


Abstract
This study was conducted to determine the ability of 18F-FDG PET and conventional imaging (CI) to predict the outcomes in breast cancer patients who have previously undergone primary treatment. Methods: The study population consisted of 61 female patients (median age, 54 y; range, 32–91 y) who were reevaluated with 18F-FDG PET and CI after treatment. The median interval between the last treatment and PET was 0.4 y (range, 0–16 y). PET was performed within 3 mo of CI (median interval, 25 d; range, 2–84 d). To determine the independent impact of PET on outcome, PET images were reinterpreted in a blind fashion. Availability of clinical information after PET scanning (21 ± 12 mo) was required for study inclusion. Study endpoints were clinical evidence of progression of disease or death. Results: Of 61 patients, 19 (31.1%) had no clinical evidence and 38 (62.3%) had evidence of residual or recurrent disease by the end of follow-up. Four patients (6.6%) had died. The positive and negative predictive values (PPV and NPV, respectively) of PET were 93% and 84%, respectively. CI yielded a PPV of 85% and an NPV of 59%. The prognostic accuracy of single whole-body PET was superior to that of multiple procedures with CI (90% vs. 75%; P < 0.05). Kaplan–Meier estimates of disease-free survival in patients with negative PET findings compared with those with positive PET findings revealed a significant difference between the 2 curves (log-rank test = 0.001). Kaplan–Meier estimates of disease-free survival stratified by CI results showed a marginally significant difference between CI-positive and CI-negative patients (log-rank test = 0.04). Conclusion: FDG PET can be used to improve prediction of the clinical outcome of previously treated breast cancer patients relative to what is achievable through CI alone.
Breast cancer is accurately detected, staged, and restaged by FDG PET (1–14). FDG PET has also been used successfully for monitoring tumor response to chemotherapy (15–19). However, it is unknown whether FDG PET predicts the outcomes in breast cancer patients after primary treatment with a similar or better accuracy than that of conventional imaging (CI).
Routine evaluation for recurrent or residual disease after breast cancer treatment includes physical examination and imaging tests such as mammography, CT, MRI, sonography, and radionuclide whole-body imaging. These tests are frequently performed as routine clinical follow-up or are prompted by rising levels of tumor markers or, in some cases, by patient symptoms. Some metastatic sites such as lymph nodes or bone marrow are not easily depicted by CI modalities, resulting in delayed diagnosis and therapeutic interventions.
Several authors have provided evidence that PET is more sensitive than CI for establishing the extent of metastatic breast cancer involvement (2,13,20–22). However, these studies were conducted on patients who underwent initial staging before treatment and did not address the prognostic significance of whole-body PET imaging on patients who have previously undergone primary breast cancer treatment.
Using disease progression or death as its endpoints, the current study examined the ability of 18F-FDG PET and CI to predict the clinical outcomes in previously treated breast cancer patients.
MATERIALS AND METHODS
Sixty-one female patients (mean age, 54 y; range, 32–91 y) who underwent whole-body PET for evaluation of breast cancer after treatment between July 1997 and June 2000 were enrolled in this study.
The initial histopathologic diagnosis was infiltrating ductal carcinoma in 45 patients (73.8%), infiltrating lobular carcinoma in 9 patients (14.8%), and apocrine carcinoma in 1 patient (1.6%). No histologic tissue classification was available for 6 patients (9.8%).
Inclusion Criteria
The following inclusion criteria were required for the patient’s enrollment in the study: (a) availability of CI reports performed within 3 mo of PET, (b) availability of follow-up data for a minimum of 6 mo after scanning, and (c) unequivocal determination of clinical status at the time of the last clinical follow-up.
Clinical Scenario
After initial diagnosis, patients underwent a variety of treatments. Surgery (lumpectomy or mastectomy) was performed on all patients. Forty-six patients (75.4%) underwent chemotherapy and 34 (55.7%) received radiation therapy. The median interval between the last treatment and PET was 0.4 y (range, 0–16 y).
Clinical whole-body PET imaging was ordered for the following indications: Forty-two patients (68.8%) were being evaluated for residual or recurrent disease without any specified reason, 10 (16.4%) had increasing levels of serum tumor markers, and 9 (14.8%) had equivocal or suspicious findings by CI. The follow-up period after PET averaged 21 ± 12 mo (median, 17 mo; range, 6–42 mo).
The clinical status, as determined by the treating physician or chart review (or both), at the time of the last follow-up was used to categorize patients as free of disease or having disease. The latter group consisted of patients who at the time of last follow-up had stable or progressive disease or had died.
Clinical PET Imaging Protocol
Patients fasted for at least 6 h before receiving an intravenous injection of 370–555 MBq 18F-FDG. PET was performed with an ECAT EXACT or HR+ system (CTI/Siemens, Knoxville, TN).
The standard clinical imaging protocol started 45–60 min after tracer injection. Images were acquired over 6–8 bed positions. Images were acquired with (n = 11) or without (n = 50) attenuation correction and were reconstructed using filtered backprojection or algebraic algorithms (23).
Image Interpretation and Classification
To determine the independent prognostic value of PET, images were reinterpreted by an experienced reader who was unaware of other clinical findings. Imaging findings were dichotomized as positive or negative for residual or recurrent cancer.
Written clinical reports of conventional images were reviewed and classified as (a) negative, if all imaging tests were negative for disease; (b) equivocal, when abnormal findings were present on any imaging test but were not interpreted as suspicious for malignancy; (c) suspicious, if any test result was clearly described as suspicious for malignancy; or (d) positive, if findings were described as consistent with malignancy. To dichotomize the data, negative and equivocal findings were subclassified as negative, and suspicious and positive findings were categorized as positive.
The clinical impression was derived from follow-up CI studies on 56 patients, biopsy of abnormalities on 18 patients, and rising tumor markers in 3 patients. The outcome of patients with true-positive PET but false-negative CI findings was verified by CI follow-up in all 6 patients, rising levels of tumor markers in 1 patient, and biopsy in another 2 patients. This information was then evaluated and categorized as stable or progressive disease. Thus, patients were considered stable if the above tests did not indicate progression of disease.
Statistical Analysis
Positive and negative predictive values (PPV and NPV, respectively) and accuracy were calculated by standard methods. Categoric data were examined using the χ2 test, with Fisher’s exact test if expected cell counts were <5. Probability of disease-free survival was computed by Kaplan–Meier analysis. The log-rank test was used to evaluate the differences between Kaplan–Meier curves. All statistical tests were performed at the 5% level of significance.
RESULTS
Reevaluation by PET after treatment was performed within 3 mo of CI (median, 25 d; range, 2–84 d). A total of 189 CI procedures, or 3.2 ± 1.4 procedures per patient, was performed. The imaging procedures performed included whole-body bone scanning (n = 40), chest CT (n = 35), abdominopelvic CT (n = 33), chest radiography (n = 24), MRI of the breast and other MRI (n = 26), sonography of the breast (n = 10), mammography (n = 16), and other procedures (n = 5).
At the time of the last follow-up, 19 of 61 patients (31.1%) were considered free of disease, whereas 38 of 61 patients (62.3%) had clinical evidence of stable or progressive disease. The remaining 4 patients (6.6%) had died.
CI yielded negative results in 22 patients (36%) (negative findings, n = 14; equivocal findings, n = 8) and positive results in 39 patients (64%) (positive findings, n = 24; suspicious findings, n = 15). PET showed negative findings in 19 patients (31.1%) patients, whereas 42 patients (68.9%) had evidence for disease on PET.
PET and CI were concordant in 46 of 61 patients (75%), 33 in which they were both positive and 13 in which they were both negative. All 33 of these positive cases were true-positive cases (PPV = 100%), and 10 of these negative cases were true-negative cases (NPV = 77%). PET and CI were discordant in the remaining 25% of patients, 9 which were positive on PET but negative on CI and 6 which were negative on PET but positive on CI. PET correctly predicted the clinical outcome in 12 of these 15 discordant cases (80%), whereas CI was correct in only 3 cases (20%), all of which were positive on PET but negative on CI (Table 1).
Imaging Findings Versus Clinical Outcome
Using the clinical outcome as the gold standard, blind PET evaluation yielded a sensitivity of 93% versus 79% for CI (P < 0.05). The specificity tended to be higher for PET than for CI (84% vs. 68%; P = 0.065). The PPV of PET was similar to that of CI (93% vs. 85%; P = 0.24). The NPV and predictive accuracy of blind PET evaluation were significantly higher than those of CI (84% vs. 59% [P < 0.05] and 90% vs. 75% [P < 0.05]) (Table 2).
Prognostic Value of PET and CI
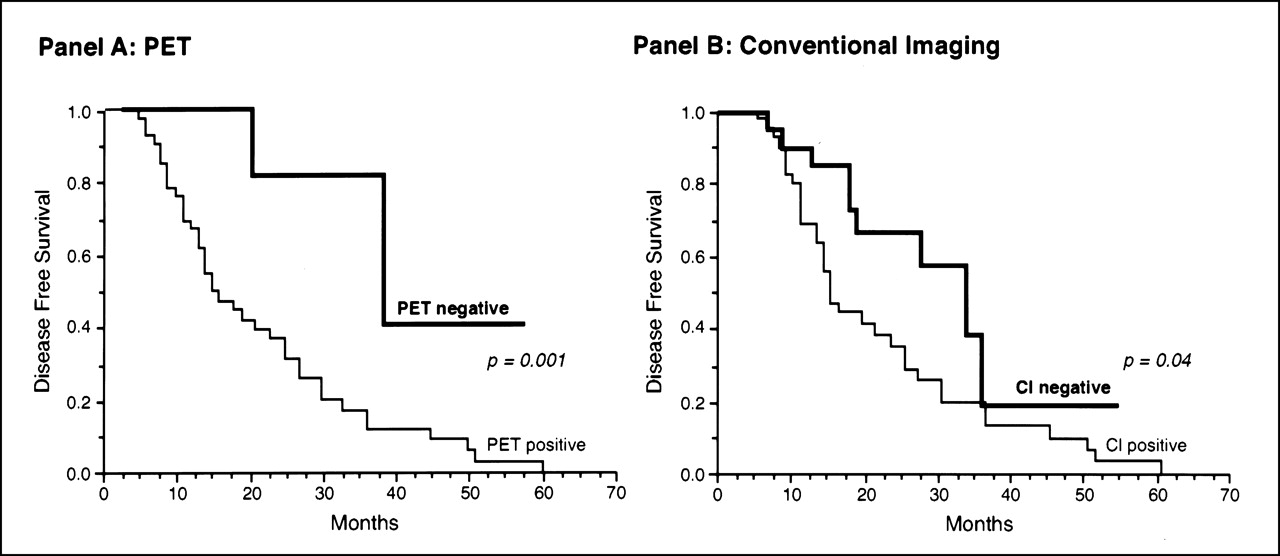
Kaplan–Meier estimates of disease-free survival in 19 patients with negative findings on PET were compared with those of 42 patients who had positive results on PET: The 2 survival curves differed significantly (log-rank test = 0.001). Kaplan–Meier estimates of disease-free survival in patients with negative CI findings (n = 22) compared with those with positive findings (n = 39) revealed a marginally significant difference between the 2 curves (log-rank test = 0.04) (Fig. 1).
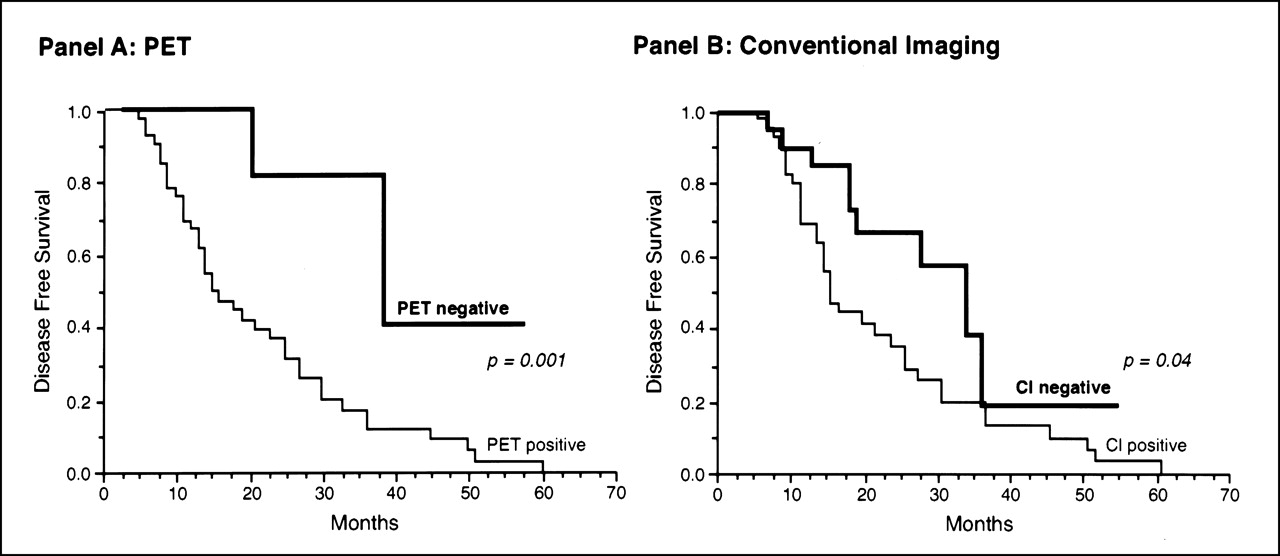
(A) Kaplan–Meier estimate of disease-free survival in 42 patients with positive PET findings compared with 19 patients with negative PET findings. P = 0.001 (log-rank test). (B) Kaplan–Meier estimate of disease-free survival in 22 patients with negative CI findings compared with 39 patients with positive CI findings. P = 0.04 (log-rank test).
DISCUSSION
This study shows the higher accuracy of 18F-FDG PET compared with combined CI modalities for predicting outcome in breast cancer patients who were reevaluated after primary treatment. Breast cancer patients commonly undergo numerous imaging studies after initial treatment even though the therapeutic options for patients with recurrent or residual disease are limited. Nevertheless, detection of local recurrence and metastatic disease can impact therapy. Local recurrence and axillary lymph node involvement may be treated surgically or with radiation therapy, whereas mediastinal lymph node involvement or distant metastases typically require chemotherapy or radiation therapy (or both) (24). The most frequently used staging examinations include plain roentgenography of the chest and bones; CT of the chest, abdomen, and pelvis; sonography; MRI; mammography; and whole-body radionuclide bone scanning.
In this study, patients underwent an average of 3.2 CI tests within 3 mo of PET and many more throughout the course of the disease. This study indicates that PET provides more accurate prognostic information than the combination of other imaging tests.
All patients enrolled in the study underwent reevaluation after treatment by CI and were followed for almost 2 y. Most patients (42/61 [68.9%]) had clinical evidence for disease at the time of the last follow-up. Clinical outcome was clearly defined in all patients and was used as a gold standard for determining the predictive accuracy of PET and CI. The predictive accuracy of PET was significantly better than that of CI (90% vs. 75%; P < 0.05). However, false-positive and false-negative findings on PET were found in 6 of 61 patients.
In all 3 cases with false-negative findings, rising levels of serum tumor markers represented the indication for PET. All 3 of these patients also had negative findings on CI. Interestingly, 2 of 3 patients with false-negative results had lobular carcinoma. Lobular carcinoma accounts for only 7%–10% of all invasive breast cancers (25–27) and exhibits lower glucose metabolic activity than invasive ductal carcinoma (28,29). These 3 patients remained asymptomatic for a mean period of 14.5 mo after PET imaging, at which time the metastatic disease was discovered. The sites of the metastatic lesions that were identified eventually were liver and bone in 1 patient, bone only in a second patient, and the anterior abdominal wall in the third patient.
PET yielded a significantly higher sensitivity (92.2%) than CI (78.6%) attributed to the larger number of false-negative results on CI. In 6 CI-negative cases, PET revealed recurrence, which was local in 1 patient, involved axillary and supraclavicular nodes in 1 patient (Fig. 2), involved mediastinal lymph nodes in 2 patients, and involved bone metastases in 2 patients. These results support previous studies that showed that lymph node metastasis and bone metastases are detected significantly more often on FDG PET than on CT or MRI (24). The CI tests performed on these patients included bone scanning (n = 5), CT or MRI of the chest (n = 6) and of the abdomen and pelvis (n = 4), and sonography (n = 1). All patients with positive findings on PET but negative findings on CI were treated with chemotherapy (n = 6), radiation (n = 3), and other treatments (n = 1).

PET images of patient with recurrent breast cancer involving left axillary and supraclavicular lymph nodes (arrows). MRI has been interpreted as consistent with fibrosis after radiation. PET findings were verified by biopsy. Left and right panels depict more anterior and more posterior coronal views, respectively.
PET yielded false-positive results in 3 patients. The false-positive results by PET resulted from uptake in a benign pleural effusion in 1 patient, physiologic muscle activity that was misinterpreted as lymph node involvement in a second patient, and uptake attributed to mastitis in the third patient.
In the group with positive CI findings (n = 39), PET was concordantly positive in 33 cases, and all of these patients had clinical evidence of relapse. The remaining 6 patients had false-positive results by CI. In 2 of these patients, CT showed suspicious lesions in the liver, conventional bone scan findings were suspicious for metastatic disease in 3 patients, and in 1 patient local recurrence was suspected by MRI of the breast. These 6 patients were monitored by other imaging tests and remained free of disease at the time of the last follow-up. Overall, among all cases in which PET and CI were discordant, PET was correct 4 times more frequently than CI (12/61 vs. 3/61 cases) and was correct in all discordant cases in which PET findings were negative.
This study has several limitations. First, patients were studied retrospectively, and only 25% of the 235 patients who underwent PET imaging after treatment for breast cancer had adequate follow-up. Specifically, no consistent information was available to further elucidate the exact time and location of disease recurrence in patients who had positive PET findings but negative CI findings. Nevertheless, to date, this is the largest study to determine the predictive value of 18F-FDG PET for patient outcome in treated breast cancer patients.
Second, the disease-free survival of breast cancer patients depends on accurate staging of the disease and also on further therapy initiated because of positive PET findings. In this study, 6 patients had true-positive PET findings but false-negative CI findings. All of these patients underwent further chemotherapy (n = 6) or radiation therapy (n = 3) and surgery (n = 1) (or all 3 treatments). Note that despite these therapeutic interventions, all patients had evidence of disease at the time of follow-up (3 with stable disease, 1 with progressive disease, and 2 who had died). Thus, 18F-FDG PET affected the management of these patients. However, the effect of these interventions cannot be determined with certainty from the current data. Treatment did not result in remission but might have delayed the progression of disease in some patients.
Third, dichotomizing the CI data as positive (for suspicious and positive findings) and negative (for negative and equivocal findings) might have skewed the results toward favoring PET. To address this issue, a subanalysis was performed that included only those patients who had unequivocal positive or negative findings on CI (n = 38). The sensitivity (81%) and the PPV (87.5%) of CI were similar to those of the entire population. The specificity and the NPV were 75% and 64%, respectively. The overall predictive accuracy of CI for this subset of the population was 79%, significantly lower compared with the predictive accuracy of PET for the same subset of the population (92%).
Fourth, written reports of CI tests, rather than rereading of studies, were used to determine the conventional test result. This approach was chosen because of the practical difficulties of obtaining original images from numerous different referral sites. On the other hand, PET images were reread because initial PET reading had been generally performed with full knowledge of the patient’s history and correlative image findings. This approach might have placed PET at an unfair advantage if we had not reread the PET scans. However, the separate analysis based on written clinical PET reports showed a significantly higher sensitivity and NPV of PET than those of CI findings, as with the blind readings, and the overall predictive accuracy of nonblind PET findings did not differ significantly from that of the blind PET interpretation.
Fifth, most PET images were acquired without attenuation correction because attenuation correction and iterative image reconstruction were not routinely performed in our clinic before January 2000. However, the attenuation correction is unlikely to change the diagnostic or predictive accuracy of PET (30,31).
Finally, study inclusion required that PET and CI needed to be performed within 3 mo of each other. Because CI was performed before PET, disease might have recurred during this time interval. To evaluate the effect of the study design on our results, we narrowed the time interval between CI and PET to 6 wk (median, 15 d; range, 2–40 d). Thirty-two patients underwent evaluation by PET and CI within that interval. The PPV, NPV, and predictive accuracy of PET were 95%, 90%, and 94%, respectively, which was significantly higher than the corresponding values for CI (75%, 50%, and 69%, respectively; P < 0.05). Moreover, the most significant impact of PET overall was an increase in the cases with true-negative PET but false-positive CI. Thus, the length of the time interval between PET and conventional studies was unlikely to have accounted for the current results.
CONCLUSION
18F-FDG PET can be used to improve prediction of the clinical outcome of previously treated breast cancer patients relative to what is achievable through CI alone.
Footnotes
Received Sep. 14, 2001; revision accepted Nov. 19, 2001.
For correspondence or reprints contact: Johannes Czernin, MD, Department of Nuclear Medicine, AR-277A CHS, UCLA School of Medicine, 10833 Le Conte Ave., Los Angeles, CA 90095-6942.
E-mail: jczernin{at}mednet.ucla.edu
REFERENCES
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Health Management of Breast Cancer Survivors
- 18F-FDG PET and PET/CT in the Evaluation of Cancer Treatment Response
- Tumor Metabolism and Blood Flow Changes by Positron Emission Tomography: Relation to Survival in Patients Treated With Neoadjuvant Chemotherapy for Locally Advanced Breast Cancer
- 18F-FDG PET/CT in Evaluating Non-CNS Pediatric Malignancies
- FDG-PET/CT in restaging of patients with recurrent breast cancer: possible impact on staging and therapy
- Predicting Chemotherapy Response to Paclitaxel with 18F-Fluoropaclitaxel and PET
- Monitoring of Early Response to Neoadjuvant Chemotherapy in Stage II and III Breast Cancer by [18F]Fluorodeoxyglucose Positron Emission Tomography
- American Society of Clinical Oncology 2006 Update of the Breast Cancer Follow-Up and Management Guidelines in the Adjuvant Setting
- 18F-FDG PET for Staging Breast Cancer in Patients with Inner-Quadrant Versus Outer-Quadrant Tumors: Comparison with Long-Term Clinical Outcome
- Bone Imaging in Metastatic Breast Cancer
- 18F-FDG PET Evaluation of the Response to Therapy for Lymphoma and for Breast, Lung, and Colorectal Carcinoma