


Abstract
Several studies have found that administration of etidronate results in competitive interference with 99mTc-labeled bone scanning reagents. In contrast, in other studies this problem was not encountered with other bisphosphonates. Methods: We prospectively studied 9 patients with hormone-refractory prostate cancer. 99mTc-methylene diphosphonate (MDP) bone scanning was performed before they received alendronate, and scanning was repeated a mean of 16.6 d afterward, when the patients had been receiving 40 mg alendronate daily for a mean of 6 d. In addition, 7 patients who underwent delayed scanning when they had been receiving alendronate for a mean of 111 d were also restudied. Quantitative whole-body bone scanning was performed, and radioactivity deposited in the bone metastasis was determined using region-of-interest analysis. Results: A <6% increase in whole-body retention of 99mTc-MDP was seen on the initial postalendronate scan compared with the baseline scan. No significant differences in activity were seen in the bone lesion evaluated on the baseline and initial postalendronate studies. The delayed postalendronate scan generally showed similar or higher tracer accumulation compared with the baseline scan. Conclusion: Alendronate did not competitively inhibit uptake of 99mTc-MDP in the skeleton or tumor metastasis. Use of alendronate before bone scanning is unlikely to result in decreased detection of lesions or falsely decreased 99mTc-MDP activity at metastatic bone tumor sites.
Bisphosphonates are being used successfully for the treatment of osteoporosis (1) and Paget’s disease of bone (2). In addition, the use of bisphosphonates to treat hypercalcemia associated with metastatic disease to bone is now standard (3). Their use in malignancies has also been successful in reducing bone pain (4) and decreasing the skeletal complications of metastatic bone disease (3), as well as increasing the median time to progression (5). The mechanism of bone damage in the presence of metastatic disease to bone is not completely understood. Osteoclasts are believed to have a central role (6). Bone resorption associated with metastatic disease is often thought to be related to activation of osteoclasts rather than to direct bone destruction by tumor cells. Compounds that inhibit osteoclasts may therefore slow the progress of metastatic bone disease or retard its occurrence. We are evaluating the utility of alendronate in combination with ketoconazole in patients with androgen-independent prostate cancer and at least 1 bone lesion shown on bone scans.
Bone scanning is performed with technetium-labeled bisphosphonates that are similar to the bisphosphonates used for therapeutic applications. There are conflicting data as to the effect of bisphosphonate therapy on localization of 99mTc-labeled bisphosphonates to bone and as to whether they cause competitive inhibition of bone uptake in tumors (7–15), thus resulting in false-negative bone scans and reducing the diagnostic sensitivity of bone scans.
Localization studies using 99mTc-labeled methylene diphosphonate (MDP) after intravenous injection of etidronate to rats showed a marked decrease in uptake in the skeleton (16). This interference could be problematic because bone scans are commonly used to assess the progress or response of metastatic disease to therapy. Several studies have found that in patients receiving etidronate intravenously or orally, bone uptake of 99mTc-labeled bone scanning agents is decreased (7,8,15,17). This finding has led to recommendations for a waiting period between bisphosphonate administration and bone scanning (7,17).
Studies with other bisphosphonates (nonetidronate) have had conflicting results. In a prospective study of 11 women with breast cancer who were treated intravenously with 300 mg clodronate for 21 d (10), no adverse effect on 99mTc-MDP uptake was noted. Macro et al. (12), in a prospective study of patients with Paget’s disease (n = 5) or metastatic bone disease (n = 6), determined the effect of pamidronate administration for up to 6 mo, with the last dose given within a mean of 30 h of the bone scan injection. The number of lesions and the activity of the lesions were unchanged after pamidronate administration. In 2 studies of patients with Paget’s disease treated with long-term pamidronate, bone scanning showed a decrease in uptake in the index lesion. Nevertheless, this decrease was probably related to the therapeutic effect of the pamidronate on the lesions rather than to competitive inhibition with falsely decreased uptake of the 99mTc-oxidronate (13) or 99mTc-MDP (9) bone tracer. Rather than interfering with bone scanning, the long-term treatment with pamidronate probably resulted in a true decrease in metabolic activity of bone in the area of the tumor.
Other bisphosphonates are being used clinically and have the potential to interfere with 99mTc-labeled bone scanning reagents. Alendronate has been labeled with 99mTc, and the resulting images were similar to those obtained with 99mTc-MDP (18). Koyano et al. (11) reported that intravenous alendronate (10 mg) interferes with the detection of lesions on 99mTc-hydroxymethylene diphosphonate bone scans. In several studies, patients had hypercalcemia, which may have interfered with bone scanning by forming complexes between calcium and bisphosphonates that would interfere with tracer distribution.
We recently embarked on a study using alendronate in conjunction with ketoconazole in patients with metastatic androgen-independent prostate cancer. In these patients, use of 99mTc bone scans to evaluate progression or tumor response is common. Because alendronate is a bisphosphonate, which can theoretically interfere with bone scans, we prospectively evaluated whether a short course of treatment with alendronate would compete and interfere with uptake of the bone scan radiopharmaceutical.
MATERIALS AND METHODS
Patient Population
Nine patients (age range, 51–74 y; mean age, 67 y) with hormone-refractory prostate cancer metastatic to the bone were to receive alendronate and ketoconazole prospectively under a protocol approved by the institutional review board of the National Cancer Institute. All patients gave written informed consent before participating. The patients had failed to benefit from prior androgen ablation (bone lesions had increased) and were maintained on medical or surgical castration. All patients underwent baseline scanning before alendronate therapy and follow-up scanning when they had been receiving alendronate for ≤1 wk (initial postalendronate scans). To determine if longer periods of alendronate administration competed with bone uptake of 99Tc-MDP, we obtained bone scans after approximately 4 mo of alendronate therapy (delayed postalendronate scans) and analyzed them in a similar fashion. Delayed postalendronate scans were analyzed for 6 patients, delayed scans were not available for 2 patients because they had gone off the protocol, and the scan of 1 patient could not be analyzed because it had been obtained using different technical parameters.
Oral alendronate was administered at a dose of 40 mg daily before the repeated bone scanning and was continued while it was performed. For 5 patients the bone scan showed extensive disseminated metastatic bone disease, whereas for 4 patients the disease was more limited, with fewer than 5 abnormal sites seen on the bone scan.
Bone scanning was performed in our standard format with an intended nominal dose of 925 MBq (25 mCi) and a scanning time of 3 h after tracer administration. 99mTc-MDP (Bracco Diagnostics, New Brunswick, NJ) was used. The bone scanning agents were prepared on site using our standard operating procedure based on the manufacturer’s recommended method. The patients were encouraged to drink fluids. Whole-body scanning was performed using a large-field-of-view double-head gamma camera (ADAC Laboratories, Milpitas, CA) and a low-energy high-resolution collimator. Scans were acquired over a mean of 22 ± 1 min (range, 20.3–23.5 min).
After baseline bone scanning, up to 5 lesions (range, 2–5) were selected for region-of-interest analysis and were reanalyzed on the repeated initial and delayed postalendronate bone scans. For each patient, the ratios of the total activity in each of the selected lesions on the baseline and postalendronate scans and of the maximal counts per pixel were determined. Then, the mean ratios were determined for each patient. In addition, for paired comparisons, the activity in a single index lesion (selected on the initial scan) was determined for each patient on both the baseline and the postalendronate scans. The index lesion was selected on the basis of good visualization, lack of overlap, and ease of drawing a region of interest on the baseline scan without reviewing the postalendronate scan, so as not to introduce bias. On the initial and delayed postalendronate scans, the same lesions were detected and similar regions of interest were again drawn or copied from the baseline scan. The total counts in the index lesion, normalized to the injected activity, were determined and compared on the baseline and postalendronate scans. To determine the whole-body retention, a large rectangle was drawn around the whole body and a smaller rectangle was drawn over a nonbody background area. The total counts in the whole body minus the background counts and the total counts in the selected lesions were normalized to the injected dose, accounting for decay. The ratio of the activity in the selected lesions or in the whole body was determined for the postalendronate and baseline scans (counts after alendronate/counts at baseline).
Statistical Analysis
Paired data were analyzed using the paired t test (Sigmastat; Jandel Corp., San Rafael, CA). The whole-body counts on the baseline and postalendronate scans were compared statistically, and the activity in the index lesion on the baseline and postalendronate scans was determined and paired t test comparisons were performed.
RESULTS
Scanning data are shown in Table 1. The injected doses for both the baseline study (917.6 ± 53.3 MBq [24.8 ± 1.4 mCi]) and the postalendronate study (909.5 ± 38.7 MBq [24.6 ± 1.1 mCi]) were not significantly different (P = 0.729). The mean time from injection to scanning for all studies was 179.4 ± 17.4 min. Overall, the baseline and initial postalendronate studies did not significantly differ in the length of time between injection and scanning (P = 0.943). A mean of 17 d (range, 13–29 d) elapsed between the baseline and initial postalendronate studies. The patients had been receiving alendronate for a mean of 6 ± 1.4 d (range, 3–8 d) before postalendronate scanning, and all patients were receiving alendronate at the time of bone scanning.
Scanning and Alendronate Administration Data
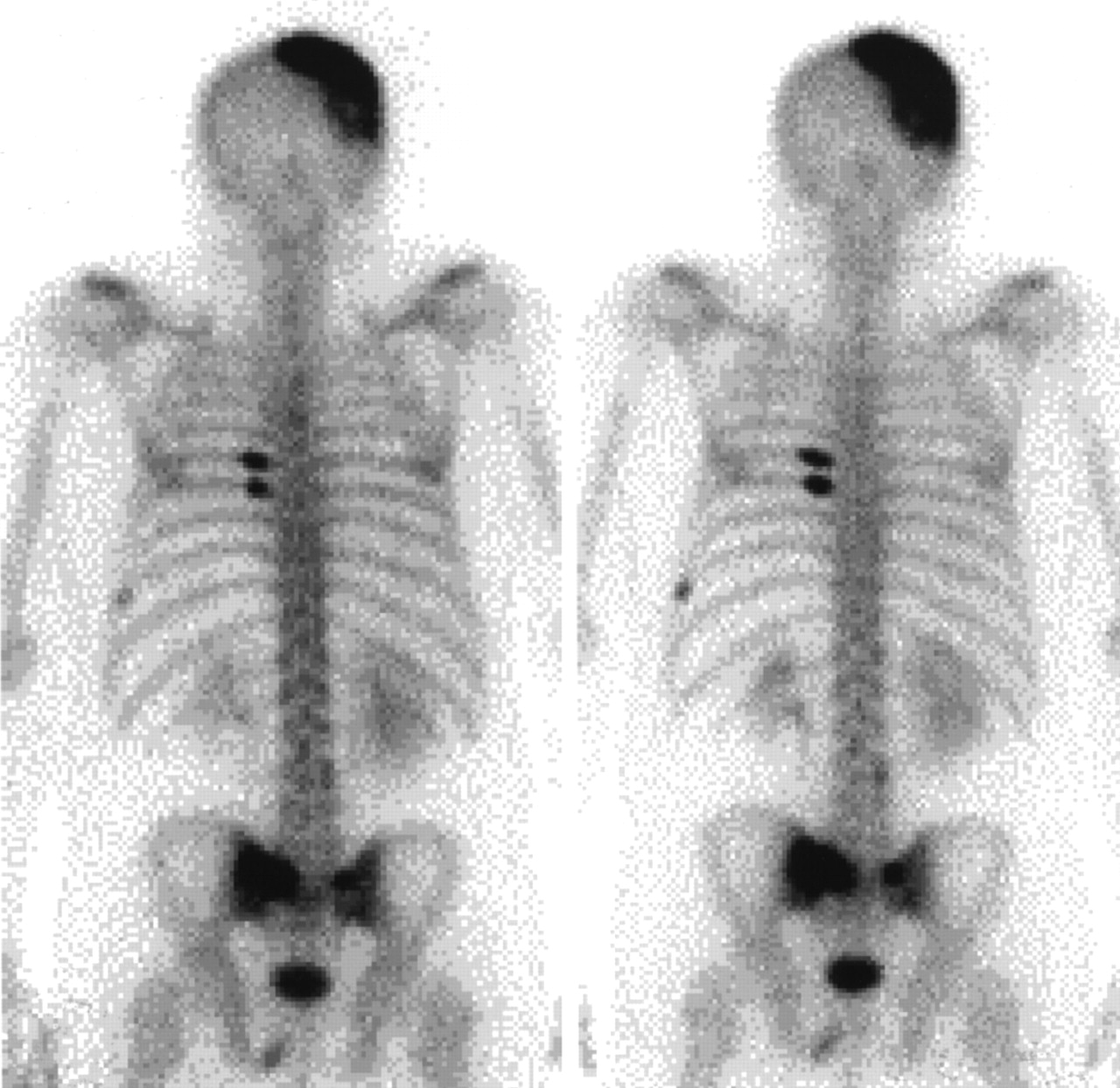
Visually, 6 of the initial postalendronate scans showed no change in tracer uptake compared with baseline. For 3 patients, at least 1 lesion appeared to be slightly more prominent on the initial postalendronate scan than on the baseline scan. No new lesions were noted on any of the initial postalendronate scans, and only 1 lesion appeared improved on the initial postalendronate scan. Representative baseline and initial postalendronate scans are shown in Figure 1.

Posterior whole-body scan from patient 4. Metastatic sites to skull, ribs, and pelvis seen on baseline scan (left) are as well visualized on postalendronate scan (right).
Slight differences were seen in the whole-body retention of 99mTc-MDP (P = 0.01). Baseline scans had a mean total whole-body count of 111,183 ± 11,988 per 37 MBq administered, compared with 117,721 ± 10,034 per 37 MBq administered for the initial postalendronate scans. This difference represented a <6% increase in whole-body retention on the initial postalendronate scans (Table 2).
Comparison of Ratio of Activity in Whole Body and Index Lesions (Postalendronate/Baseline)
The total activity in the index lesions was determined. Although the mean total activity on the initial postalendronate scans was slightly higher than that on the baseline scans (Table 2), this increase was not significant (1.175 ± 0.839 cps vs. 1.392 ± 1.225 cps normalized to the number of megabecquerels administered [P = 0.182]).
For each patient, both the total counts and the maximum counts per pixel in each lesion were determined. The mean ratio of activity on initial postalendronate scans versus baseline scans for all lesions in a given patient was then obtained (Table 3). In general, an increase or, in some cases, a small decrease in both measurements for the initial postalendronate scan was seen.
Comparison of Ratio of Activity in Postalendronate vs. Baseline Scans in All Bony Metastatic Lesions Analyzed
Delayed scanning was performed a mean of 112 d (range, 99–127 d) after the patients began receiving alendronate (Table 1). The ratio of whole-body counts on the delayed postalendronate scan was similar to that on the initial postalendronate scan (Table 2). When the whole-body counts corrected for administered dose were directly compared, no significant differences were seen (ANOVA, P = 0.67). The ratio of activity on the delayed postalendronate scan compared with the baseline scan also indicated that, in general, no decrease in activity occurred in the index lesions (Table 2).
DISCUSSION
Because the bisphosphonates in use have similar structures to all routine bone-scanning agents, these drugs could, theoretically, interfere with bone scan localization. This interference has been observed when bone scanning has been performed after etidronate therapy (7,8). In contrast, the only 2 prospective studies using bisphosphonates (clodronate and pamidronate) did not show interference with 99mTc-labeled bisphosphonate localization (9,10).
Because we were interested in treating patients with alendronate in combination with other potential anti–prostate cancer reagents, we needed to ensure that any changes observed on the bone scan were caused by changes in bone metabolism and not by a competitive carrier effect. This concern was heightened by the report that 99mTc-labeled alendronate showed higher and faster accumulation than 99mTc-MDP (18). Our study showed that oral administration of alendronate did not competitively and adversely interfere with accumulation of the 99mTc-MDP bone-scanning agent in tumors. The total retained activity shown on the whole-body scans after administration of alendronate was also similar to that on the baseline scans. The 6% higher whole-body retention seen on the initial postalendronate scans may be related to a slight disease progression during the delays between the baseline and postalendronate studies (mean, 16.6 d). Furthermore, the initial-postalendronate–to–baseline ratio of uptake seen in the metastatic bone lesions was often >1 and only once <0.90, suggesting that alendronate did not compete significantly with 99mTc-MDP (Table 2). Direct comparison of activity on the baseline and initial postalendronate studies showed that alendronate did not interfere with the ability to detect metastatic disease.
We believe that the mean duration of alendronate administration (7 d) should have been enough to show whether a competitive effect with 99Tc-MDP existed. The pharmacokinetics of alendronate are characterized by poor bioavailability (1%–2%) (19). Nonetheless, for the percentage of drug that does enter the circulation, >97% is renally eliminated within 24 h. This fact supports the sufficiency of the interval we chose between baseline and postalendronate scanning to achieve a pseudo steady state (20). Furthermore, our analysis of the delayed bone scans acquired while the patients had been receiving alendronate for a mean of 112 d showed that the patients had a similar overall retention in their whole body. In addition, uptake in the index lesion of most patients either increased or very slightly decreased. Therefore, any improvement in bone lesions seen on the bone scans is unlikely to be related to competition between alendronate and 99mTc-MDP but, rather, is secondary to an effect on bone-level metabolism from the alendronate or any concomitant therapy.
CONCLUSION
Administration of alendronate did not competitively inhibit 99mTc-MDP uptake and is unlikely to result in false-negative findings or interference with tumor visualization.
Footnotes
Received Jan. 16, 2001; revision accepted May 14, 2001.
For correspondence or reprints contact: Jorge A. Carrasquillo, MD, Bldg. 10, Room 1C496, 10 Center Dr. MSC 1180, Bethesda, MD 20892-1180.




{kind=link}