


Abstract
Bone metastasis occurs as a result of a complex pathophysiologic process between host and tumor cells leading to cellular invasion, migration adhesion, and stimulation of osteoclastic and osteoblastic activity. The process is mediated by parathyroid hormones, cytokines, and tumor-derived factors. Several sequelae occur as a result of osseous metastases and resulting bone pain can lead to significant debilitation. Pain associated with osseous metastasis is thought to be distinct from neuropathic or inflammatory pain. Several mechanisms—such as invasion of tumor cells, spinal cord astrogliosis, and sensitization of nervous system—have been postulated to cause pain. Pharmaceutical therapy of bone pain includes nonsteroidal analgesics and opiates. These drugs are associated with side effects, and tolerance to these agents necessitates treatment with other modalities. Bisphosphonates act by inhibiting osteoclast-mediated resorption and have been increasingly used in treatment of painful bone metastasis. While external beam radiation therapy remains the mainstay of pain palliation of solitary lesions, bone-seeking radiopharmaceuticals have entered the therapeutic armamentarium for the treatment of multiple painful osseous lesions. 32P has been used for >3 decades in the treatment of multiple osseous metastases. The myelosuppression caused by this agent has led to the development of other bone-seeking radiopharmaceuticals, including 89SrCl, 153Sm-ethylenediaminetetramethylene phosphonic acid (153Sm-EDTMP), 179mSnCl, and 166Ho-Labeled 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetramethylenephosphonate (166Ho-DOTMP). 89Sr is a bone-seeking radionuclide, whereas 153Sm-EDTMP is a bone-seeking tetraphosphonate; both have been approved by the Food and Drug Administration for the treatment of painful osseous metastases. While both agents have been shown to have efficacy in the treatment of painful osseous metastases from prostate cancer, they may also have utility in the treatment of painful osseous metastases from breast cancer and perhaps from non-small cell lung cancer. This article illustrates the salient features of these radiopharmaceuticals, including the approved dose, method of administration, and indications for use. We conclude with recommended guidelines for therapy and follow-up.
Bone metastasis is a major complication of several solid cancers; the prostate, breast, lung, kidney, and thyroid are cancers most associated with bone pain (most often, breast and prostate). Although bone metastases are often clinically silent, they can lead to serious sequelae, such as pain, fractures, and hypercalcemia. These complications often reduce performance status and decrease the quality of life. Bone pain due to metastasis is often considered a unique type of pain. It is initially a dull or aching pain, worse at night, that improves with physical activity (1). If pain increases with physical activity, the risk of imminent fracture is increased.
The pathophysiology of bone metastasis and related complications is complex. Normal bone undergoes continuous remodeling that is essential to maintain mechanical function. The process is performed by a multicellular unit formed by 2 different cell types, osteoclasts and osteoblasts. Osteoclasts resorb bone, whereas osteoblasts replace bone (2). Systemic factors—such as the parathyroid hormone, local osteoclast-activating cytokines, and growth factors—contribute to the process (3). During bone resorption, growth factors and mineral ions are released from the bone matrix. When bone metastases occurs, a cycle of signaling takes place that results in increased osteolytic activity. Tumor-derived factors stimulate osteoclast-mediated bone resorption, whereas the growth factors released from the bone matrix stimulate the tumor cells to grow and secrete additional cytokines. This leads to osteopenia and increased risk of developing fractures and, when lesions are in vertebrae, spinal cord compression. The calcium released from the bone matrix in the course of this process can lead to the hypercalcemia of malignancy (HCM), a serious metabolic condition.
Skeletal metastasis is a multifactorial process in which several biologic processes play a role leading to interaction between host and tumor cells. Cellular invasion and migration, cell matrix adhesion or cell-to-cell adhesions, interaction with endothelial cells, regulation of growth factor, and stimulation of osteoclasts and osteoblasts are thought to contribute to development of skeletal metastasis. Cadtherins, integrins, imuunoglobulins, selectins, and CD44 are some of the molecules implicated in loss of cellular adhesion that causes cell matrix detachment, invasion, and migration. Several isoforms of CD44, an adhesion molecule that binds hyaluronate, have been associated with lymphatic spread of the tumors and are expressed in breast and colon cancers. P selectins bind to a wide range of carcinoma cells, including breast, colon, and lung. Interaction with the endothelial cells leads to local arrest or further migration of the tumor cells. Platelet fibrin thrombi and inflammatory cytokines lead to adhesions and arrest of the tumor cells, whereas chemotactic factors lead to increased mobility of tumor cells. Invasiveness is mediated by several enzyme systems, including serine proteases, of which matrix metalloproteins and urokinase plasminogen activation system are thought to be most important. Cellular motility is critical for tumor cells to develop distant metastasis. Motility is mediated by several factors, including: growth factors, hyaluronians, components of matrix, and host- or tumor-secreted factors. Cytokinins such as autotoxin and hepatocyte growth factor are also implicated in inducing cell motility (4–7).
Pain from bone metastasis is of variable intensity and intermittent at onset but progresses to continuous low level pain with episodes of breakthrough pain, which later becomes chronic pain. Mechanical allodynia, in which normal nonpainful activity such as coughing and gentle limb movements can also be perceived as painful, can occur leading to significant limitation of activity. Bone pain is thought to be distinct from neuropathic or inflammatory pain, where there is upregulation of the glial fibrillary acidic protein in the spinal cord indicating astrogliosis. The exact mechanism of cancer pain is unknown and it is postulated that the pain may be due to the presence of tumor in the bone. Treatment with bisphosphonates supports the thought that osteolysis leads to bone pain, which is linked to the number and extent of osteoclastic activity. Bone cancer pain is also thought to occur due to sensitization of the nervous system. Sensory information from peripheral tissues is transmitted to the spinal cord and brain by primary afferent sensory neurons, nociceptors that detect stimuli that are perceived as harmful and convert into electrochemical signals that are transmitted to the central nervous system. Tumors secrete a variety of factors that sensitize or directly excite primary afferent neurons, causing the sensation of pain. Receptors for many of these factors are expressed by primary afferent neurons. Peripheral sensitization leads to increased release of substance P from nociceptors, even with minor stimulation. Sensitization also occurs centrally in the dorsal horn of the spinal cord, which leads to allodynia and hyperalgesia. The spinal cord may show marked astrocytosis, increased expression of c-Fos (a general marker of neuronal activity), and a peptide—dynorphin. Other factors that may contribute to the activation of sensory neurons, is the lower intracellular and extracellular pH of solid tumors, which can also cause pain in cancer patients. It is also thought that tumor growth may entrap and injure nerves, causing neuropathic pain (8–10).
Management of bone pain includes analgesia, radiation, radiofrequency (RF) ablation, hormones, chemotherapy, and surgery. Localized sites of involvement can be treated with surgery, RF ablation, or external beam radiation, whereas radiopharmaceuticals, hormones, and chemotherapy are used to treat more diffuse bone involvement.
Control of bone pain usually begins with analgesic medications used in a 3-step approach. Nonsteroidal antiinflammatory drugs (NSAIDs), including aspirin, ibuprofen, and naproxen, are used to relieve mild to moderate pain initially. With persistent or increased pain while on NSAIDs, treatment progresses to the second step, which utilizes weak opioids, such as codeine or hydrocodone, changing to higher doses or more potent opioids (step 3), such as morphine, hydromorphone, or fentanyl, if the pain persists or becomes more severe. The more potent narcotic agents have significant side effects, including constipation, limitations in mental and physical status, and addiction. Lethargy and constipation are particularly common symptoms. Increased doses also increase the cost significantly when used on a long-term basis. To limit the dose of these medications, radiation therapy and surgery are used for the treatment of localized bone metastases. Some patients with extensive disease in a portion of the body are candidates for hemibody irradiation. Hemibody radiation provides relief from pain associated with extensive bone involvement, but it is associated with a high incidence of side effects (11). Bone-seeking radionuclides are therefore preferred for widespread painful bone metastasis (12).
BISPHOSPHONATES
Bisphosphonates (Fig. 1) inhibit osteoclast-mediated bone resorption by binding to bone mineral, interfering with osteoclast activation. These agents also promote repair by stimulating osteoblast differentiation and bone formation. As a result, these agents are playing an increasing role in the treatment of painful bone metastases.

Structure of bisphosphonate.
Bisphosphonates are used in the treatment of benign conditions, such as osteoporosis; in malignancies with osteoblastic and osteolytic bone metastases as well as HCM (13,14). The use of bisphosphonates has made a significant change in the therapeutic approach to management of bone metastasis and pain prevention in breast cancer and multiple myeloma (15). Bisphosphonates reduce skeletal complications (16): delay progression of existing bone metastases and reduce the development of new lesions in patients with breast cancer and multiple myeloma (17,18).
Pamidronate, zoledronate, and clodronate are some of the bisphosphonates that have been used clinically. Pamidronate is a second-generation bisphosphonate that is effective in patients with multiple myeloma or breast cancer, who primarily have osteolytic metastases (19,20), and is shown to reduce skeletal complication and morbidity in patients with breast cancer (20–22). Zoledronic acid is a newer nitrogen-containing bisphosphonate that has been evaluated in bone metastases from a variety of cancers. Zoledronic acid was shown to be as effective as pamidronate in reducing skeletal complications (23) but was superior in treating hypercalcemia (24). In breast cancer patients, bisphosphonate therapy is recommended for patients with radiographic evidence of bone destruction but is not recommended for treatment based an abnormal bone scan alone (25). This therapy also reduces skeletal-related events in hormone-refractory prostate cancer (26), non-small cell lung cancer, and urologic malignancies (27,28).
There has been concern regarding the efficacy of bone scanning in patients who were treated with bisphosphonates since methylene diphosphonate (MDP) is similar to the bisphosphonates. The literature is controversial, suggesting that the timing of the bone scan vis-à-vis the last dose of bisphosphonate is critical, though this has not been borne out by studies with etidronate and alendronate (29–31).
RADIATION THERAPY
External beam radiation therapy can often produce pain relief within 48 h of the start of therapy. External beam therapy is most effective when the disease is localized, allowing the highest dose to be delivered to the lesion. If multiple lesions at multiple sites require therapy, side effects—particularly bone marrow suppression—limit the dose that can be delivered. Hemibody radiation therapy has been used in patients with widespread lesions and pain but can lead to significant toxicity, including alopecia and radiation pneumonitis if the upper body is treated; or nausea, vomiting, and diarrhea if the lower body is treated. Myelosuppression can also occur especially in patients treated with whole-body radiation.
The mechanism of pain relief after radiation therapy is not known. Radiation causes a reduction in the number of viable tumor cells that may result in shrinkage of the tumor. Removal of the tumor from bone then enables osteoblastic repair, restoring integrity of the damaged bone. However, certain features—especially the lack of a dose-response relationship and the rapid pain relief, which may be seen especially after systemic radiation (within 24–48 h in up to 25% of patients)—make it unlikely that tumor shrinkage itself is responsible for the pain relief (32). It has also been suggested that radiation may have an analgesic effect through osteoclast inhibition, which provides an insight to bisphosphonate activity (33).
In about 80% of patients with local pain, a single dose of radiation will achieve pain relief within 4–6 wk. If a lesion recurs at that site, retreatment is effective if subradical doses were used (34–36). Wide-field external beam treatment aimed to cover areas roughly equivalent to the half-body above or below the diaphragm depending on the sites of pain may be given in those with widespread disease or where systemic treatment has failed or is inappropriate. Treatment is delivered as single doses of 6 Gy to the upper hemibody, which is limited by lung tolerance, and 8 Gy to the lower hemibody (37). Sequential hemibody radiotherapy, allowing 4–6 wk between each treatment, is given to achieve coverage of the whole skeleton with external beam radiotherapy. The interval between treatments is useful for bone marrow regeneration. After lower hemibody treatment, short-lived and self-limiting nausea and gastrointestinal upset are common; in upper hemibody treatment, pneumonitis is common if tolerance doses are exceeded. Symptomatic bone marrow depression may also occur and transfusion is often required to maintain the hemoglobin in the early weeks after treatment (38), though life-threatening complications such as neutropenia or thrombocytopenia are unusual.
RADIOPHARMACEUTICAL THERAPY
Since multiple sites of osseous metastases are common and some patients have multifocal bone pain, systemic targeted treatment of the skeletal metastatic sites offers the potential of pain relief with minimal side effects. Radiopharmaceuticals developed for the treatment of painful bone metastases use the following radionuclides: 32P, 89Sr, 186Re, 188Re, 153Sm, and 177Lu (Table 1). All agents have advantages and side effects. The agents differ in terms of efficacy; duration of pain palliation; tumoricidal effects; ability to repeat treatments; toxicity, and expense. Most studies with these agents have been conducted in prostate and breast cancer patients.
Radiopharmaceuticals
MECHANISM OF ACTION
The sources of radiation within bone differ with the radiopharmaceutical used: The metallic chelated radiotracers tend to chemically absorb to the trabecular surface, whereas 32P and 89Sr (as the chloride) distribute more widely throughout bone. Due to the heterogeneity of radiopharmaceutical uptake, spicule thickening, and tumor and marrow distribution, there is variation in dosimetry (39).
32P
32P is a reactor-produced, pure β-emitting radionuclide with a physical half-life of 14.3 d. The maximum and mean β-particle energies are 1.71 and 0.695 MeV, respectively, with the mean and maximum particle range in tissue of 3 and 8 mm, respectively. Oral and injectable 32P (usually the injectable sodium orthophosphate) was introduced for treatment of metastatic bone pain >50 y ago. 32P is incorporated into the hydroxyapatite molecule present in large amounts in most osseous metastases. The likely mechanism of action is DNA damage from decay to 32S, with subsequent cell death, as well as damage to cells producing pain modulators—for example, lymphocytes that produce lymphokines.
32P as sodium orthophosphate was one of the first radiopharmaceuticals used to reduce pain from bone metastases (40) and the most widely used radiotracer until the 1980s (41). Its uptake in malignant tissue was demonstrated by Lawrence et al. (42). Earlier studies used testosterone and androgen stimulation for 32P bone metastasis therapy (43–45). The response rates were between 59% and 93% for prostate cancer and between 52% and 94% for breast cancer, with overall response rates of 77% and 84%. No dose-response relationship was seen. Pain palliation occurred within 14 d, with a range of 2 d to 4 wk. A major problem with 32P therapy is the occurrence of toxicity, including myelosuppression and pancytopenia. Additional concerns include the very high β-energy and low lesion-to-normal bone ratio. Pancytopenia occurs around 4–5 wk, with recovery by 6–7 wk, and is dose dependent. However, this is not found to be clinically significant with either a single dose or even multiple doses up to 444 MBq (12 mCi). Acute leukemias have been reported with use of 32P in polycythemia vera; however, grade 4 leukopenia and thrombocytopenia are quite rare (41).
89SrCl
Strontium is an element that behaves biologically like calcium. It localizes in bone primarily in areas of osteoblastic activity. 89Sr has a physical half-life of 50.5 d and emits a β-particle with a maximum energy of 1.46 MeV and an average soft-tissue range of 2.4 mm. The usual therapeutic dose is 148 MBq (4 mCi).
After intravenous administration, 89Sr is concentrated in bone in proportion to osteoblastic activity. Of the 89Sr that is not concentrated in bone, about 80% is excreted through the kidneys and about 20% through the gastrointestinal system. Although the biologic half-life is 4–5 d, about 20% is retained in the body after 90 d (46).
89Sr therapy can relieve bone pain for up to 14 mo and is recommended for use in patients with moderate pain and a reasonable life expectancy. Response rates range from 60% to 84% (47). The onset of pain relief is generally within 7–21 d, with a mean duration of relief of about 6 mo. Transient increased bone pain (painful flare) may occur in the first 2–3 d after treatment. This is usually mild, self-limited, and controlled with analgesics. A flare usually heralds a good treatment response. Patients can be retreated after 90 d, though multiple therapies may lead to greater marrow toxicity. There is a dose-response relationship for complete relief of pain (though not for partial pain relief) (48). Several studies have demonstrated no significant differences between response to 89Sr and response to local or hemibody radiation (49,50). Concurrently administered chemotherapy is effective in enhancing pain relief and delaying the onset of new painful metastases (51). However, combining 89Sr with chemotherapy does not increase the overall pain relief response rates (complete plus partial response of 55%–80%). Although the agent is useful for osseous pain palliation, there is no survival benefit, even when a dose of 399.6 MBq (10.8 mCi) is used (49,52). However, in patients with androgen-independent prostate cancer and severe bone pain (53), combined treatment with 89Sr and doxorubicin resulted in a mean survival of 28 mo compared with 17 mo for patients treated with doxorubicin alone. The use of 89Sr can help reduce the lifetime health-care costs by decreasing both the need for radiotherapy and the need for narcotics and hospitalization (54,55).
153Sm
153Sm, a nuclide with a physical half-life of 1.9 d, decays by β-emission. The β-particle has a maximum energy of 0.81 MeV, a mean energy of 0.23 MeV, and an average soft-tissue range of 0.6 mm. The β-ray is accompanied by a 103-keV γ-ray, which is 28% abundant. 153Sm is complexed with ethylenediaminetetramethylene phosphonic acid to form 153Sm-EDTMP. This phosphonate complex concentrates in the skeleton, in proportion to osteoblastic activity. After intravenous injection, <1% remains in the blood at 5 h. About 65% of the dose remains in the skeleton. The urinary excretion is nearly complete by 6 h (56). The distribution of 153Sm-EDTMP is identical to that of bone-seeking radiopharmaceuticals such as 99mTc-MDP (99mTc-methylene diphosphonate) (57) (Fig. 2). 153Sm-EDTMP is usually administered at a dose of 37 MBq/kg (1 mCi/kg). An initial dose-escalation study demonstrated dose-limiting myelotoxicity, with a maximum tolerated dose of 37 MBq/kg (1 mCi/kg) (58). Platelet nadir occurred between days 16 and 45 (median, 28 d). Pain palliation occurs in 62%–74% of patients (56,59,60) with better overall responses at higher doses. Pretreatment platelet count, tumor type, prior hormonal therapy, and percentage of 153Sm-EDTMP uptake had more impact on myelotoxicity than the administered activity. Patients with extensive metastases were more likely to have myelotoxicity, probably due to a fragile marrow. Bone marrow suppression was generally mild, reversible, and not associated with grade 4 toxicity. Platelets and white blood cells reached nadir at 3 or 4 wk with both doses and recovered by 8 wk (61). A trend toward improved survival was also seen (59).

Targeting of bone metastases with 153Sm-EDTMP in patient with prostate cancer. ANT = anterior; POST = posterior. Arrow indicates uptake in pubic bone.
153Sm is the most widely used pain palliation radiopharmaceutical agent in the United States. Its ease of use, the ability to image its distribution, and its clinical results (including the ability to titrate the amount based on body weight) make it attractive, while issues with availability, radiation safety, and potential irreversible myelosuppression limit wider use.
Rhenium Isotopes
186Re-Labeled 1,1-hydroxyethylidene diphosphonate (186Re-HEDP/186Re-(Sn)HEDP or etidronate) and 188Re are investigational radiopharmaceuticals for bone pain palliation. 186Re has a physical half-life of 3.7 d and emits a β-particle with a maximum energy of 1.07 MeV, a mean energy of 0.349 MeV, and an average soft-tissue range of 1.1 mm. A study by Sciuto et al. with 186Re-HEDP showed overall pain palliation of 92% in breast cancer patients (47). Pain relief was established early and the tumor-to-bone marrow absorbed dose ratio was 14:1, suggesting its clinical relevance in patients with more compromised bone marrow reserve. Typical marrow recovery times range from 4 to 6 wk. Other reported side effects are mild pain flare phenomenon (6.5%), occurring in the first week after treatment and lasting 2–4 d (62). Several initial studies reported the safety and efficacy of use of 186Re-HEDP in bone pain palliation. The maximum tolerated administered activity of 186Re-HEDP in patients with metastatic breast cancer was found to be 2,405 MBq (65 mCi) with thrombocytopenia as dose-limiting toxicity (63), and a response rate of 77% has been reported (64).
Its role in androgen-independent prostate cancer and multiple other cancers has also been studied with reported response rates of about 50%–100% in various cancers (65,66). For a variety of reasons, however, the agent is not available for use in the United States.
188Re is an isotope of 186Re and is also been used for bone pain palliation. It is inexpensive, as it may be “milked” on demand from a 188W/188Re generator, and a kit is available for attaching it to HEDP. 188Re-(Sn)HEDP has similar biodistribution and radiation dosimetry characteristics as 186Re-(Sn)HEDP and appears to result in similar benefits and toxicities in patients with skeletal metastases. Dosimetric calculations asserted safe, same-day outpatient therapy to be feasible with 188Re-(Sn)HEDP (67). This has mainly been investigated for use in developing countries. It offers the possibility of repeated therapy without additional costs. The high energy of this β-emitter, with a maximal energy of 2.12 MeV, has the potential of killing tumor cells. There are limited data on the use of this agent. An initial study demonstrated pain palliation in 60%–75% of prostate cancer patients receiving a dose of ≥2.6 GBq (68). Recently, the effectiveness of repeated therapy using 188Re-HEDP has been demonstrated in 64 patients with progressive, hormone-resistant prostate cancer (69).
117mSn-Pentetate
The chelate 117mSn-diethylenetriaminepentaacetic acid (117mSn-DTPA) is an experimental radiopharmaceutical undergoing evaluation for treatment of painful bone metastases. 117mSn, a nuclide with a physical half-life of 13.6 d, decays by isomeric transition with emission of the dominant γ-ray at 156 keV. The γ-ray undergoes conversion and it is the conversion electrons that have the therapeutic potential. The energetic conversion electrons have a very short range in soft tissue (0.2−0.3 mm), which may explain the low incidence of myelosuppression seen with 117mSn-pentetate. 117mSn is injected as the pentetate (DTPA) chelate and has no affinity for hydroxyapatite. The mechanism of localization is postulated as precipitation of stannous oxide on bone surfaces or by a hydrolysis reaction with hydroxyapatite. In reported studies, the pain palliation rate is approximately 75%. There is no dose-response relationship; the onset of pain relief is also much earlier than that with the other agents described. At doses of >444 MBq (>12 mCi) (per 70 kg body weight), pain palliation has been noted as early as <1 wk after treatment (70).
PATIENT IDENTIFICATION AND REFERRAL
Patients referred for bone pain palliation therapy are most commonly breast and prostate cancer patients, referred for radiopharmaceutical treatment by the medical oncologists. Before treatment it is mandatory to check the complete blood count, total leukocyte count, and platelet count (Tables 2 and 3). Since the blood counts can change dramatically in these patients, especially if they are receiving other chemotherapy or radiotherapy, the blood counts should be performed within a week before therapy. Patients with myelosuppression should be evaluated carefully to determine if the benefits of treatment outweigh the risks of worsening the myelosuppression.
Common Indications and Contraindications
Checklist Before Administration of Radiopharmaceutical
A detailed history should be taken to evaluate other systemic illness that can affect treatment or increase side effects. An ideal patient is one who has multiple painful bone metastases positive on bone scan and who is clinically experiencing worsening of pain while on nonnarcotic analgesics. A bone scan is necessary to document metastatic disease at the site of pain. With 153Sm, images can be obtained after the dose is administered, making it possible to confirm uptake at the metastatic sites. The imaging is done the same day (2–4 h) or the next day (the latter has the advantage of better visualization of lumbosacral and pelvic disease, as there is clearance from the urinary system).
ADMINISTRATION OF RADIOPHARMACEUTICAL AGENT
Once eligibility is established, the patient is treated in an outpatient setting. A worksheet for assessing the eligibility may be used (Fig. 3). The patient is instructed about the radiation safety precautions. Informed consent is obtained. Patient identifiers are checked. An intravenous line is inserted and one must ensure good blood return and free flow of the saline flush to prevent extravasation of tracer. When 89Sr is used, a fixed dose of 148 MBq (4 mCi) is usually used. If 159Sm is used, the patient is weighed, and 37 MBq/kg (1 mCi/kg) is administered. The dose is administered by an attending physician. The tracer is injected as a slow intravenous injection over a period of 1–2 min and flushed with 10–20 mL of saline. A note is placed in the patient’s record describing the administration. The radiation safety officer is informed and present during the administration. If the patient is treated with samarium, images are usually recorded at 24 h to compare with the diagnostic bone scan.
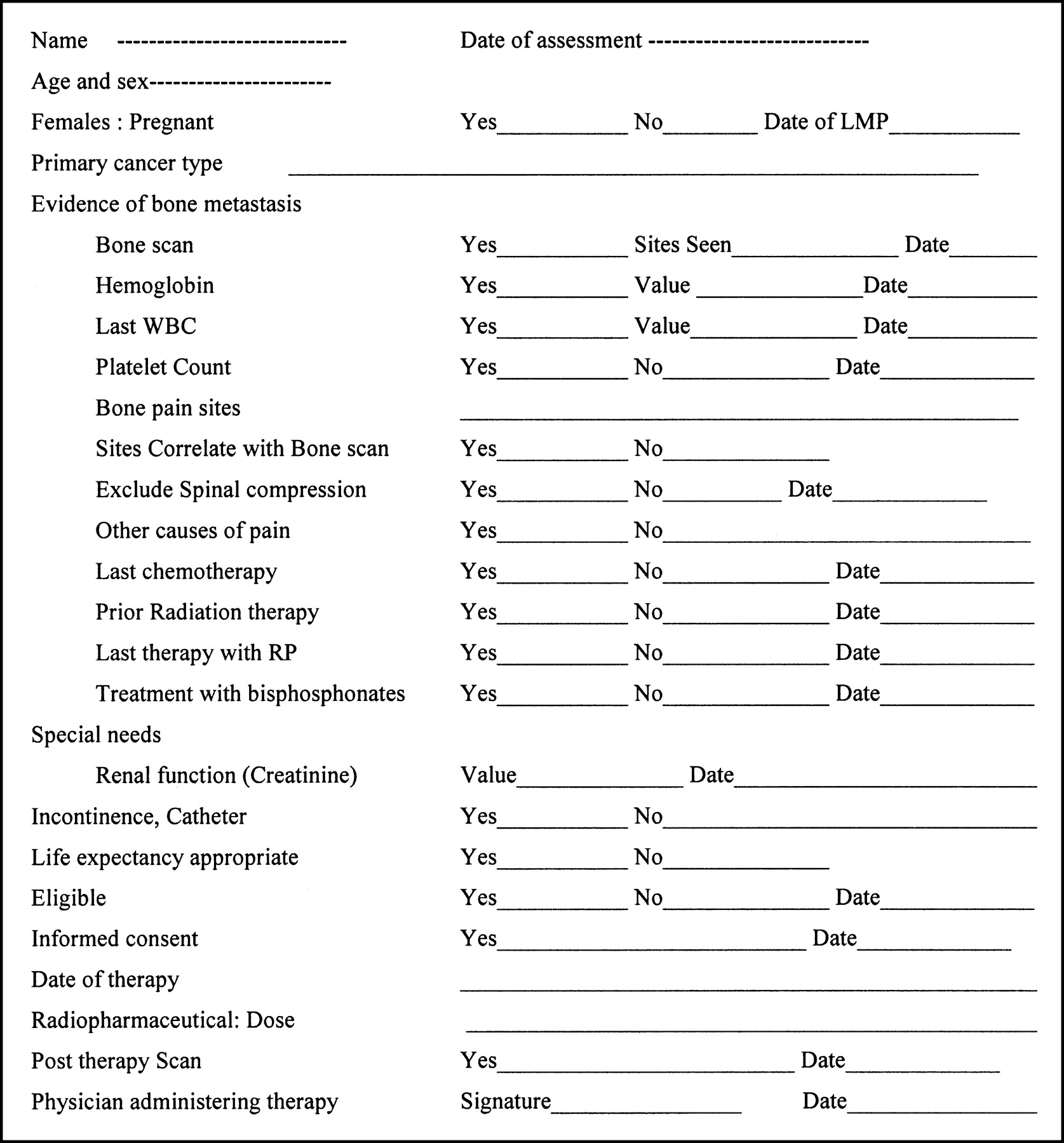
Worksheet for radiopharmaceutical therapy for bone pain. LMP = last menstrual period; WBC = white blood cell count; RP = radiopharmaceutical.
FOLLOW-UP
Patients are usually seen by their medical oncologist in follow-up. Blood counts are obtained at least weekly for the first 6 wk and more frequently if there is evidence of toxicity. A drop in counts may be seen by 2–4 wk after treatment. Blood counts, notably thrombocyte and neutrophil counts, should be obtained until all counts are normal; return to pretreatment baseline may not always occur. Patients whose blood counts do return to pretreatment values may be retreated, generally not before 3 mo.
In summary, bone pain palliation therapy with radiopharmaceuticals is a cost-effective systemic therapy to relieve pain from skeletal metastases with a consequent decrease in morbidity with an improvement in quality of life; use of bone-seeking radiopharmaceuticals, by themselves or as part of a multimodality regimen, may also reduce disease progression. It should be actively considered especially in patients with widespread metastasis. The ability to use this treatment with other therapies with added benefit is definitely an asset. Although single therapy has been shown to be effective especially in metastatic prostate cancer, repeat therapies should be carefully administered as the effect of such therapy on marrow reserve has not yet been completely elucidated.
Footnotes
Received Apr. 15, 2004; accepted Apr. 15, 2004.
For correspondence or reprints contact: Neeta Pandit-Taskar, MD, Nuclear Medicine Service, Memorial Sloan-Kettering Cancer Center, 1275 York Ave., New York, NY 10021.
E-mail: pandit-n{at}mskcc.org
↵* NOTE: FOR CE CREDIT, YOU CAN ACCESS THIS ACTIVITY THROUGH THE SNM WEB SITE (http://www.snm.org/ce_online) THROUGH AUGUST 2005.
REFERENCES





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Prostate Cancer, Version 1.2014
- Prostate Cancer
- Bone metastases from differentiated thyroid carcinoma
- High-Linear Energy Transfer Irradiation Targeted to Skeletal Metastases by the {alpha}-Emitter 223Ra: Adjuvant or Alternative to Conventional Modalities?
- {beta}2-Microglobulin Is a Signaling and Growth-Promoting Factor for Human Prostate Cancer Bone Metastasis.