increase in the next 2 decades (1). Cardiovascular disease is the most common cause of morbidity and mortality in patients older than 65 y (1). Coronary angioplasty and coronary bypass surgery have become more available for elderly patients and may substantially improve short- and long-term outcome in high-risk patients (2). Prognostic evaluation in elderly patients with suspected or known coronary artery disease can distinguish high-risk patients who may benefit from an invasive approach from low-risk patients who do not require invasive procedures. Unfortunately, information on prognostic stratification by noninvasive testing in elderly patients is relatively limited (3,4). The feasibility of exercise stress testing in elderly patients is often unsatisfactory because of lack of physical fitness and the presence of comorbid conditions such as degenerative joint disease, claudication, and peripheral neuropathy. Pharmacologic stress myocardial perfusion SPECT is a feasible alternative. However, data on the prognostic value of this technique in elderly patients are scarce (3,4). The purpose of this study was to determine the prognostic value of dobutamine 99mTc-tetrofosmin SPECT for the prediction of total mortality and cardiac events in elderly patients unable to perform exercise testing.
MATERIALS AND METHODS
Study Population
A total of 272 consecutive patients ≥ 65 y old and unable to perform exercise testing underwent dobutamine stress 99mTc-tetrofosmin SPECT for the evaluation of suspected or known coronary artery disease. Follow-up was complete for 270 (99.3%) of 272 patients. Twenty-three patients underwent myocardial revascularization within 60 d of the scintigraphy and were excluded from analysis. This exclusion was based on previous data indicating that in the first 60 d after the test, referral for myocardial revascularization tends to be based on the SPECT results, whereas >60 d after testing, referral for myocardial revascularization tends to be based on deterioration of the patient’s clinical status (5). Accordingly, the prognostic data reported are based on 247 patients. A total of 48 patients (19%) were >75 y old. In 119 patients (48%), the stress myocardial perfusion imaging was performed to evaluate known coronary artery disease; 89 of them had a previous myocardial infarction, and 30 had proven coronary artery disease without previous infarction. The remaining 128 patients (52%) had suspected coronary artery disease and underwent imaging for diagnostic reasons. Ninety-seven patients (39%) had typical angina, 60 (24%) had atypical angina, and 34 (14%) had nonanginal symptoms. All patients gave informed consent before the test. The local Medical Ethics Committee approved the study protocol.
Before dobutamine stress 99mTc-tetrofosmin SPECT, a structured clinical interview and history were acquired and cardiac risk factors were assessed. Hypertension was defined as a blood pressure ≥ 140/90 mm Hg or treatment with antihypertensive medication. Diabetes mellitus was defined as a fasting glucose level ≥ 7.8 mmol/L or the need for insulin or oral hypoglycemic medication. Hypercholesterolemia was defined as a total cholesterol ≥ 6.4 mmol/L or treatment with lipid-lowering medication.
Dobutamine Stress Testing
Dobutamine stress testing was performed according to a standard protocol as previously reported (6). Dobutamine was infused through the antecubital vein, starting at a dose of 10 μg/kg/min for 3 min and increasing by 10 μg/kg/min every 3 min up to a maximum dose of 40 μg/kg/min. If the test endpoint was not reached at a dobutamine dose of 40 μg/kg/min, atropine (up to 1 mg) was given intravenously. Blood pressure and heart rate were monitored and electrocardiography was recorded constantly. Test endpoints were achievement of target heart rate (85% of maximum age- and sex-predicted heart rate); horizontal or downsloping ST-segment depression > 2 mm at an interval of 80 ms after the J-point, compared with baseline; ST-segment elevation > 1 mm in patients without previous myocardial infarction; severe angina; a systolic blood pressure fall > 40 mm Hg, compared with baseline; blood pressure > 240/120 mm Hg; or significant cardiac arrhythmias. Metoprolol was available to reverse the adverse effects of dobutamine/atropine.
SPECT
Approximately 1 min before the termination of the stress test, an intravenous dose of 370 MBq of 99mTc-tetrofosmin was administered (6). For resting studies, 370 MBq of tetrofosmin were injected at least 24 h after the stress study. Image acquisition was performed with a triple-head γ-camera system (Prism 3000 XP; Picker International). For each study, 6 oblique (short axis) slices from the apex to the base and 3 sagittal (vertical long axis) slices were defined. Each of the 6 short-axis slices was divided into 8 equal segments. The septal part of the 2 basal slices was excluded from analysis because this region corresponds to the fibrous portion of the interventricular septum and normally exhibits reduced uptake. Therefore, 47 segments were identified (3 long axis and 44 short axis). The SPECT scoring model has been described previously (6) and has been depicted previously by Salustri et al. (7). The scan was interpreted semiquantitatively by visual analysis assisted by analysis of the circumferential profiles. Rest and stress images were evaluated by measuring the area between the lower limit of normal and the actual circumferential profile in 6 short-axis slices. Profile curves 2 SDs below normal perfusion were considered abnormal. Stress and rest tomographic views were reviewed side by side by an experienced observer who was unaware of each patient’s clinical data. A reversible perfusion defect was defined as a perfusion defect on stress images that partially or completely resolved at rest in ≥2 contiguous segments or slices in the 47-segment model. A fixed perfusion defect was defined as a perfusion defect on stress images in ≥2 contiguous segments or slices that persisted on rest images in the 47-segment model. A study was considered to have abnormal findings if a fixed or reversible perfusion defect (or both) was present. To identify the coronary artery related to the location of the perfusion defect, the 47 segments imaged by SPECT were combined into 6 major regions: anterior, inferior, septal anterior, septal posterior, posterolateral, and apical. This combination provides easily interpretable information for the treating cardiologist. Each of the 6 major left ventricular segments was scored using a 4-grade scoring method (0 = normal, 1 = slightly reduced, 2 = moderately reduced, and 3 = severely reduced or absence of uptake). The perfusion defect score was derived by summing the score of the 6 myocardial segments at stress (summed stress score).
Patient Follow-up
The follow-up data were obtained by reviewing hospital records and by contacting the patient’s general practitioner. The date of the last examination or consultation was used to determine follow-up time. Endpoints were overall death, cardiac death, nonfatal myocardial infarction, and late (>60 d) coronary revascularization. Cardiac death was defined as death caused by myocardial infarction, significant cardiac arrhythmias, or refractory congestive heart failure. Sudden death occurring without another explanation was included as cardiac death. Myocardial infarction was defined according to standard criteria (8).
Statistical Analysis
Continuous data were expressed as mean ± SD, and percentages were rounded. Statistical analysis was performed with the BMDP statistical software package (BMDP Statistical Software Inc.). Continuous variables were compared using the Student t test for unpaired samples. Differences between proportions were compared using the χ2 test. Univariate and multivariate Cox proportional hazards regression models were used to identify independent predictors of total mortality and cardiac events (9). Variables were selected in a stepwise forward-selection manner, with entry and retention set at a significance level of 0.05. The risk of a variable was expressed as a hazard ratio with a corresponding 95% confidence interval. The incremental value of myocardial perfusion scintigraphy over the clinical variables in the prediction of events was determined according to 3 models. In model 1, the incremental value of abnormal scan findings over clinical data and stress test information was assessed. In model 2, the presence of a fixed or reversible defect was entered. In model 3 the summed stress score was entered. The probability of survival was calculated using the Kaplan-Meier method, and survival curves were compared using the log-rank test. P < 0.05 was considered statistically significant.
RESULTS
Demographics and Stress Test Results
Clinical data are presented in Table 1. Dobutamine stress increased heart rate significantly (from 72 ± 15 to 128 ± 16 bpm, P < 0.001) and increased systolic blood pressure modestly (from 140 ± 23 to 146 ± 31 mm Hg, P < 0.001). The highest dobutamine dose was 10 μg/kg/min in 1 patient (0.4%), 20 μg/kg/min in 44 (18%), 30 μg/kg/min in 45 (18%), and 40 μg/kg/min in 157 (64%). In 88 patients (36%), atropine was added. Patients who were using β-blocker therapy during the dobutamine stress test more frequently received atropine than did patients not receiving β-blocker therapy (54 of 105, 51%, vs. 34 of 142, 24%, P < 0.001). Side effects that occurred during dobutamine stress testing were generally self-limiting. These included atrial fibrillation in 5 patients (2.0%), short ventricular tachycardia (<10 complexes) in 6 patients (2.4%), and severe hypotension (decrease in systolic blood pressure > 40 mm Hg) in 4 patients (1.6%). Minor side effects included nausea in 4 (1.6%), flushing in 3 (1.2%), and headache in 13 (5.3%). No patient experienced a myocardial infarction or ventricular fibrillation during or immediately after the stress test.
Clinical Characteristics
SPECT and Outcome Events
A total of 107 patients (43%) had normal perfusion, and 140 (57%) had abnormal perfusion. In these 140 patients, perfusion abnormalities were reversible in 20 (14%), fixed in 67 (48%), and both fixed and reversible (or partially reversible) in 53 (38%). During a mean follow-up of 3.3 ± 1.4 y, 59 deaths (24%) occurred, of which 29 (12%) were due to cardiac causes. Nonfatal myocardial infarction occurred in 16 patients (6%). Forty-nine patients (20%) underwent late (>60 d) myocardial revascularization (28 patients had coronary bypass surgery, and 21 had coronary angioplasty).
Predictive Value of Clinical Data and Test Results
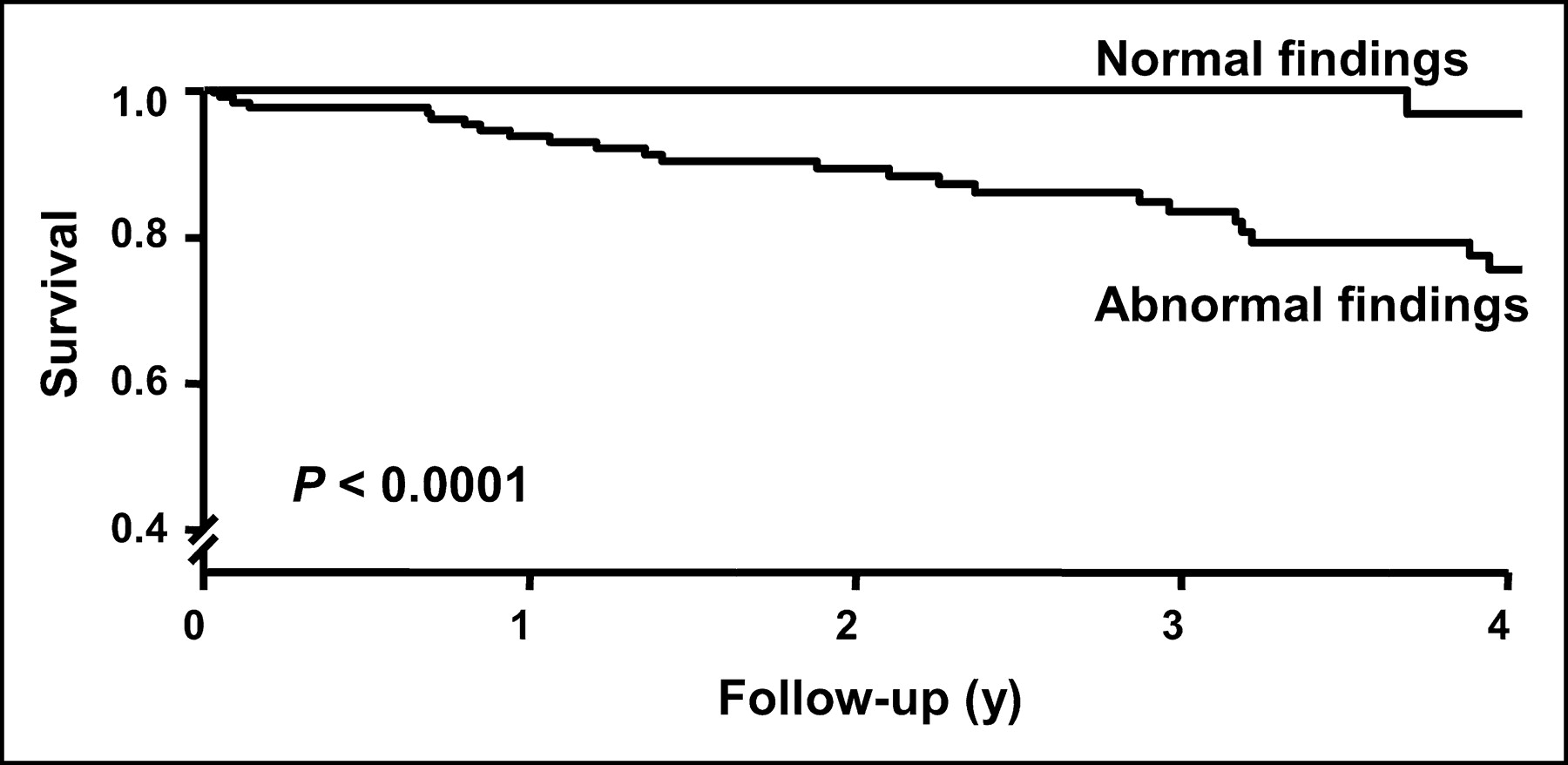
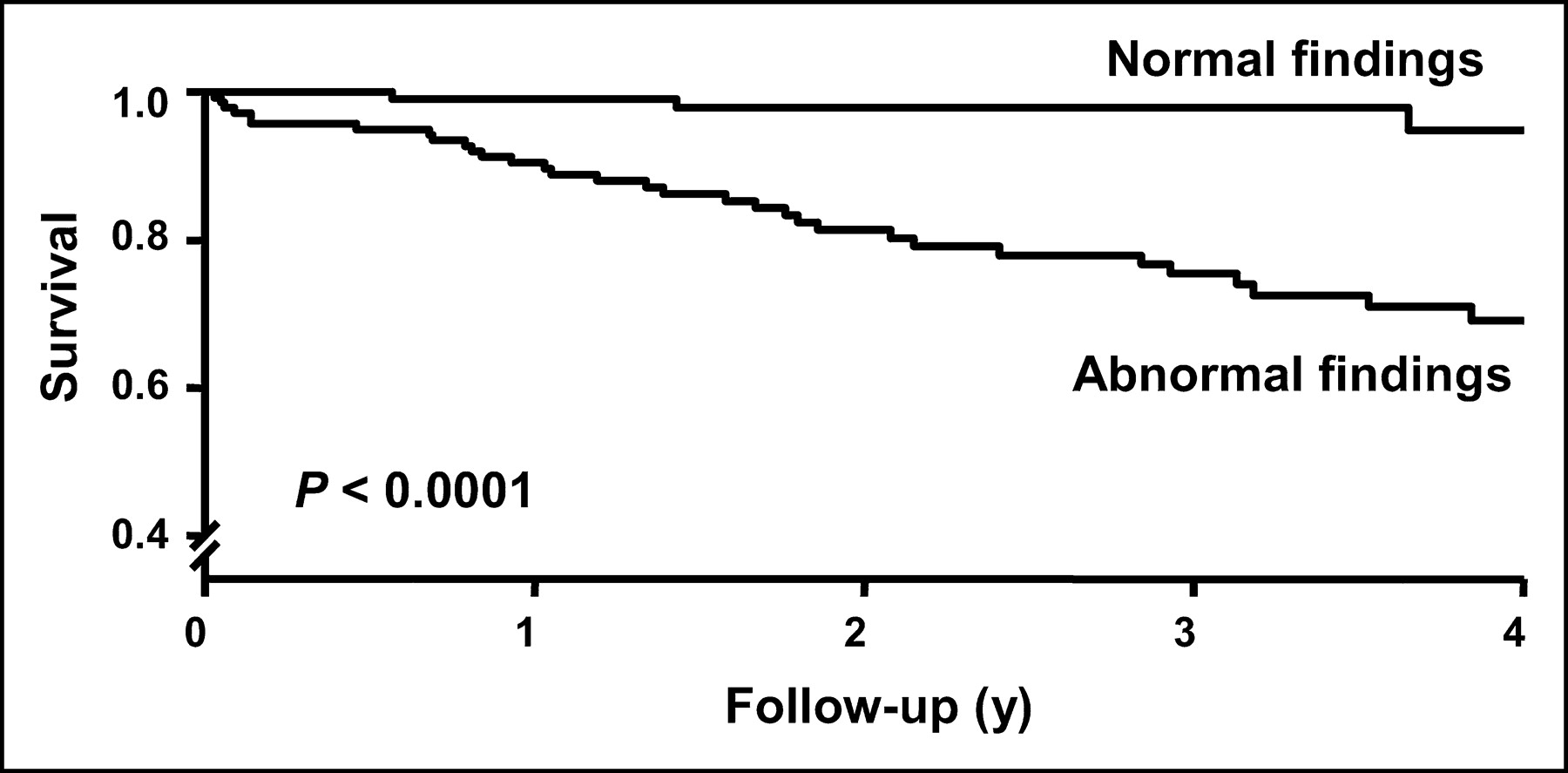
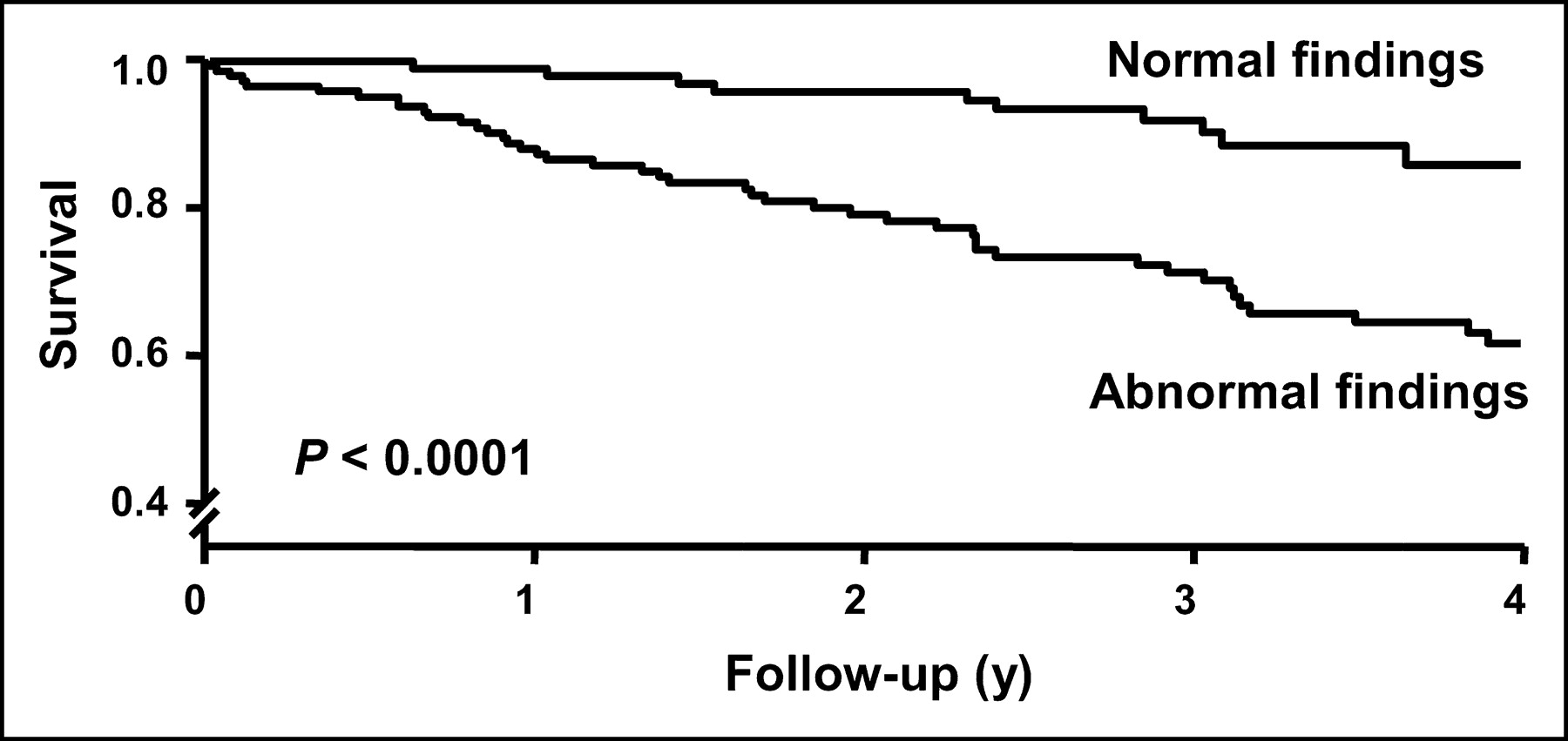
Kaplan-Meier survival curves and cumulative event rates are presented in Figures 1–3. Patients with normal perfusion had a low event rate. Remarkably, no cardiac deaths occurred during the first 3 y after the test in those whose test results were normal. Survival curves continued to diverge during follow-up, indicating that the prognostic value of dobutamine stress 99mTc-tetrofosmin SPECT was maintained over time. The annual event rates for total mortality, cardiac death, and cardiac death or nonfatal infarction were, respectively, 3.2%, 0.2%, and 0.7% after a scan with normal findings and, respectively, 9.5%, 4.3%, and 8% after a scan with abnormal findings (all P < 0.0001).

Kaplan-Meier survival curves for total mortality according to results of dobutamine stress 99mTc-tetrofosmin SPECT.
Kaplan-Meier survival curves for cardiac death according to results of dobutamine stress 99mTc-tetrofosmin SPECT.
Kaplan-Meier survival curves for cardiac death or nonfatal myocardial infarction according to results of dobutamine stress 99mTc-tetrofosmin SPECT.
Univariate and multivariate predictors of total mortality and cardiac events are presented in Tables 2–4. Theincremental prognostic value of dobutamine stress 99mTc-tetrofosmin SPECT over clinical data was assessed using the 3 models. All models provided incremental information over clinical and stress test data. Model 1, which included any abnormal scan finding, offered the most powerful incremental information for the prediction of total mortality (global χ2 = 26; P < 0.05). Model 2, which included both fixed and reversible perfusion defects, provided the most powerful incremental information for the prediction of cardiac death, as well as of cardiac death or nonfatal infarction (global χ2 = 53 and 51, respectively; P < 0.0001).
Univariate and Multivariate Predictors of Total Mortality
Univariate and Multivariate Predictors of Cardiac Death
Univariate and Multivariate Predictors of Cardiac Death or Myocardial Infarction
DISCUSSION
This study assessed the prognostic value of dobutamine stress 99mTc-tetrofosmin SPECT in the prediction of mortality and hard cardiac events in elderly patients. Despite their advanced age, patients with normal myocardial perfusion findings had an excellent outcome, with no cardiac deaths during the first 3 y after a normal test. In contrast, patients with abnormal myocardial perfusion findings had an elevated risk of future cardiac events. 99mTc-Tetrofosmin SPECT provided prognostic information incremental to clinical and stress test parameters for the prediction of total mortality and cardiac events during a nearly complete follow-up of 3.3 ± 1.4 y. Independent clinical predictors of total mortality were smoking and congestive heart failure. Independent clinical predictors of cardiac events were diabetes mellitus, smoking, and congestive heart failure. Furthermore, the presence of a left bundle branch block was predictive of cardiac death. 99mTc-Tetrofosmin SPECT provided incremental prognostic information over clinical and stress test parameters. The multivariate model that included any scan abnormality provided the most powerful incremental information for the prediction of total mortality. The multivariate model that included both fixed and reversible perfusion defects offered the most powerful incremental information for the prediction of cardiac death, as well as of cardiac death or nonfatal infarction. Moreover, multivariate analysis showed that the summed stress score, which indicates the extent and severity of perfusion abnormalities, provided incremental prognostic information over clinical data. These results demonstrate that the evaluation of elderly patients using dobutamine stress 99mTc-tetrofosmin SPECT is a safe and feasible method that provides clinically useful information on clinical outcome.
Previous data indicate that dobutamine stress 99mTc-tetrofosmin SPECT is safe and feasible in elderly patients (10). However, information on the prognostic value of stress myocardial perfusion imaging in the elderly is scarce. Furthermore, there are no data to support a role of stress myocardial perfusion imaging in the prediction of all causes of mortality in the elderly. Currently, prognostic data on sestamibi SPECT in the elderly are not available. Iskandrian et al. (11) assessed the use of exercise 201Tl imaging for the prognostic stratification of 404 elderly patients with a mean age of 65 y (range, 60–82 y). During a follow-up of 25 ± 15 mo, 8 (2%) died of cardiac causes, and 10 (2%) had nonfatal myocardial infarction. Patients with abnormal exercise 201Tl findings had higher event rates than did those with normal findings (8% vs. 1%, P < 0.001). Steingart et al. (12) followed 578 patients aged 65 y or older (range, 65–85 y) using exercise myocardial perfusion imaging. Almost 80% underwent 201Tl SPECT; the remainder underwent 99mTc-sestamibi imaging. During a follow-up of 4.4 ± 1.3 y, 39 deaths and 17 nonfatal myocardial infarctions occurred. The authors concluded that treadmill exercise is a valuable tool in elderly patients with adequate exercise capacity and that myocardial perfusion imaging added only modest prognostic information. The event rate was lower than for our study, as may be explained by our inclusion of patients unable to perform exercise testing, who are generally recognized as a higher-risk group, compared with patients who can exercise (13). Shaw et al. (14) studied 348 patients ≥ 70 y old using dipyridamole 201Tl imaging. During a follow-up of 23 ± 15 mo, there were 52 cardiac deaths (15%) and 24 nonfatal myocardial infarctions (7%). The event rate for cardiac death or nonfatal infarction was 2% in patients with normal scan findings and 20% in patients with abnormal scan findings. Abnormal (reversible or fixed perfusion defect) dipyridamole 201Tl findings were the best predictor of cardiac events.
The 0.7% hard cardiac event rate in patients with normal dobutamine stress 99mTc-tetrofosmin SPECT findings is substantially lower than the hard cardiac event rate in patients with normal 201Tl findings (11,12,14). This difference may be related to the better imaging characteristics of 99mTc-tetrofosmin than of 201Tl. Clinical trials have demonstrated that 99mTc-tetrofosmin SPECT provides diagnostic and prognostic information comparable to that derived from traditional 201Tl imaging, with the extra benefit of higher image quality and increased certainty in interpretation (15–17). This study expands the body of literature regarding the prognostic utility of this relatively new radioactive isotope in patients with known or suspected coronary artery disease. The study also is, to our knowledge, the first to support a role of stress myocardial perfusion imaging in the prediction of all causes of mortality in the elderly. The present data indicate that elderly patients with normal dobutamine stress 99mTc-tetrofosmin myocardial perfusion findings have a favorable prognosis during the 3 y after the study if no change in clinical status occurs. There have been several attempts to quantify the low-risk period after a scan with normal findings is obtained (18). Prognostic information derived from exercise sestamibi SPECT demonstrates that repeated testing should be not required up to 4 or 5 y after a study with normal findings; however, when symptoms arise or clinical status changes, retesting and subsequent angiography and revascularization may be required (19). Further studies are needed to confirm these data in elderly patients. The left ventricular ejection fraction was not available in all patients; this is a limitation of the study.
CONCLUSION
Dobutamine stress 99mTc-tetrofosmin SPECT provides incremental prognostic information for the prediction of all causes of mortality and hard cardiac events in the elderly. Elderly patients with normal myocardial perfusion findings have a good prognosis and do not require further invasive evaluation during the 3 y after the study if no change in clinical status occurs.
Footnotes
Received May 24, 2004; revision accepted Aug. 12, 2004.
For correspondence or reprints contact: Arend F.L. Schinkel, MD, PhD, Thoraxcenter Room Ba 302, Erasmus Medical Center, Dr. Molewaterplein 40, 3015 GD Rotterdam, The Netherlands.
E-mail: arendschinkel{at}hetnet.nl
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons
- 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons
- Testing of Low-Risk Patients Presenting to the Emergency Department With Chest Pain: A Scientific Statement From the American Heart Association
- Prognostic Implications of Myocardial Perfusion Single-Photon Emission Computed Tomography in the Elderly
- The Year in Cardiac Imaging