


Abstract
This study was performed to determine differences in 123I image quality at 5 and 24 h for the detection of residual thyroid or recurrent disease in patients with differentiated thyroid cancer and to evaluate which of these approaches provides the optimal yield compared with scans obtained after 131I therapy. Methods: The study included 99 patients (70 women, 29 men). Histopathology included 88 papillary cancers, 7 follicular cancers, and 4 Hürthle cell tumors. Each patient previously had a near-total thyroidectomy. Seventy patients were receiving initial 131I therapy, and 29 had undergone prior radioablative therapy with 131I. Whole-body images and spot views of the neck and chest were obtained with a dual-head scanner at 5 and 24 h after the oral administration of 56 MBq (1.5 mCi) Na123I. In addition, tomographic images of the neck and chest were obtained in 26 patients. The images obtained at 5 and 24 h were evaluated for the number of lesions visualized and the image quality. Seventy-four patients received radioablative therapy after this diagnostic work-up. Whole-body images were obtained on these patients 7 d after 131I therapy and were compared with the diagnostic scans. Results: Overall, images acquired 5 and 24 h after oral administration of 56 MBq (1.5 mCi) 123I were concordant in 73% of patients. For 25 patients (25%), 24-h scanning was superior by detecting additional neck foci or confirming equivocal neck foci (20 patients) and confirming equivocal pulmonary uptake (5 patients). In the subset of patients undergoing surveillance imaging after prior 131I ablation therapy with positive scans, 24-h images were superior in 66%. In 3 patients, SPECT revealed additional foci compared with planar images at 5 h. These foci were also clearly identified on the planar images obtained at 24 h. Images obtained after therapy did not identify additional sites of tumor involvement compared with those noted on 24-h images but did reveal more foci of residual thyroid tissue in 5 patients. Conclusion: The diagnostic yield of planar diagnostic 123I scintigraphy at 24 h was superior to that at 5 h for lesion detection and image quality, and images obtained after 131I therapy did not reveal unknown metastatic foci.
Diagnostic radioiodine scanning is routinely used for most patients with differentiated thyroid cancer (DTC), either before thyroid remnant ablation or as surveillance for cancer recurrence (1). Whereas 131I is the ideal radionuclide for ablating residual thyroid tissue or recurrent DTC (or both), it is suboptimal for diagnostic purposes. The disadvantages of using 131I as a diagnostic agent in the management of DTC include poor image quality because of its physical characteristics (γ-photopeak of 364 keV) and possible stunning of functioning thyroid cells associated with its β-emission, which decreases the impact of the therapeutic doses of 131I administered after a diagnostic dose of this radionuclide (2,3). In patients with DTC who are undergoing remnant ablation, we have shown that whole-body images obtained 5 h after the oral administration of 56 MBq (1.5 mCi) 123I are superior to those obtained at 48 h after the oral administration of 111 MBq (3 mCi) 131I (4). Subsequently, we have routinely used 123I scintigraphy to detect functioning thyroid tissue and metastases in patients with a history of DTC.
This study was performed to optimize the 123I imaging protocol by comparing images acquired at 5 and 24 h after the administration of 56 MBq (1.5 mCi) 123I in patients with DTC, either before thyroid remnant ablation or for surveillance of residual or recurrent cancer. In addition, diagnostic 123I images were compared with scans obtained 7 d after 131I therapy in patients who were considered candidates for such interventions.
MATERIALS AND METHODS
Patients
We retrospectively evaluated the 123I whole-body scans that were obtained on 99 consecutive patients with DTC (70 women, 29 men; mean age, 46 y; age range, 17–79 y). The histopathologic results revealed 88 papillary cancers, 7 follicular cancers, and 4 Hürthle cell cancers. Each patient had undergone a near-total thyroidectomy before imaging. Seventy patients were scanned before thyroid remnant ablation (group I). Twenty-nine patients had received prior radioablative 131I therapy and were being studied for thyroid cancer recurrence (group II).
Scintigraphy
Thyroid hormone replacement was withheld for 2 wk (triiodothyronine) to 4 wk (levothyroxine) before the scintigraphic study, and a low-iodine diet was followed for 1 wk before scintigraphy. All patients had serum levels of thyroid-stimulating hormone of >40 mU/L at the time of scanning.
The patients received 56 MBq (1.5 mCi) Na123I orally on the morning of the examination. Five hours later, planar whole-body and dedicated neck and chest images were obtained in anterior and posterior projections using a low-energy collimator on a dual-head gamma camera. Tomographic images (SPECT) of the neck and chest were also obtained if deemed necessary. The patients were reimaged at 24 h. As with 5-h studies, a whole-body scan and spot views of the neck and chest were obtained in anterior and posterior projections. Patients with foci of functioning tissue or metastases received therapeutic doses of 131I (3,700–7,400 MBq [100–200 mCi]) within the next 24 h. One week after therapy with 131I, planar whole-body images and spot views of the neck and chest were obtained in anterior and posterior projections using a medium-energy collimator on a dual-head gamma camera.
All images were reviewed by 2 nuclear medicine physicians and 1 endocrinologist. Qualitative evaluation of the number and location of foci and the image quality at 5 and 24 h was performed. In addition, in a representative sample (n = 20), a quantitative evaluation was performed by comparing the ratio of counts in the tumor to counts in the background using identical regions of interest on the 5- and 24-h images. Also, the 5- and 24-h 123I images were compared with those obtained after 131I ablative therapy.
RESULTS
Group I
Seventy of the scans were obtained on patients who had undergone near-total thyroidectomy before radioablative therapy with 131I (group I). Two patients had diagnostic 123I scans with negative findings and were not treated with 131I; 68 patients had diagnostic scans with positive findings. As expected, most lesions in group I patients were in the thyroid bed and the neck. Additional sites of uptake included pulmonary metastases (4 patients), femoral metastasis (1 patient), and mediastinal involvement (5 patients). In 68 patients in group I, the diagnostic scans with positive findings showed 150 foci of functioning thyroid tissue or metastases at 5 h and 166 foci at 24 h. Two patients each had 1 lesion that was better visualized on 5-h scans. These included a focus in the thyroid fossa that was count poor at 24 h because of technical reasons and a mediastinal focus that was present at 5 h but was absent at 24 h and most likely represented esophageal activity (Fig. 1). Eleven patients had a total of 17 additional thyroid bed foci that were visualized at 24 h but not at 5 h. In addition, 7 patients had 24-h images that clearly delineated 15 thyroid bed foci that were equivocal on 5-h images (Fig. 2). On the basis of the findings of the 5-h planar images, SPECT was performed on 26 patients, which revealed additional pulmonary or mediastinal foci in 3 patients. However, these foci were also clearly identified on planar images obtained at 24 h (Fig. 3). Overall, in group I, 47 patients (67%) had concordant scans at 5 and 24 h and 21 patients (30%) had 24-h images that were superior to 5-h images.

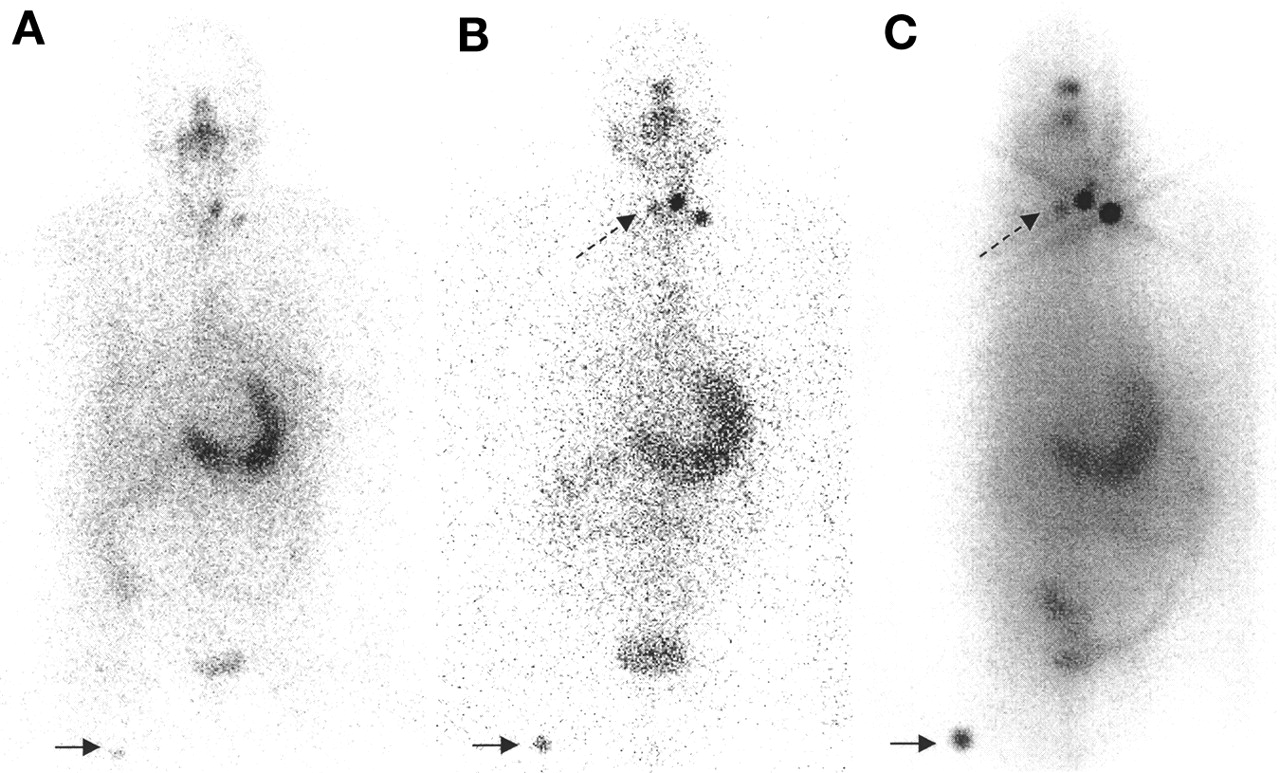
Planar images obtained 5 h after 123I administration and before 131I therapy for thyroid remnant ablation. Mediastinal focus (arrow) detected on 5-h image (A) is not present on 24-h scan (B) or on scans after 131I therapy (not shown). Finding most likely represents focal retention of saliva 123I in esophagus.
Planar images obtained 5 h (A) and 24 h (B) after 123I administration and 7 d after 131I therapy (C) in patient who was referred for thyroid remnant ablation. Right thyroid bed focus (dashed arrow) is not seen on 5-h image but is clearly present on 24-h image. Other foci of tracer activity in thyroid bed (left lower neck) and in right femur region (solid arrow) are better defined on 24-h image. Findings on 24-h image are confirmed by scan obtained 7 d after 131I therapy.
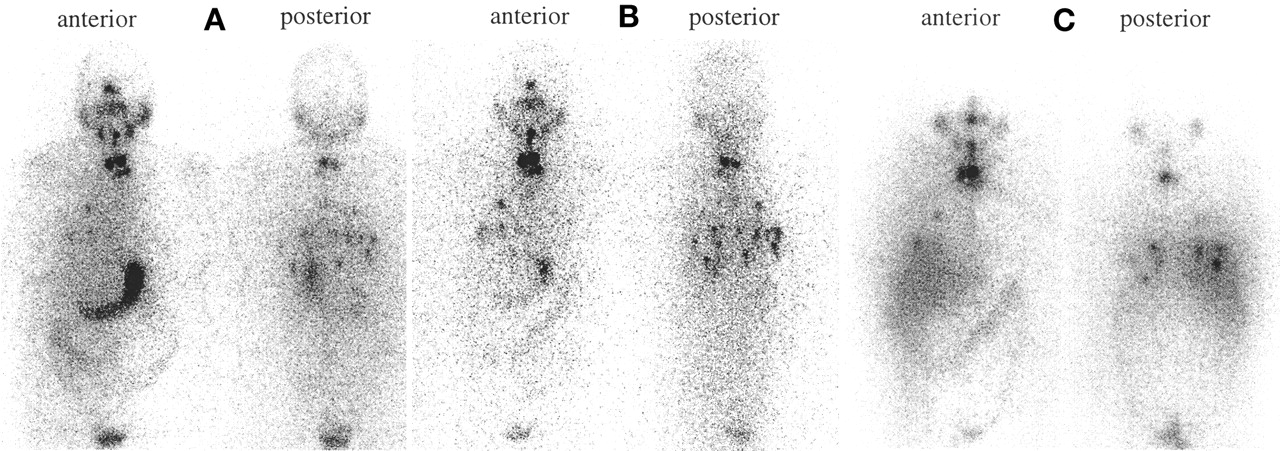
Planar images acquired 5 h (A) and 24 h (B) after 123I administration and 7 d after 131I therapy (C) in patient with known pulmonary metastases who was scheduled to undergo thyroid remnant ablation. Five-hour and 24-h scans reveal bilateral pulmonary metastases (more clearly defined on posterior views than on anterior views), which appear more extensive and distinct on 24-h images than on 5-h images. Findings are confirmed by scan obtained 7 d after 131I therapy.
On 68 patients who were treated with 131I for either thyroid remnant ablation alone or remnant ablation in the presence of distant metastases, images obtained 1 wk after 131I therapy did not identify additional sites of tumor metastases compared with the 123I images acquired at 24 h. In 5 patients (7%), 1 or 2 additional foci were seen in the thyroid bed on the scans obtained after therapy, but this finding did not alter clinical management.
Group II
Surveillance imaging was performed on 29 patients with DTC who had undergone prior near-total thyroidectomy and radioablative therapy with 131I. Scintigraphic findings were negative on 23 patients (79%) at 5 and 24 h. The remaining 6 patients in group II had 123I scans with positive findings that revealed a total of 4 foci in the thyroid bed at 5 h, 6 foci at 24 h, and diffuse pulmonary uptake in 2 patients that was present at 5 and 24 h. The 5- and 24-h scans detected an equivalent number of lesions of the thyroid fossa in 2 patients. However, the 24-h scan revealed 2 additional foci in the thyroid fossa that were not detected at 5 h in a third patient and confirmed a thyroid bed focus that was equivocal at 5 h in a fourth patient. Bilateral pulmonary metastases in 2 patients with papillary cancer were found on the 5- and 24-h images but were more distinct at 24 h (Fig. 4). Thus, 24-h images were superior to 5-h images in 4 of the 6 patients (66%) with positive surveillance scans. These 6 patients were treated with 131I, and no additional sites of metastasis or residual thyroid tissue were visualized on the scans acquired 1 wk later. None of the 23 patients with negative diagnostic 123I scans had an elevated serum thyroglobulin level, and 131I therapy was not administered.

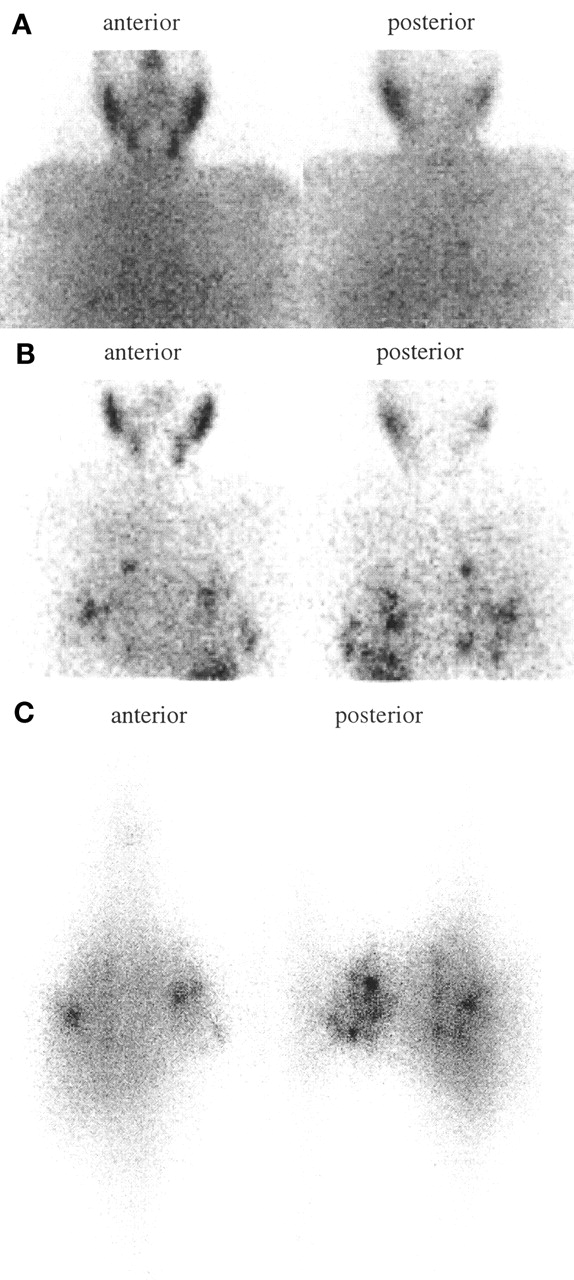
Planar images obtained 5 h (A) and 24 h (B) after 123I administration and 7 d after 131I therapy (C) in patient with known pulmonary metastases 1 y after initial thyroid remnant ablation. Foci of uptake in lungs are faint on 5-h image but are clearly defined on 24-h image and are further confirmed by scan obtained 7 d after 131I therapy.
In groups I and II, all lesions detected on the 123I scans at 24 h were confirmed on imaging after therapy; therefore, there was no evidence of stunning. In addition, a visual comparison of scans found that 24-h images were qualitatively better at delineating lesions than 5-h images. In a representative sample of 20 patients (from groups I and II), tumor-to-background ratios were quantified at 5 and 24 h using identical regions of interest. The ratio of mean tumor- to-background counts between 24 and 5 h in these 20 studies was 2.8:1 with an SD of 1.4.
DISCUSSION
Our results show that diagnostic imaging with 56 MBq (1.5 mCi) 123I is sensitive for the detection of residual thyroid tissue or metastatic thyroid cancer in patients with DTC who are undergoing preablation or surveillance scanning. Overall, images acquired 5 and 24 h after oral administration of 56 MBq (1.5 mCi) 123I were concordant in 73% of patients. For 25 patients (25%), 24-h scanning was superior by detecting additional neck foci or confirming equivocal neck foci (20 patients) and confirming equivocal pulmonary uptake (5 patients). In the subset of 6 patients undergoing surveillance imaging after prior 131I ablation therapy with positive scans, 24-h images were superior in 66%. Therefore, acquisition of images at 24 h is preferable for surveillance patients.
This study provides the largest and most comprehensive systematic comparison of diagnostic 123I whole-body imaging with scanning after therapy during initial ablation and subsequent surveillance and treatment of metastatic disease. Several other studies have evaluated 123I as a diagnostic agent in patients undergoing scanning before initial 131I ablative therapy. However, 2 groups used only low doses of 123I (10–20 MBq [270–540 μCi]) with the aim of detecting remnant functioning thyroid tissue, which is not ideal for performing whole-body scanning to detect metastatic disease (5,6). A third group used a larger dose of 30–37 MBq (0.8–1.0 mCi) 123I to perform whole-body imaging, but they reported only 13 patients who had just undergone surgery. At this time, only 1 patient had metastatic disease, which was in the lung, and this 123I scan was reported to have a lower uptake intensity than the scan obtained after therapy (7). In our study, metastatic pulmonary disease was present in 4 of the patients undergoing initial 131I therapy. In these patients, the 123I images acquired at 24 h were equal to the scans obtained after therapy, which may reflect the larger 123I dose (56 MBq [1.5 mCi]) used in our study.
On the other hand, 2 small studies have administered even larger doses of 123I (370–1,000 MBq [10–27 mCi]) for diagnostic imaging than we used (8,9). Compared with imaging after therapy, their findings were similar to ours, so that that there does not appear to be an incremental sensitivity in scanning with these large doses. Four-hour images were found to have higher background activity, and 48-h scans did not detect additional lesions compared with 24-h images (9). These data support our findings and our recommendation that imaging at 24 h may be optimal.
Although our study shows excellent concordance between diagnostic 123I images and scans after therapy, we did not compare diagnostic imaging between the 2 isotopes, 123I versus 131I. However, our diagnostic images acquired at 24 h were concordant with scans obtained 7 d after 131I therapy in 93% of patients and only showed additional foci within the thyroid bed in the other 5 patients, which did not alter clinical management. Our findings suggest that 123I may be superior to 131I as a diagnostic agent because published reports comparing diagnostic 131I imaging with scans obtained after therapy have shown discordance in up to 24% of patients, with new locations of metastases revealed in 10% (10,11). Most important, in our study, no new sites of metastases were seen on scanning after therapy compared with diagnostic imaging.
CONCLUSION
Diagnostic scanning with 56 MBq (1.5 mCi) 123I at 24 h is sensitive for detecting residual thyroid tissue and distant metastases in patients with DTC, even in the presence of a thyroid remnant. For patients undergoing initial ablation therapy, imaging of the neck and chest at 4 h may enhance patient convenience so that a therapeutic 131I dose can be ordered the next day; 24-h whole-body images should still be obtained because of their superior image quality. For patients undergoing surveillance imaging, a 24-h scan is best. All patients must be encouraged to swallow water before imaging to reduce the possibility of esophageal activity. With only a modest increase in radioisotope cost, the use of 123I minimizes the radiation dose to the thyroid remnant and functioning metastases, which may optimize the success of subsequent 131I therapy, and provides high-quality images for lesion detection.
Footnotes
Received Mar. 16, 2001; revision accepted Jun. 12, 2001.
For correspondence or reprints contact: Susan J. Mandel, MD, MPH, Endocrinology, Hospital of the University of Pennsylvania, 1 Maloney/3400 Spruce St., Philadelphia, PA 19104.
E-mail: smandel{at}mail.med.upenn.edu




{kind=link}
{kind=link}
{kind=link}
{kind=link}