


Abstract
Assessment of reversible defects in exercise 201Tl perfusion SPECT has low sensitivity and high specificity for detection of multivessel coronary artery disease (CAD). The goal of this study was to evaluate whether the left ventricular ejection fraction (LVEF) in exercise 201Tl gated SPECT had incremental diagnostic value over perfusion data for detection of multivessel CAD. Methods: One hundred eighty-two patients underwent exercise 201Tl gated SPECT. Automated LV function analysis software was used for calculation of the postexercise and the rest LVEF. The best threshold between 0- to 1-vessel CAD and 2- to 3-vessel CAD was determined as the cutoff that on receiver-operating-characteristic analysis resulted in the best sensitivity for detection of multivessel CAD with an associated specificity of >90%. Results: Only 18 (26.9%) of 67 patients with multivessel CAD had reversible defects in multiple territories. Sensitivities of the postexercise and the rest LVEF and the worsening of the LVEF by exercise did not differ from those of perfusion data alone. Sensitivities of the combination of perfusion data and the postexercise and rest LVEF did not differ from those of perfusion data alone, whereas the sensitivity of the combination of perfusion data and worsening of the LVEF (i.e., reversible defects in multiple territories or worsening of the LVEF >5.6% [or both]) was significantly greater than that of perfusion data alone (43.3% vs. 26.9%; P < 0.05), with an acceptable level of specificity (90.4%). Conclusion: The worsening of the LVEF by exercise has the potential to detect patients with multivessel CAD among those without multivessel patterns of reversible defects.
Exercise 201Tl myocardial perfusion imaging is a well-established method for diagnosis and risk stratification of patients with coronary artery disease (CAD) (1–4). This diagnosis is based primarily on the identification of perfusion defects. However, a potential limitation of 201Tl scanning is that a measure of relative myocardial blood flow, rather than absolute myocardial blood flow, is obtained. In patients with multivessel CAD, the degree of ischemia may be underestimated because of the relatively balanced global hypoperfusion of the left ventricle (LV) without absolute quantification of regional blood flow. Perfusion defects may be evident only in the most ischemic area, whereas the least ischemic area may appear normal. For this reason, some patients with multivessel CAD exhibit perfusion abnormalities in all of the expected coronary arterial territories on 201Tl imaging. Previous reports (5–7) estimated that as few as 13%–50% of patients with 3-vessel CAD or left main CAD had perfusion abnormalities in multiple territories.
To improve the performance of the scintigraphic methods for detection of multivessel CAD, the use of indirect scintigraphic parameters other than multiple perfusion defects has been reported and validated—that is, increased lung (8,9) or right ventricular (RV) (10) uptake of 201Tl, transient ischemic LV dilatation (8,11), and myocardial 201Tl washout (12). Of these signs, increased lung or RV uptake of 201Tl is an indirect sign of exercise-induced LV dysfunction. Exercise-induced LV dysfunction leads to decreased compliance of the LV, which increases in the LV end-diastolic pressure. The increased LV end-diastolic pressure is transmitted back to the pulmonary capillaries, resulting in leakage of 201Tl into the pulmonary interstitial spaces (13). The increased LV end-diastolic pressure is transmitted back to the pulmonary artery and RV. Wackers et al. (14) showed that an acute increase in RV myocardial blood flow attributed to acute RV strain after pulmonary banding in a canine model resulted in an increased ratio of RV to LV (RV/LV) of 201Tl activity, even before the development of RV hypertrophy.
An automated algorithm (15,16) for direct evaluation of LV function from electrocardiographically (ECG) gated myocardial perfusion SPECT is now commercially available. Recent studies (17–19) using this algorithm showed that in patients with stress-induced perfusion abnormalities, the LV ejection fraction (LVEF) after stress was significantly lower than the LVEF at rest and that the severity of perfusion abnormalities was closely related to the degree of exercise-induced LV dysfunction. Although this automated algorithm has been initially validated using 99mTc-labeled tracers (15,16), recent studies (20–22) have validated the accuracy of 201Tl gated SPECT for measurement of LV function and shown its feasibility and reliability.
The goal of this study was to evaluate whether the LVEF measured by the automated algorithm in exercise ECG gated 201Tl SPECT had incremental diagnostic value over perfusion data for detection of multivessel CAD compared with lung or RV uptake of 201Tl.
MATERIALS AND METHODS
Patient Population
We identified 182 consecutive patients with normal sinus rhythm and known or suspected CAD who underwent exercise 201Tl myocardial SPECT and coronary arteriography in our hospital between January 1999 and July 2000. Patients who had undergone coronary bypass grafting were excluded. Baseline characteristics of the 182 patients are shown in Table 1. Diagnosis of previous myocardial infarction was based on documented elevation of creatine kinase or the presence of the Q-wave on ECG. Thirteen of the 182 patients had significant left main CAD, which was considered equivalent to combined disease of the left anterior descending artery and the left circumflex artery.
Baseline Characteristics of 182 Patients
Exercise 201Tl Myocardial SPECT
Each patient performed symptom-limited exercise on a bicycle. The initial workload was 25 or 50 W and was increased 25 W every 2 min until an endpoint was reached. The endpoints included excessive fatigue, dyspnea, moderate-to-severe angina, hypotension, diagnostic ST depression (>1.5-mm horizontal or downsloping or >2.0-mm upsloping), or significant arrhythmia. At peak exercise, 201Tl (111 MBq for patients without previous myocardial infarction and 74 MBq for patients with previous myocardial infarction) was injected intravenously, and each patient was encouraged to exercise for an additional minute. The postexercise images were obtained immediately after termination of the exercise, and delayed images were obtained 4 h later. In patients with previous myocardial infarction, an additional dose of 37 MBq 201Tl was injected at rest immediately after the acquisition of delayed images, and images after reinjection were obtained 20 min later.
SPECT was performed with a 2-detector gamma camera (Vertex; ADAC Laboratories, Milpitas, CA) equipped with low-energy, general-purpose collimators, with the detectors set to form a 90° angle. Thirty-two equidistant projections were acquired over 180° in a 64 × 64 matrix from the 45° right anterior oblique projection to the 45° left posterior oblique projection. Acquisition of ECG gated images was performed with 40 s per step, in 6° angular steps. At each projection, 8 frames were acquired per cardiac cycle. Nongated images for assessment of 201Tl uptake were obtained by summing all gated images. Transaxial slices of 4.7-mm pixel thickness were reconstructed using a Butterworth filter (order, 5.0; critical frequency, 0.35 cycle per pixel) and the filtered backprojection method (ramp filter) on a processing computer (Pegasys; ADAC Laboratories) with an automatic processing software program for SPECT (Cedars AutoSPECT; Cedars-Sinai Medical Center, Los Angeles, CA) (23). No attenuation correction was applied.
Scintigraphic Image Analysis
Perfusion Defects.
Two experienced observers interpreted the tomographic images visually by consensus. The LV was divided into 9 segments (Fig. 1). 201Tl uptake of each segment was assessed with a 4-point scoring system (3 = normal uptake; 2 = mildly reduced uptake; 1 = moderately reduced uptake; 0 = severely reduced or absent uptake). A reversible defect was defined as ≥1 grade improvement in any segment on the delayed images or reinjection images compared with the postexercise images. The 9 segments were assigned to 3 coronary territories as shown in Figure 1. Reversible defects of LV were classified according to the vascular territories of the 3 major coronary arteries; anterior, septal, and apical defects represented disease in the left anterior descending artery, inferior defects represented disease in the right coronary artery, and lateral defects represented disease in the left circumflex artery. Because of overlap between coronary territories, minimal extension of a perfusion defect into the adjacent territory was considered a perfusion defect of the predominant territory.

Short-axis tomographic segments in relation to coronary arterial territories. Reversible defects in anterior, septal, and apical segments represented disease in left anterior descending artery (LAD), those in inferior segments represented disease in right coronary artery (RCA), and those in lateral segments represented disease in left circumflex artery (LCX).
LVEF.
A completely automated LV function analysis software program (Cedars Quantitative Gated SPECT; Cedars-Sinai Medical Center) (15,16) was used for calculation of the global LVEF. The postexercise LVEF was derived from initial images, and the rest LVEF was derived from delayed images in patients without reinjection images and from reinjection images in patients with reinjection images.
Lung Uptake of 201Tl.
The summed anterior projection image was used for quantification of lung uptake of 201Tl using a ratio of lung to heart (lung/heart). Two regions of interest (ROIs) were drawn: 1 over the entire right lung avoiding the hepatic activity, and 1 over the myocardial wall. The lung/heart was defined as the maximal count in the lung ROI divided by the maximal count in the myocardial ROI (8,9). The postexercise lung/heart was derived from postexercise images, and the rest lung/heart was derived from delayed images.
RV Uptake of 201Tl.
The summed short-axis tomographic images were used for quantification of RV uptake of 201Tl using an RV/LV. ROIs were drawn over the free wall of the RV and LV wall including the interventricular septum on all short-axis images. The RV/LV was defined as the maximal count in the RV ROIs divided by the maximal count in the LV ROIs (10,24). The postexercise RV/LV was derived from postexercise images, and the rest RV/LV was derived from delayed images.
Coronary Arteriography
All patients underwent coronary arteriography within 10 wk (6 ± 13 d) of 201Tl SPECT. Coronary angioplasty was not performed between scintigraphic study and coronary arteriography in any patients. Coronary artery narrowing was assessed visually and reported as the percentage luminal diameter stenosis. Significant coronary stenosis was defined as ≥70% narrowing of the internal diameter of the left anterior descending artery, the left circumflex artery, the right coronary artery, or their major branches and ≥50% narrowing of the left main coronary artery.
Statistics
Values are given as mean ± SD. κ-Statistics were used to evaluate the concordance of diagnosis of the number of diseased vessels with coronary arteriography and 201Tl SPECT perfusion data. One-way ANOVA was used to compare scintigraphic parameters among groups. Posthoc comparisons were performed with by the Tukey test. The best thresholds of lung uptake, RV uptake, and LVEF between 0- to 1-vessel versus 2- to 3-vessel CAD were determined as the cutoff that on receiver-operating-characteristic (ROC) analysis resulted in the best sensitivity for detection of multivessel CAD with an associated specificity of >90%. Incidences of phenomena were compared with the χ2 test. Univariate analysis was performed on scintigraphic criteria to identify potential predictors of multivessel CAD. Univariate variables with P < 0.05 were selected as potentially significant and were entered into a multivariate logistic regression model to identify independent predictors of multivessel CAD. Coefficients of correlation between the rest and exercise LVEF were calculated by linear regression analysis. P < 0.05 was considered significant. These analyses were performed with SPSS version 10.0 software (SPSS, Inc., Chicago, IL).
RESULTS
Scintigraphic Data and Number of Diseased Vessels
Relationships between scintigraphic data and the number of diseased vessels are shown in Table 2. Only 6 (16.2%) of 37 patients with 2-vessel CAD and 3 (10.0%) of 30 patients with 3-vessel CAD had reversible defects in all diseased territories. Only 18 (26.9%) of 67 patients with multivessel CAD had reversible defects in multiple territories.
Relationships Between Scintigraphic Data and Number of Diseased Vessels
The postexercise and rest LVEF were decreased with increasing number of diseased vessels. The magnitude of worsening of the LVEF by exercise rose with increasing number of diseased vessels. The postexercise lung/heart and the postexercise RV/LV and the rest RV/LV increased with number of diseased vessels. The number of diseased vessels had no effect on either the rest lung/heart or the difference between the rest RV/LV and the postexercise RV/LV. The difference between the rest lung/heart and the postexercise lung/heart decreased with number of diseased vessels.
The values of worsening of the LVEF by exercise were 2.1% ± 8.4% (P = 0.04 vs. patients without the left anterior descending artery lesion) in patients with the proximal left anterior descending artery lesion (n = 41), −1.5% ± 8.3% in patients with the distal left anterior descending artery lesion (n = 46), and −1.2% ± 6.2% in patients without the left anterior descending artery lesion (n = 95). The values of worsening of the LVEF by exercise were 3.8% ± 6.6% in patients with multivessel CAD including the proximal left anterior descending artery lesion (n = 24) and −0.3% ± 10.3% in patients with 1-vessel CAD of the proximal left anterior descending artery (n = 17).
Detection of Multivessel CAD with Scintigraphic Parameters
Scintigraphic parameter data for patients with and without multivessel CAD and the best thresholds of scintigraphic parameters for detection of multivessel CAD are shown in Table 3. Neither results of ROC analysis for the rest lung/heart nor the difference between the postexercise RV/LV and the rest RV/LV reached statistical significance. The sensitivities of the other parameters using their best thresholds determined by ROC analysis for detection of multivessel CAD ranged from 22.4% to 29.9% when combined with 90.4% specificities (Table 3).
Scintigraphic Parameter Data for Patients With and Without Multivessel CAD and Best Thresholds of Scintigraphic Parameters for Detection of Multivessel CAD
The diagnostic capabilities of scintigraphic parameters with the best thresholds for detection of multivessel CAD are summarized in Table 4. Sensitivities of the postexercise and the rest LVEF, worsening of the LVEF, the postexercise lung/heart, the difference between the rest lung/heart and the postexercise lung/heart, and the postexercise RV/LV and the rest RV/LV by themselves did not differ from those of perfusion data alone. Sensitivities of the combination of perfusion data and scintigraphic parameters other than worsening of the LVEF did not differ from those of perfusion data alone, whereas the sensitivity of the combination of perfusion data and worsening of the LVEF (i.e., reversible defects in multiple territories or worsening of the LVEF by exercise >5.6% [or both]) was significantly greater than that of perfusion data alone (43.3% vs. 26.9%; P < 0.05). Specificities of all scintigraphic parameters by themselves and in combination with perfusion data were significantly lower than those of perfusion data alone (90.4% vs. 100%; P < 0.001) but remained >90%. No difference was found in sensitivities, specificities, or diagnostic accuracies among these parameters either by themselves or in combination with perfusion data.
Diagnostic Capabilities of Scintigraphic Parameters with Best Thresholds for Detection of Multivessel CAD
The results of univariate and multivariate analysis of prediction of multivessel CAD are shown in Table 5. In scintigraphic parameters evaluated in this study, the number of territories with reversible defects and worsening of the LVEF by exercise were independent predictors of multivessel CAD.
Univariate and Multivariate Analysis of Predictors of Multivessel CAD
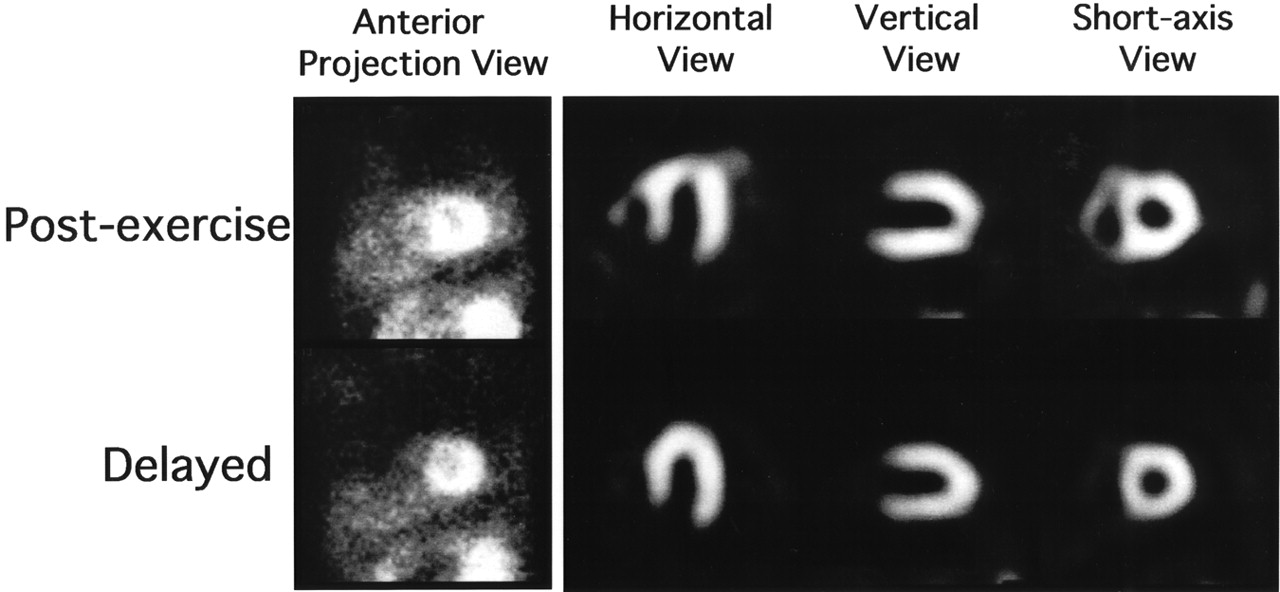
Representative images of a patient with angina pectoris are shown in Figures 2 and 3.

Representative images of anterior projection views and tomograms from 63-y-old male patient with 75% stenosis of left main coronary artery and 75% stenosis of proximal left anterior descending artery. Lung uptake of 201Tl on anterior projection view of postexercise image was markedly increased (lung/heart, 0.57), but that on delayed image was not increased (lung/heart, 0.45). Tomographic images revealed mild reversible defect in apex of LV. RV uptake of 201Tl on postexercise images was markedly increased (RV/LV, 0.66), but that on delayed images was not increased (RV/LV, 0.35).

LV functional images obtained by gated SPECT from same patient as in Figure 2. Outer cage and solid surface represent endocardial surfaces at end diastole and end systole, respectively. LVEF calculated from postexercise images was markedly reduced (LVEF, 40%), but that calculated from delayed images was 60%.
Rest LVEF and Detection of Multivessel Disease by Worsening of LVEF by Exercise
The postexercise LVEF was closely correlated with the rest LVEF (r = 0.84; P < 0.001), whereas worsening of the LVEF by exercise was minimally correlated with the rest LVEF (r = 0.17; P < 0.05). The diagnostic value of a >5.6% worsening of the LVEF by exercise for detection of multivessel CAD is summarized in Table 6.
Diagnostic Value of >5.6% Worsening of LVEF by Exercise for Detection of Multivessel CAD
In patients with a rest LVEF of >50%, the sensitivity of worsening of the LVEF by itself did not differ from that of perfusion data alone (34.1% vs. 17.1%; P = not significant), but the sensitivity of the combination of perfusion data and worsening of the LVEF was significantly greater than that of perfusion data alone (41.5% vs. 17.1%; P < 0.02).Specificities of worsening of the LVEF by itself and in combination with perfusion data were significantly lower than those of perfusion data alone but remained acceptable (87.8%). The diagnostic accuracies of worsening of the LVEF by itself and in combination with perfusion data did not differ from those of perfusion data alone.
In patients with a rest LVEF ≤ 50%, sensitivities, specificities, and diagnostic accuracies of worsening of the LVEF by itself and in combination with perfusion data did not differ from those of perfusion data only.
DISCUSSION
Our results showed that the postexercise and the rest LVEF, and worsening of the LVEF by exercise measured by ECG gated exercise 201Tl SPECT, had diagnostic value for detection of multivessel CAD as well as lung or RV uptake of 201Tl. In particular, the combination of assessment of worsening of the LVEF by exercise and perfusion data in exercise myocardial 201Tl SPECT was more sensitive with acceptable specificity for detection of multivessel CAD than assessment of perfusion data alone. Moreover, worsening of the LVEF by exercise was nearly independent of the rest LVEF and could detect multivessel CAD in patients with a preserved rest LVEF.
Myocardial stunning was initially reported in animal models of coronary occlusion and reperfusion (25). It was shown subsequently that myocardial stunning is also caused by exercise-induced ischemia. The time course of resolution of ischemic LV dysfunction in patients has been reported to range from immediate to 2 h (26–28). An echocardiographic study (26) revealed persistence of regional wall motion abnormalities 30 min after completion of exercise in a high proportion of patients with multivessel CAD. Myocardial uptake of perfusion tracer at the time of acquisition represents the relative myocardial perfusion pattern at the time of tracer injection, whereas the functional data derived from ECG gating represent LV function at the time of acquisition. Acquisition of the initial images in this study required about 15 min after completion of exercise. Accordingly, in some patients with exercise-induced ischemia, LV regional and global function might have already returned to baseline by the completion of the poststress acquisition. In patients with severe coronary artery stenosis, stunning does occur as a consequence of repeated episodes of ischemia during daily life, and repeated episodes of ischemic stunning lead to chronic depression of LV function (29). Therefore, it is possible that in some patients with severe coronary artery stenosis, LV regional and global function is reduced even at rest and that exercise does not induce additional LV dysfunction. Worsening of the LVEF by exercise might correspondingly have relatively low sensitivity in the detection of multivessel CAD.
Because the severity and duration of postischemic functional depression depend on the severity of the ischemia (27,28), recent reports have shown a good relationship between the severity of perfusion abnormalities and exercise-induced LV dysfunction in exercise perfusion scanning (18,19). However, in patients with multivessel CAD, the degree of ischemia may be underestimated because of the relatively balanced global hypoperfusion of the LV without absolute quantification of regional blood flow. In this study, perfusion data revealed reversible defects in multiple territories in only 18 (26.9%) of 67 patients with multivessel CAD, which were comparable to those of previous studies (5–7), whereas worsening of the LVEF by exercise was detected in 11 (22.4%) of 49 patients with reversible defects in at most 1 territory and multivessel CAD.
Multiple studies have shown that the rest LVEF and the postexercise LVEF are powerful predictors of cardiac events and long-term survival of patients with CAD (30,31). The magnitude of worsening of the LVEF by exercise used in this study was nearly independent of LV function at rest and could identify those with multivessel CAD even among patients with a preserved rest LVEF.
Previous studies showed the incremental prognostic value of myocardial perfusion SPECT over clinical and exercise data in predicting cardiac death and nonfatal myocardial infarction (2–4). A significant relationship exists between the extent of perfusion abnormality and cardiovascular mortality, and patients with a normal or mildly abnormal stress SPECT perfusion scan have low cardiovascular mortality (2,3,32,33). However, only some patients with multivessel disease exhibit multivessel patterns of perfusion abnormalities (5–7). Hachamovitch et al. (33) reported that patients with mildly abnormal stress SPECT perfusion scans were at low risk for cardiac death but at intermediate risk for nonfatal myocardial infarction. Patients with multivessel disease have poor prognosis without revascularization and benefit from revascularization in terms of survival (34). Accordingly, it is important to detect patients with multivessel CAD among those with no or mild perfusion abnormalities and to recommend that such patients undergo coronary arteriography and revascularization. As shown in this study, worsening of the LVEF by exercise has the potential to detect patients with multivessel CAD among those without multivessel patterns of reversible defects.
Mazzanti et al. (11) reported that automatic measurement of transient ischemic LV dilatation on stress 99mTc-sestamibi/rest 201Tl dual-isotope nongated SPECT was sensitive and highly specific for detection of severe and extensive CAD (stenosis ≥90% involving either the proximal left anterior descending artery or 2 or 3 coronary arteries). However, in their study, transient ischemic LV dilatation could not detect multivessel CAD with only mild to moderate stenosis, and no incremental diagnostic value of transient ischemic LV dilatation for detection of multivessel CAD over perfusion data was found. In this study, we showed that worsening of the LVEF by exercise was insensitive but had incremental diagnostic value over perfusion data for detection of multivessel CAD.
Johnson et al. (17) reported that in 22 (36%) of 61 patients with reversible perfusion defects, the poststress LVEF was >5% lower than the rest LVEF and that rest to poststress differences in chordal shortening were significantly greater in territories with reversible perfusion defect than in those without reversible defect on stress/rest sestamibi gated SPECT. In their study, the poststress LVEF exhibited no significant correlation with the number of diseased vessels, and no data concerning the relationship between worsening of the LVEF by exercise and the number of diseased vessels were presented.
The postexercise LVEF, the lung/heart, and the RV/LV are all affected by cardiac function at rest (24,35). Because patients with multivessel CAD have a decreased rest LVEF, as shown in this study, these parameters might not be specific markers of exercise-induced LV dysfunction. Measurements of the lung/heart or the RV/LV require manual tracing of ROIs, and patients with proximal right coronary artery lesions or prior RV infarction may not have increased RV uptake, even if they have multivessel CAD (10). On the other hand, worsening of the LVEF by exercise appears to be a specific marker of exercise-induced LV dysfunction and can be obtained completely automatically.
In this study, perfusion defects were interpreted visually. Visual analysis in this study might categorize some mild but significant defects of 201Tl as being normal, resulting in the low sensitivity of perfusion defects for detection of multivessel CAD. Visual analysis of perfusion defects is the most common method in clinical practice, but quantitative analysis of 201Tl distribution was reported to increase the sensitivity of visual analysis for detection of multivessel CAD (12). Moreover, we did not assess transient ischemic LV dilatation, although transient ischemic LV dilatation was also reported to be a sensitive marker for detection of severe and extensive CAD (8,11). These points are the major limitations in this study. To confirm the incremental value of the LVEF for detection of multivessel CAD, further study is necessary to evaluate whether LVEF analysis in exercise 201Tl SPECT had incremental diagnostic value over quantitative analysis of perfusion defects or analysis of transient ischemic LV dilatation for detection of multivessel CAD.
In this study, we evaluated completely or partially reversible defects as a perfusion variable to identify patients with multivessel CAD, but not fixed defects. This might result in the low sensitivity of perfusion data for detection of multivessel CAD. However, many patients in this study had previous myocardial infarctions treated with coronary angioplasty. In other words, many patients had previous myocardial infarctions but no significant stenosis in the infarct-related artery. Accordingly, fixed defects can identify the presence of previous myocardial infarction but cannot identify significant coronary artery stenosis. Because the purpose of this study was to identify significant coronary artery stenosis by evaluating exercise-induced ischemia and exercise-induced LV dysfunction, we did not evaluate fixed defects.
As shown in Table 1, 58% of our patients were treated with β-blockers, resulting in a relatively low peak heart rate. A low peak heart rate and medication with nitrates or calcium-channel blockers (or both) would tend to decrease the sensitivity of all scintigraphic parameters for detection of multivessel CAD. This is one limitation of this study.
The decision to perform coronary arteriography was made by physicians on the basis of SPECT findings or other clinical findings, and patient selection was biased. This study did not determine the prognostic value of perfusion data, the LVEF, or diagnosis with the combination of perfusion data and the LVEF. To confirm the clinical usefulness of worsening of the LVEF by exercise in detection of multivessel CAD, a prospective study with a large population, including evaluation of prognosis, is required.
CONCLUSION
The combination of assessment of worsening of the LVEF by exercise and perfusion data in exercise myocardial 201Tl gated SPECT was more sensitive with acceptable specificity for detection of multivessel CAD than assessment of perfusion data alone. Worsening of the LVEF by exercise has the potential to detect patients with multivessel CAD among those without multivessel patterns of reversible defects.
Footnotes
Received Jul. 23, 2001; revision accepted Oct. 25, 2001.
For correspondence or reprints contact: Hiroyuki Yamagishi, MD, Department of Internal Medicine and Cardiology, Osaka City University Graduate School of Medicine, 1-4-3 Asahi-Machi, Abeno-Ku, Osaka, 545-8585, Japan.
E-mail: yamagishi{at}med.osaka-cu.ac.jp
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Fractional Flow Reserve and Myocardial Perfusion Imaging in Patients With Angiographic Multivessel Coronary Artery Disease
- Nuclear cardiology: myocardial perfusion imaging with SPECT and PET
- Prediction of Death and Nonfatal Myocardial Infarction in High-Risk Patients: A Comparison Between the Duke Treadmill Score, Peak Exercise Radionuclide Angiography, and SPECT Perfusion Imaging
- Effect of Perfusion Pattern and Imaging Sequence on Gated Perfusion SPECT Evaluation of Myocardial Stunning
- The Additive Value of Combined Assessment of Myocardial Perfusion and Ventricular Function Studies
- The Diagnostic and Prognostic Value of ECG-Gated SPECT Myocardial Perfusion Imaging
- Risk stratification using stress myocardial perfusion imaging: don't neglect the value of clinical variables
- Incremental value of combined perfusion and function over perfusion alone by gated SPECT myocardial perfusion imaging for detection of severe three-vessel coronary artery disease