


Abstract
Among patients with resected non–small cell lung cancer (NSCLC), approximately 50% present with a recurrent tumor. The clinical or pathologic TNM staging does not always provide a satisfactory explanation for differences in relapse and survival. Thus, it is of major importance to be able to predict these relapses and to prevent them with an active chemotherapy or radiotherapy program (or both). 18F-FDG uptake on PET could be of prognostic significance in patients with resected NSCLC. The goal of this study was to determine whether the level of metabolic activity observed with 18F-FDG uptake correlates with the probability of postoperative recurrence in patients with NSCLC. Methods: Fifty-seven patients with NSCLC were examined with 18F-FDG PET. For semiquantitative analysis, standardized uptake values (SUVs) were calculated. Patients were classified into high-SUV (>5.0) and low-SUV (≤5.0) groups. All patients underwent thoracotomy within 4 wk after the 18F-FDG PET study. Tumor 18F-FDG uptake (SUV), pathologic stage, and lesion size were analyzed for their possible association with disease-free survival. Results: Forty-six patients had pathologic stage I NSCLC and 11 had pathologic stage II or stage III NSCLC. In a univariate analysis, patients with an SUV of ≤5 had a much better disease-free survival than did patients with an SUV of >5 (P < 0.0001). In patients with pathologic stage I and stage IA NSCLC, the SUV was also correlated with disease-free survival (P < 0.0001 and P = 0.0012, respectively). Patients with pathologic stage I disease had an expected 5-y disease-free survival rate of 88% if the SUV was ≤5 and a survival rate of ≤17% if the SUV was >5. A multivariate Cox analysis identified the SUV as the most significant independent factor for disease-free survival. Conclusion: We conclude that the 18F-FDG uptake in primary NSCLC determined by PET has a significant independent postoperative prognostic value for recurrence, especially in patients with pathologic stage I NSCLC. 18F-FDG uptake was superior to pathologic stage in predicting relapse of patients with NSCLC.
The tumor-node-metastasis (TNM) staging system is the most important tool used by clinical oncologists to estimate prognosis (1) and to choose the best combination of treatment modalities such as surgery, radiation therapy, and chemotherapy. However, the clinical or pathologic TNM staging does not always provide a satisfactory explanation for differences in relapse and survival. Resected stage I non–small cell lung cancer (NSCLC) is a typical example. Many patients are cured, but some suffer an early relapse and die. Approximately 50% of patients with resected NSCLC present with a recurrent tumor (2). Approximately 35% of stage I patients who undergo resection relapse, resulting in a 5-y survival rate of approximately 65% (3). Thus, it is of major importance to be able to predict these relapses and to prevent them with an active chemotherapy or radiotherapy program (or both).
Recent advances in molecular biology have helped to elucidate different patterns of relapse and survival in resected stage I NSCLC. For instance, measures of tumor proliferation estimated by proliferating cell nuclear antigen (PCNA) and Ki-67 expression have prognostic value for recurrence and survival in resected NSCLC (4,5). NSCLC is also characterized by glucose metabolic derangements. Increased glycolysis results in the upregulation of glucose transporter protein (especially subtype Glut-1) and in increased hexokinase activity (6). These glucose metabolic derangements can be measured quantitatively in vivo by PET after administration of 18F-FDG. Recently, the 18F-FDG uptake in NSCLC has been correlated with the growth rate and proliferation capacity of tumors (7–9) and has also been identified as an independent prognostic factor correlated with tumor aggressiveness and survival in patients with lung cancer (10–13). The more metabolically active the tumor, the worse the outcome.
On the basis of these findings, we analyzed recurrence in patients with resected NSCLC. The aim of this study was to evaluate whether the standardized uptake value (SUV), a semiquantitative measurement of 18F-FDG uptake in the tumor, was predictive of the prognosis for recurrence in patients with surgically resected NSCLC.
MATERIALS AND METHODS
Patients
Fifty-seven patients with NSCLC were included in this retrospective study. The study group included patients with NSCLC who underwent 18F-FDG PET between February 1994 and November 2000, then underwent resection of the tumor, and then were monitored bimonthly at the outpatient clinic after surgery. Excluded were patients who showed evidence of distal metastatic disease before surgery, who received postoperative chemotherapy or radiation therapy, or who had insulin-dependent diabetes and serum glucose levels of >120 mg/dL just before the 18F-FDG was injected. Not all eligible patients underwent 18F-FDG PET because of limitations of scheduling and patient consent. Patient characteristics recorded at baseline included age, sex, tumor cell type (adenocarcinoma, squamous cell carcinoma, adenosquamous cell carcinoma, or large cell carcinoma), cell differentiation (poorly, moderately, or well differentiated), lesion size (maximal tumor diameter as determined by pathologic findings), and pathologic stage (according to the TNM staging system). Informed consent was obtained from patients for the 18F-FDG PET study.
18F-FDG PET
Thoracic PET was performed using a dedicated PET camera (Headtome IV; Shimazu, Kyoto, Japan) with 4 rings, which provided 7 tomographic slices. The intrinsic resolution was 5-mm full width at half maximum at the center. After at least 4 h of fasting, each subject underwent transmission scanning for attenuation correction for 10 min. Immediately after obtaining the transmission scan, 18F-FDG was administered intravenously, and a static scan (14–24 tomographic slices at 6.5-mm intervals) was obtained 40 min later for 10–20 min using a 128 × 128 matrix. The average injection dose of 18F-FDG was 185 MBq.
Data Analysis
The 18F-FDG images were visually interpreted from the films and carefully correlated with a contemporaneous CT study. For semiquantitative analysis of the 18F-FDG uptake, irregular regions of interest (ROIs) were placed over the most intense area of 18F-FDG accumulation. To place ROIs on the lesion, a modified method, based on the original report of Ahuja et al. (12), was used. The ROIs placed on the lesions encompassed all pixels within that lesion with uptake values of >90% of the maximum uptake in that slice, and the average counted rate in each ROI was calculated. After correction for radioactive decay, the ROIs were analyzed by computing the SUV (tumor activity concentration/injected dose/body weight), which was calculated using a calibration factor between PET counts and radioactivity concentration.
Statistical Analysis
Disease-free survival time was defined as the time interval from the date of 18F-FDG PET until recurrence or the last follow-up date. Survival time was defined as the time interval from the date of 18F-FDG PET until death or the last follow-up date. Survival and disease-free survival were calculated with the Kaplan–Meier method, and groups were compared using the log-rank test.
Multivariate analysis was performed with the Cox proportional hazards model to assess the joint effects and interactions of the following variables on disease-free survival: SUV, pathologic stage, and lesion size. A log-rank test and a generalized Wilcoxon test were used to determine a statistically significant SUV cutoff value, which was used for survival and disease-free survival analyses.
RESULTS
The characteristics of the 57 patients are listed in Table 1. The SUV was 3.6 ± 2.3 (mean ± SD) and ranged from 0.38 to 9.74. Forty-six patients had pathologic stage I NSCLC, including 38 with stage IA (T1 N0 M0) and 8 with stage IB (T2 N0 M0) NSCLC. Eleven patients had pathologic stage II or stage III NSCLC. The lesion size, which was determined from the resected specimens, was 2.6 ± 1.1 cm (mean ± SD) and ranged from 0.8 to 6.3 cm. Fifteen (26.3%) of the lung cancers were >3 cm in diameter. Of the remaining 42 lung cancers, 20 (35.1%) were 2.1–3.0 cm and 22 (38.6%) were ≤2 cm. The histologic types were 47 adenocarcinomas, including 13 bronchioloalveolar carcinomas, 8 squamous cell carcinomas, 1 adenosquamous cell carcinoma, and 1 large cell carcinoma. Seventeen (29.8%) of the 57 patients suffered a recurrence during follow-up at a median time of 14 mo after the PET study, and 11 of these patients died during follow-up at a median time of 19 mo after the PET study. Forty patients did not suffer a recurrence at the time of data analysis. Follow-up for these patients was available for a median period of 33.5 mo after the PET study.
Characteristics and Radionuclide Imaging Results of 57 Patients
Univariate Survival Analysis
The influence of tumor 18F-FDG uptake was explored for various SUV cutoff values. The most discriminate cutoff point for prognosis proved to be at an SUV of 5, although dichotomization with a broad range of SUVs, between 4 and 7, gave significantly discriminative log-rank probability values and generalized Wilcoxon probability values. Patients with an SUV of ≤5 had a significantly better survival rate than patients with an SUV of >5 (P = 0.0002) (Fig. 1A). In 44 patients with lung cancer other than bronchioloalveolar carcinoma, those with an SUV of ≤5 had a significantly better survival rate than patients with an SUV of >5 (P = 0.0028).
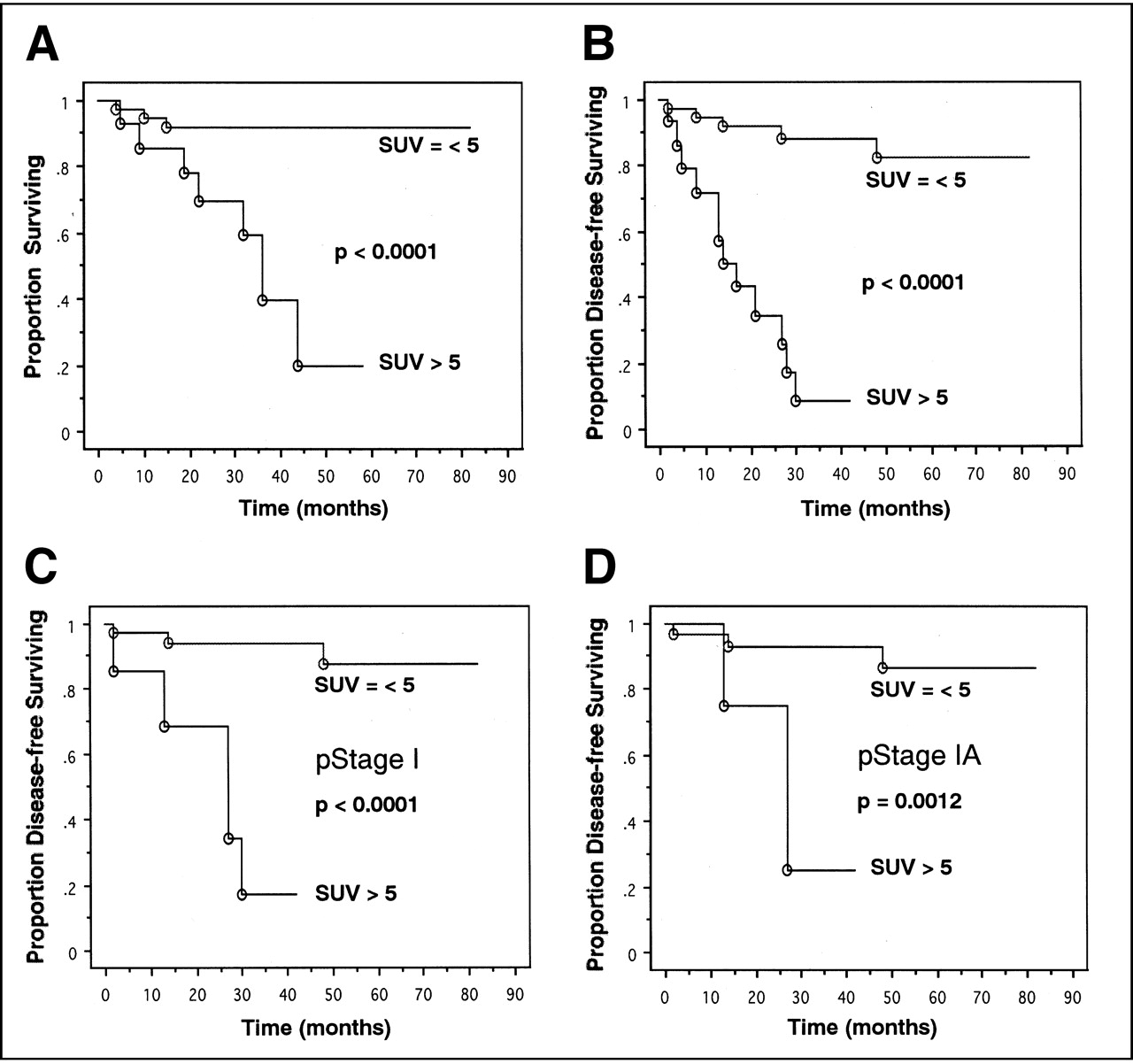
(A) Kaplan–Meier survival curves of all 57 patients according to SUV of lung cancer. (B) Kaplan–Meier disease-free survival curves of all 57 patients according to SUV of lung cancer. (C and D) Kaplan–Meier disease-free survival curves of 46 patients with pathologic stage (pStage) I NSCLC (C) and 38 patients with pStage IA NSCLC (D) according to SUV of lung cancer. Curves reveal clear demarcation, with poor survival or disease-free survival of subjects in high-SUV group.
Univariate Disease-Free Survival Analysis
The influence of tumor 18F-FDG uptake was explored for various SUV cutoff values, and the most discriminative cutoff point was again found to be an SUV of 5. Patients with an SUV of ≤5 also had a significantly better disease-free survival rate than patients with an SUV of >5 (P < 0.0001) (Fig. 1B). In patients with pathologic stage I (Fig. 1C) and stage IA (Fig. 1D) NSCLCs, the SUV was also correlated with disease-free survival (P < 0.0001 and P = 0.0012, respectively). Images from representative patients (patients 35 and 37) are shown in Figures 2 and 3. Patients with pathologic stage I NSCLC had an expected 5-y disease-free survival rate of 88% if the SUV was ≤5 and a survival rate of ≤17% if the SUV was >5. In 44 patients with lung cancer other than bronchioloalveolar carcinoma, those with an SUV of ≤5 also had a significantly better disease-free survival rate than patients with an SUV of >5 (P < 0.0001). In patients with pathologic stage I and stage IA lung cancers other than bronchioloalveolar carcinoma, the SUV was also correlated with disease-free survival (P = 0.0004 and P = 0.0124, respectively).
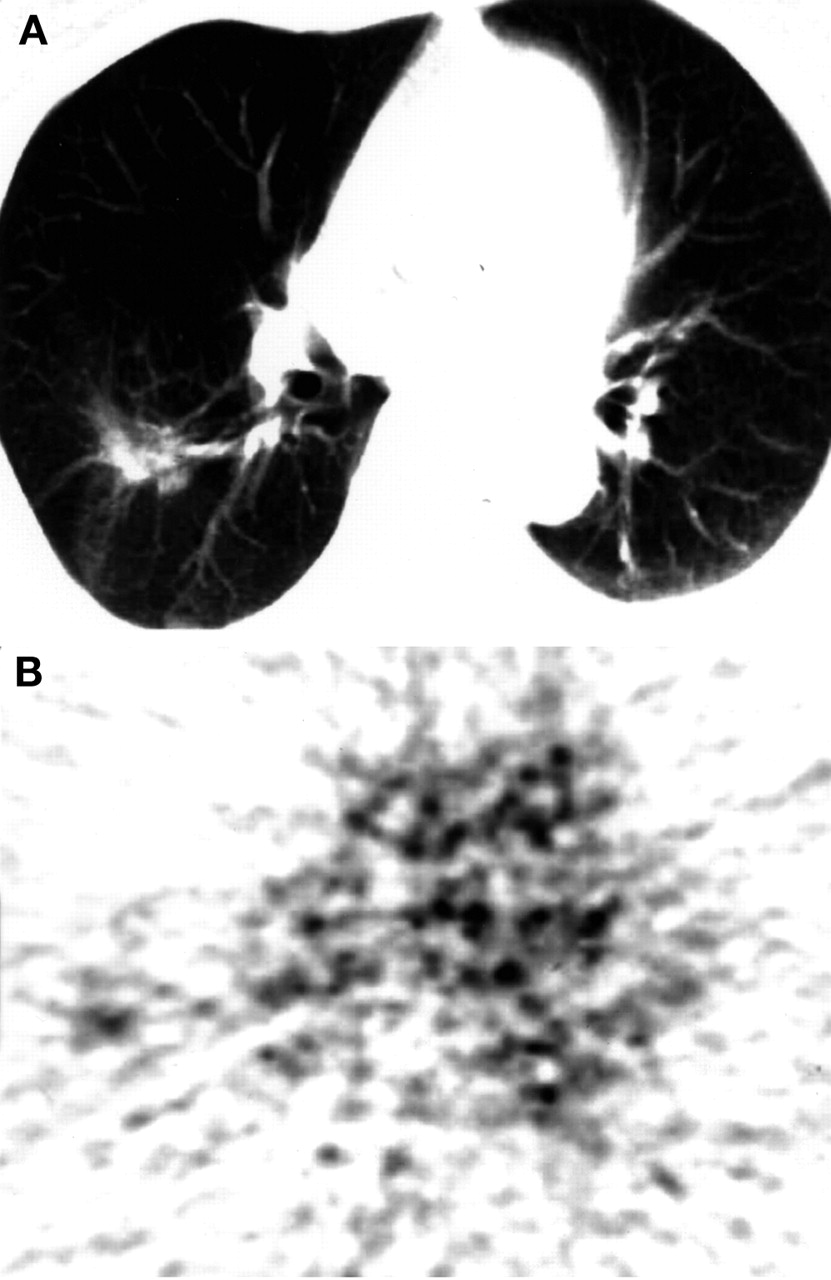
Patient 37: moderately differentiated adenocarcinoma, 3.5 cm in maximal diameter, pathologic stage IB (T2 N0 M0). (A) CT image shows nodule in right lung. (B) 18F-FDG PET shows faint accumulation in tumor (SUV, 2.12). Patient was alive 53 mo after PET study.

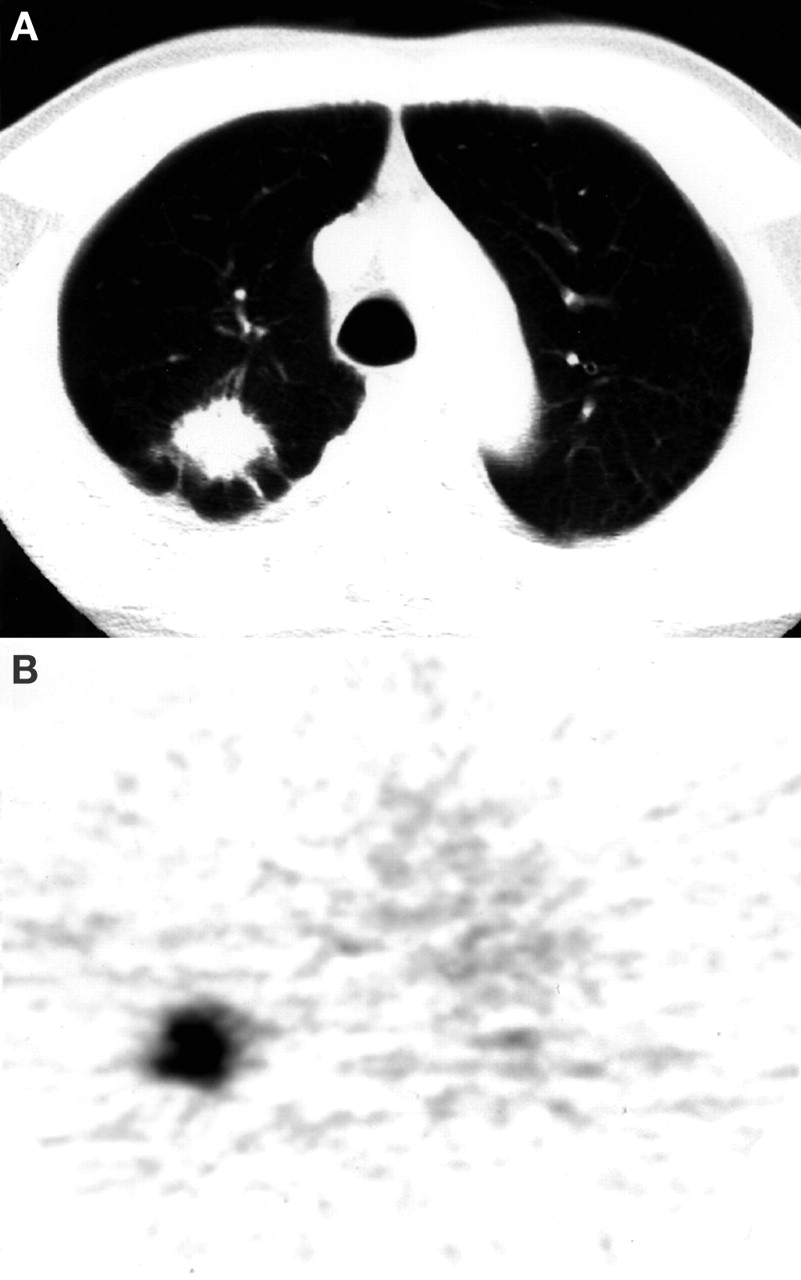
Patient 35: moderately differentiated adenocarcinoma, 2.9 cm in maximal diameter, pathologic stage IA (T1 N0 M0). (A) CT image shows nodule in right lung. (B) 18F-FDG PET shows hot accumulation in tumor (SUV, 5.76). Patient suffered recurrence in brain 27 mo after PET study and died 32 mo after PET study.
Multivariate Disease-Free Survival Analysis
The joint effects and interactions of the SUV, pathologic stage, and lesion size were examined to determine whether the SUV had prognostic importance for recurrence beyond that provided by the pathologic stage and lesion size. The categoric variable (pathologic stage I vs. stages II and III) and the numeric variables (SUV <5 vs. >5 and tumor diameter <3 vs. >3 cm) were dichotomized. A multivariate Cox analysis identified the SUV as the most significant independent factor for disease-free survival (Table 2). In 44 patients with lung cancer other than bronchioloalveolar carcinoma, a multivariate Cox analysis again identified the SUV as the most significant independent factor for disease-free survival.
Cox Proportional Hazards Model (Using Dichotomized Variables)
DISCUSSION
The principal finding of this study is that 18F-FDG uptake in primary NSCLC patients determined by PET has a significant independent postoperative prognostic value for recurrence, especially in patients with pathologic stage I NSCLC: The greater the 18F-FDG uptake in lung cancer, the higher the incidence of metastasis. 18F-FDG uptake was superior to pathologic stage in predicting relapse of patients with NSCLC.
In this study, approximately 30% of patients with resected NSCLC presented with a tumor recurrence. Approximately 17% of stage I patients who underwent resection suffered a relapse. The ability to predict recurrence is an important contribution to treatment planning. If postoperative prognosis can be determined before surgery, it will be possible to determine indications for intensive preoperative and postoperative treatment, including radiotherapy and chemotherapy. Thus, 18F-FDG PET appears to be useful in determining the optimal therapeutic policy and in contributing to improvement of the postoperative prognosis.
Although the pathologic stage is the most important prognostic factor to date (1), it provides an incomplete biologic profile of NSCLC. Measures of tumor proliferation estimated by PCNA and Ki-67 expression have prognostic value in patients with resected NSCLC (4,5). Increased PCNA and Ki-67 expression have been found to predict poor outcome (4,5) and to be associated with the development of metastases (14). A better understanding of the molecular biology of NSCLC has recently led to the identification of factors that could explain the more aggressive behavior of some tumors. A further molecular–biologic derangement found in NSCLC is altered glucose metabolism, resulting primarily from increased glycolysis and upregulation of glucose transporter proteins (especially Glut-1) and increased hexokinase activity (6). The 18F-FDG uptake in NSCLC has been correlated with tumor growth rate and proliferation capacity (7–9): The greater the 18F-FDG uptake, the higher the proliferation capacity. The 18F-FDG uptake in NSCLC has also been correlated with aggressiveness (pleural involvement, vascular invasion, and lymphatic permeation), as determined by pathology in adenocarcinoma of the lung (10): The greater the 18F-FDG uptake, the more aggressive the tumor. Aggressiveness, especially vascular invasion, is an important determinant of recurrence in stage I NSCLC (14,15). Furthermore, overexpression of the Glut-1 transporter, an important feature of glucose disturbance in NSCLC (16), has also been linked to a poorer prognosis (17,18). All of these findings could explain the relationship between 18F-FDG uptake on PET and biologic aggressiveness, and thus prognosis, in NSCLC.
18F-FDG uptake has been identified recently as a significant prognostic factor correlated with survival in patients with lung cancer (10–13): The more metabolically active the tumor, the worse the outcome. Dhital et al. (11) reported that an SUV of ≥20 was of significant prognostic value in 77 patients with primary lung cancer. Ahuja et al. (12) reported that an SUV of >10 was of significant adverse prognostic importance in 155 patients with NSCLC. In these studies, not only the surgical group but also the radiation or chemotherapy group (or both) were included. Vansteenkiste et al. (13) reported that for the SUV a group dichotomy with a cutoff SUV value of 7 had the best discriminative value for prognosis in the total 125 patients with NSCLC and in the surgical cohort. In our study, because the selection of treatment regimen was also a significant prognostic factor, only surgically resected patients were included, and the most discriminative cutoff point was found at an SUV of 5, a lower value than those found in other studies. There are several possible explanations for this phenomenon. First, our study included only surgically resected patients, and 46 (80.7%) of the 57 patients had pathologic stage I lung cancers. Second, the tumor size (mean ± SD) was small (2.60 ± 1.67 cm), and 38.6% of the total lung cancers were ≤2 cm in size. 18F-FDG uptake values determined by PET are subject to partial-volume effects, which lead to an underestimation of the real value (19). Finally, depending on the type of neoplasm, wide individual variations in glucose consumption can be observed. The uptake of 18F-FDG by adenocarcinomas has been shown to correlate with their degree of cell differentiation (20). In particular, the 18F-FDG uptake in bronchioloalveolar carcinomas was significantly lower than that in nonbronchioloalveolar adenocarcinomas (7,20). In our study, the SUV (mean ± SD) of all lung cancers was low (3.6 ± 2.3). This finding can be attributed to the fact that our study included many bronchioloalveolar carcinomas and well-differentiated adenocarcinomas, which have low SUV values.
Our study has certain limitations. First, dichotomization with a broad range of SUVs, between 4 and 7, gave significantly discriminative log-rank probability values and generalized Wilcoxon probability values, although the most discriminate cutoff point for prognosis proved to be at an SUV of 5. Vansteenkiste et al. (13) also reported that dichotomization with a broad range of SUVs gave significantly discriminative log-rank probability values (<0.05). It seems reasonable to hypothesize that there is no true cutoff point but, rather, a transition zone, within which the prognosis gradually worsens (13).
Second, because of limitations of scheduling and patient consent, we were unable to study sequential patients, a factor that may introduce a selection bias. This study included many adenocarcinomas, especially bronchioloalveolar carcinomas; however, recent evidence suggests that the number of cases of adenocarcinoma of the lung has increased dramatically in the last decade and this is largely attributed to an increase in bronchioloalveolar carcinoma (21,22). Therefore, we performed additional survival and disease-free survival analyses to see whether 18F-FDG uptake (SUV) has a significant discriminate value for prognosis in patients with lung cancer other than bronchioloalveolar carcinoma. In 44 patients with lung cancer other than bronchioloalveolar carcinoma, those with an SUV of ≤5 had a significantly better survival rate and disease-free survival rate than patients with an SUV of >5. In patients with pathologic stage I and stage IA lung cancers other than bronchioloalveolar carcinoma, the SUV was correlated with disease-free survival. A multivariate analysis also identified the SUV as the most significant independent factor for disease-free survival. Thus, 18F-FDG uptake (SUV) also has a significant independent postoperative prognostic value for recurrence in patients with lung cancer other than bronchioloalveolar carcinoma.
Third, we did not include the data of PCNA or Ki-67 expression in multivariate disease-free survival analysis, although measures of tumor proliferation with PCNA and Ki-67 expression have prognostic value in patients with resected NSCLC. Clearly, additional study is essential to determine whether the SUV has a postoperative prognostic value for recurrence beyond that provided by PCNA and Ki-67 expression.
Univariate and multivariate analyses showed that an increased SUV identifies a subgroup of patients with the worst prognosis for recurrence, and this parameter seems to be more important than pathologic stage as a prognostic factor for recurrence. Patients with pathologic stage I disease and a hypermetabolic lesion may benefit from chemotherapy or radiotherapy (or both) after surgery. No clear data support the possibility that additional treatment in this setting improves survival. If a group of these high-risk patients who realistically have microscopic metastasis at presentation could be identified, improved outcomes may be possible. Further studies assessing patient survival after various therapeutic protocols are recommended.
CONCLUSION
18F-FDG uptake in primary NSCLC patients determined by PET has a significant independent postoperative prognostic value for recurrence, especially in patients with pathologic stage I NSCLC: The greater the 18F-FDG uptake in lung cancer, the higher the incidence of metastasis. 18F-FDG uptake was superior to pathologic stage in predicting relapse of patients with NSCLC.
Acknowledgments
This work was supported by a Grant for Project Research (H2001-2 and A1999-1) from the High-Technology Center of Kanazawa Medical University, a Grant-in-Aid for Cancer Research (12-4) from the Ministry of Health, Labour and Welfare, Japan, and a Grant-in-Aid for Scientific Research (13670192) from the Ministry of Education, Science, and Culture, Japan.
Footnotes
Received May 23, 2001; revision accepted Sep. 25, 2001.
For correspondence or reprints contact: Kotaro Higashi, MD, Department of Radiology, Kanazawa Medical University, 1-1, Daigaku, Uchinada, Kahoku-gun, Ishikawa, 920-0293, Japan.
E-mail: h550208{at}kanazawa-med.ac.jp
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Primary tumour standardised uptake value is prognostic in nonsmall cell lung cancer: a multivariate pooled analysis of individual data
- Value of Metabolic Tumor Volume on Repeated 18F-FDG PET/CT for Early Prediction of Survival in Locally Advanced Non-Small Cell Lung Cancer Treated with Concurrent Chemoradiotherapy
- Prediction of Recurrence after Complete Resection in Patients with NSCLC
- Complementary Roles of Whole-Body Diffusion-Weighted MRI and 18F-FDG PET: The State of the Art and Potential Applications
- 18F-FDG Uptake in Lung, Breast, and Colon Cancers: Molecular Biology Correlates and Disease Characterization
- The role of positron emission tomography in the management of non-small cell lung cancer
- Prognostic Value of Fluorine-18 Fluorodeoxyglucose Positron Emission Tomography Imaging in Patients With Advanced-Stage Non-Small-Cell Lung Carcinoma
- Fluorodeoxyglucose Uptake of Primary Non-Small Cell Lung Cancer at Positron Emission Tomography: New Contrary Data on Prognostic Role
- Bone Marrow Hypermetabolism on 18F-FDG PET as a Survival Prognostic Factor in Non-Small Cell Lung Cancer
- Microvessel Density: Correlation with 18F-FDG Uptake and Prognostic Impact in Lung Adenocarcinomas
- Findings on 18F-FDG PET Scans After Neoadjuvant Chemoradiation Provides Prognostic Stratification in Patients with Locally Advanced Rectal Carcinoma Subsequently Treated by Radical Surgery
- Functional Imaging in Lung Cancer
- [18F]Fluorodeoxyglucose Uptake by Positron Emission Tomography Predicts Outcome of Non-Small-Cell Lung Cancer
- 18F-FDG Uptake by Primary Tumor as a Predictor of Intratumoral Lymphatic Vessel Invasion and Lymph Node Involvement in Non-Small Cell Lung Cancer: Analysis of a Multicenter Study
- The Role of PET Scan in Diagnosis, Staging, and Management of Non-Small Cell Lung Cancer
- Preoperative F-18 Fluorodeoxyglucose-Positron Emission Tomography Maximal Standardized Uptake Value Predicts Survival After Lung Cancer Resection
- In Vitro Proton Magnetic Resonance Spectroscopic Lactate and Choline Measurements, 18F-FDG Uptake, and Prognosis in Patients with Lung Adenocarcinoma
- Relationship between Non-Small Cell Lung Cancer Fluorodeoxyglucose Uptake at Positron Emission Tomography and Surgical Stage with Relevance to Patient Prognosis
- American Society of Clinical Oncology Treatment of Unresectable Non-Small-Cell Lung Cancer Guideline: Update 2003
- Whole-Body 18F-FDG PET Identifies High-Risk Myeloma