


Abstract
Sympathetic cardiopulmonary nerves arise from the cervical sympathetic trunks and travel alongside the great arteries to innervate the ventricles. Because of the proximity of the nerve and artery, cardiac sympathetic denervation may occur in patients who have just undergone surgery for the repair of an ascending aortic aneurysm. Methods: To evaluate the cardiac sympathetic activity in aortic aneurysm, we performed cardiac 123I-metaiodobenzylguanidine (MIBG) imaging on 12 patients (mean age ± SD, 47 ± 17 y) before and after the surgical repair of an aneurysm. Seven patients scheduled for coronary artery bypass grafting also underwent 123I-MIBG imaging as controls for open-chest surgery. Planar images were obtained at 15 min (early) and 4 h (delayed) after injection of 111 MBq 123I-MIBG, and the cardiac 123I-MIBG uptake was graded quantitatively and visually. The quantitative evaluation was based on the heart-to-mediastinum ratio (H/M), and visual evaluation was performed by assigning a score of 0–3 (0 = absent, 1 = severely reduced, 2 = reduced, and 3 = normal). Heart rate variability using 24-h Holter electrocardiography was analyzed before and after the operation to generate a time-domain index of heart rate variability as an index of autonomic balance. Results: In patients with aortic aneurysms, both early and delayed H/Ms were significantly decreased after the operation (early H/M: 1.84 ± 0.16 before vs. 1.40 ± 0.16 after, P = 0.001; delayed H/M: 1.79 ± 0.38 before vs. 1.27 ± 0.18 after, P = 0.004). Visual analysis of 123I-MIBG accumulation in early images showed absence of 123I-MIBG accumulation in 3 of 12 patients, a score of 1 in 7 patients, and a score of 2 in 2 patients. In contrast, no significant difference between H/M before surgery and H/M after surgery was seen in patients who underwent coronary artery bypass grafting. The time-domain index of heart rate variability was significantly lower after the operation than before (135 ± 40 after vs. 96 ± 27 before, P < 0.05). Conclusion: Cardiac sympathetic nerves are totally or partially denervated after the surgical repair of ascending aortic aneurysm.
Sympathetic cardiopulmonary nerves arise from the cervical sympathetic trunks and travel alongside the great arteries to innervate the ventricles (1). A recently available norepinephrine analog, 123I-metaiodobenzylguanidine (MIBG), accumulates in the endings of sympathetic nerves through an uptake-1 mechanism and reflects cardiac sympathetic nervous function. Theoretically, mechanical interruption of the cardiac sympathetic nerves can be expected to reduce 123I-MIBG accumulation in the heart. In patients who undergo surgical correction of an ascending aortic aneurysm, such a reduction in 123I-MIBG accumulation can lead to cardiac sympathetic denervation. In transplanted hearts, the sympathetic neurons are severed from their nerve terminals, thereby depleting the norepinephrine reserves and producing complete cardiac denervation (2). Previous studies have reported that 123I-MIBG uptake is absent from transplanted human heart early (<1 y) after transplantation (3–5). The purpose of this study was to evaluate cardiac sympathetic nervous function early after surgical correction of ascending aortic aneurysm.
MATERIALS AND METHODS
Patients
Twelve patients (9 men, 3 women; age range, 26–72 y; mean age ± SD, 47 ± 17 y) with aortic aneurysms (dissecting aneurysms, annuloaortic ectasia with aortic regurgitation, and thoracic aneurysms) were enrolled in this study. None of the patients had significant coronary artery stenosis (luminal narrowing > 50%, as shown by coronary angiography), diabetes mellitus, systemic autonomic disease, or cardiomyopathy. Patients with major complications after the operation were excluded. For patients with annuloaortic ectasia and aortic regurgitation, the Bentall operation (repair of ascending aorta and replacement of aortic valve) was performed. The aorta was transected in all patients. Table 1 lists the clinical backgrounds, including preoperative diagnosis, operative method used, aortic cross-clamp time, cardiopulmonary bypass time, and total postoperative catecholamine dose and duration. Seven men (age range, 59–74 y; mean age, 64 ± 7.6 y) who were waiting for coronary artery bypass grafting (CABG) were also enrolled as control patients for open-chest surgery without aortic repair. The Institutional Committee on Human Clinical Investigations approved this study protocol. All patients were well informed of these procedures and consented to participate in this study.
Clinical Characteristics of Patients with Aortic Aneurysm
123I-MIBG Imaging
All patients underwent cardiac 123I-MIBG imaging within 1 mo before the operation and within 2 mo after the operation. After thyroid blockade with oral administration of 150 mg potassium iodide, anterior planar imaging was performed 15 min after (early imaging) and 4 h after (delayed imaging) injection of 111 MBq 123I-MIBG. Seven of the patients with aortic aneurysms underwent SPECT imaging. Imaging was performed using a single-head gamma camera (DS7; Sopha Medical, Buc, France) with a low-energy, high-resolution collimator. 123I-MIBG accumulation was visually graded as absent, severely reduced, reduced, or normal by 2 independent observers who were unaware of patient data. Global 123I-MIBG uptake was also assessed semiquantitatively by the heart-to-mediastinum ratio (H/M) as described in our previous study (6).
Analysis of Heart Rate Variability
Autonomic dysfunction was evaluated by heart rate variability (HRV) using 24-h electrocardiographic monitoring performed twice: once within 14 d before the operation and once within 14 d after the operation. Low frequency (0.05–0.15 Hz), high frequency (0.15–0.50 Hz), SDNN (SD of all normal-to-normal intervals), and SDANN (SD of the averages of normal-to-normal intervals in all 5-min segments of the entire recording) were used as time-domain indices of HRV. The patients with atrial fibrillation and frequent premature ventricular or atrial contraction were excluded from the analysis (7).
Statistical Analysis
All results are expressed as the mean values ± 1 SD. The Wilcoxon signed rank test was used to compare scintigraphic results and HRV values before and after the operation. The Mann-Whitney test was used to compare scintigraphic findings or clinical data in subgroups of patients. The Spearman rank correlation was used to compare the HRV value with scintigraphic results. Statistical significance was set at a probability value of 0.05. Multivariate stepwise regression was used to analyze whether age, aortic cross-clamp time, cardiopulmonary bypass time, total postoperative catecholamine dose, or duration of catecholamine dose was independently related to H/M.
RESULTS
123I-MIBG Scintigraphy
In patients with aortic aneurysms, 123I-MIBG imaging was performed 10 ± 9 d before (range, 3–31 d) and 27 ± 8 d after (range, 16–46 d) the operation. The reduction in cardiac 123I-MIBG uptake after the operation was marked in 3 patients and slight in 9 patients, as exemplified by the representative patients shown in Figures 1 and 2, respectively. Visual analysis of 123I-MIBG accumulation from early imaging after the operation showed 123I-MIBG to be absent in 3 patients, severely reduced in 7, and moderately reduced in 2. The same analysis performed on delayed imaging showed absence in 5, severe reduction in 6, and moderate reduction in 1. As shown in Figure 3, the H/M in both early and delayed images was confirmed to be significantly lower after the operation than before (early, P < 0.0001; delayed, P = 0.0004). The H/M was decreased after the operation in all patients but varied considerably, ranging from 1.10 to 1.68 in early images and from 1.01 to 1.77 in delayed images. The early H/M was 1.38 ± 0.19 in 6 patients who underwent replacement of both the ascending aorta and the total aortic arch and 1.42 ± 0.13 in 6 patients who underwent replacement of only the ascending aorta. No statistical difference in the early H/M was obtained between those 2 groups. Table 2 compares clinical parameters in the patients with no early uptake of 123I-MIBG (total denervation, n = 3) and clinical parameters in the other patients (partial denervation, n = 9). Among the parameters, cardiopulmonary bypass time and total catecholamine dose differed significantly between the 2 groups. Analysis of multivariate stepwise regression showed that cardiopulmonary bypass time (F = 4.57) and total catecholamine dose (F = 4.34) were independently related to early H/M after the operation (r = 0.77; P = 0.018).

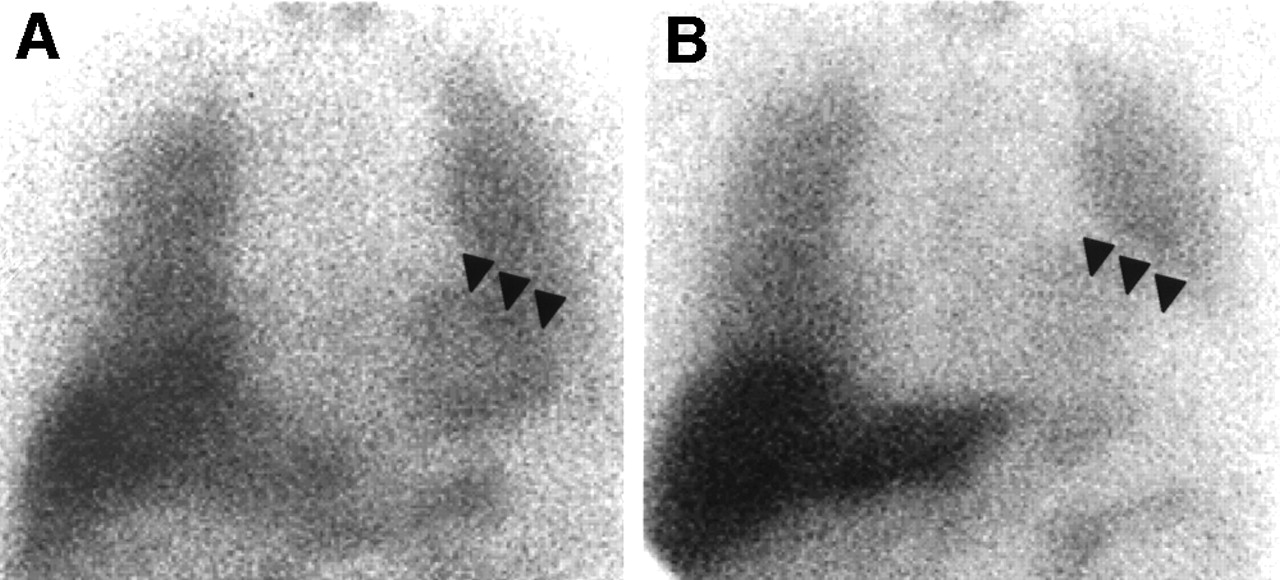
A 66-y-old man with thoracic aortic aneurysm from ascending aorta to total aortic arch. Ascending and total arch graft replacement was performed. (A) 123I-MIBG early image shows normal accumulation (arrowheads) in whole heart (H/M, 1.83) before operation. (B) One month after operation, MIGB accumulation is markedly decreased (H/M, 1.33).

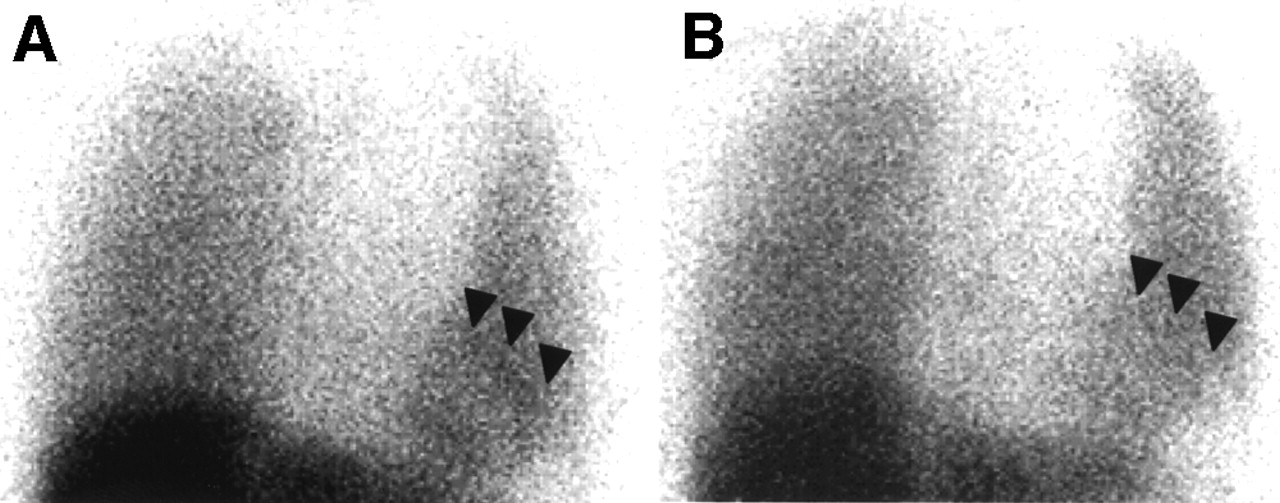
A 30-y-old man with thoracic aortic aneurysm from ascending aorta to total aortic arch. Ascending and total arch graft replacement was performed. (A) 123I-MIBG delayed image before operation shows normal accumulation (arrowheads) in whole heart (H/M, 1.92). (B) One month after operation, MIBG accumulation is slightly decreased (H/M, 1.68).
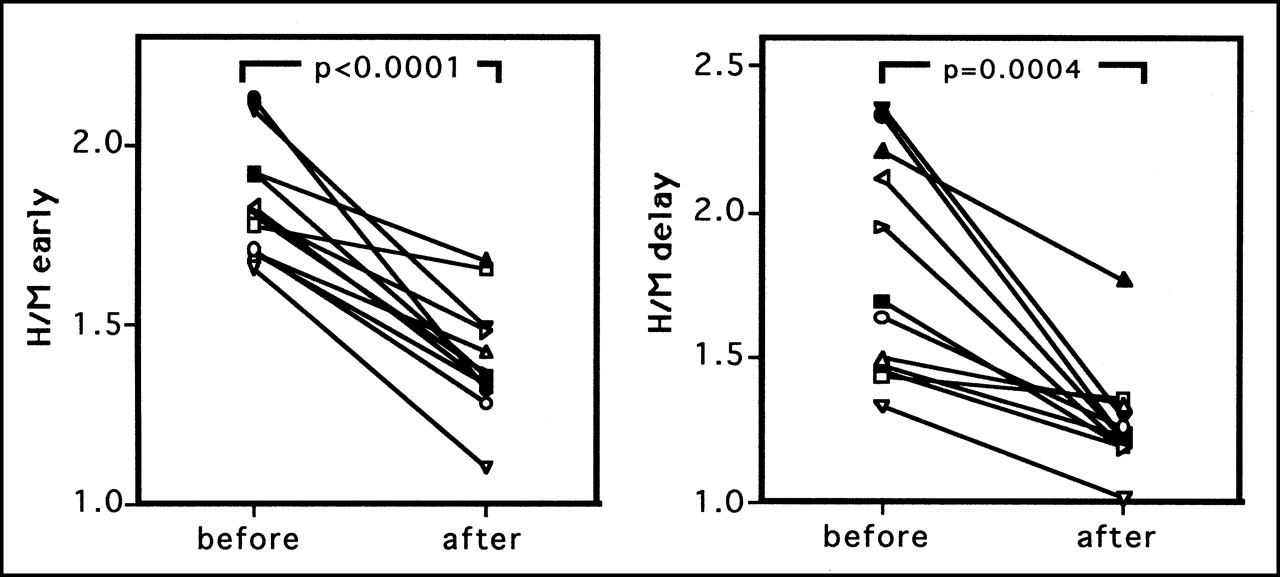
Changes in early (left) and delayed (right) H/Ms of 123I-MIBG before and after aortic replacement surgery. Both early and delayed images showed significant decrease in H/M after operation.
Comparison of Parameters Between Total and Partial Denervation
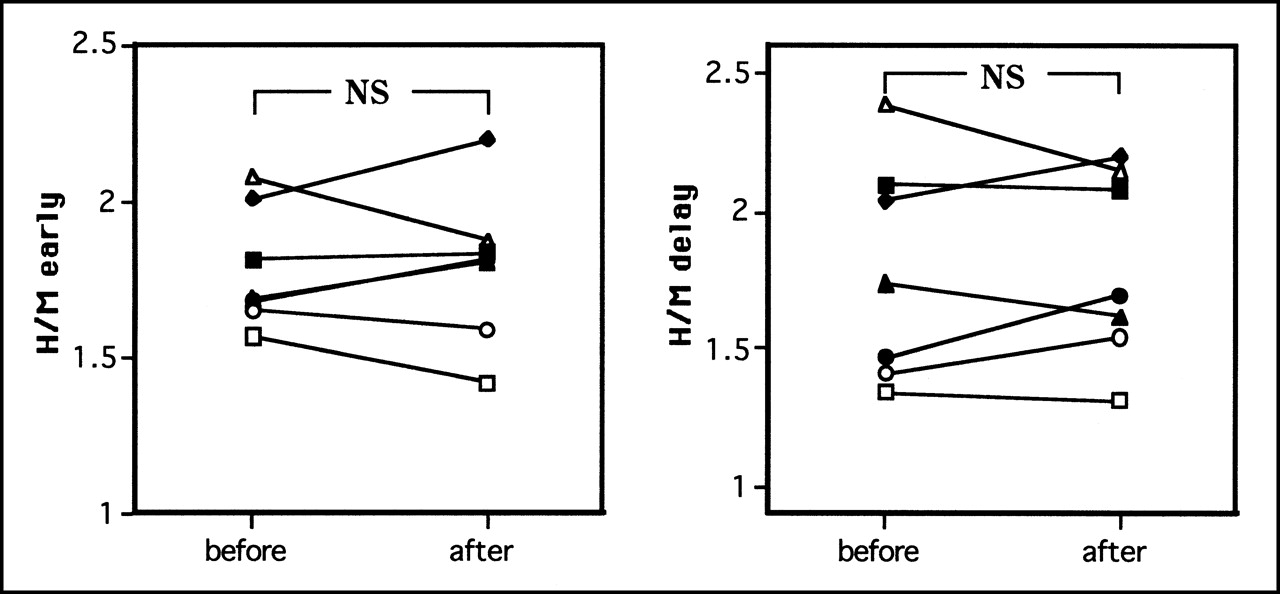
The early and delayed SPECT images after the operations in these patient groups indicated a global cardiac defect in 2 patients and inferoposterior and apical defects in 5 patients. In control patients with CABG, early and delayed H/Ms before the operation did not significantly differ from those after the operation (Fig. 4).
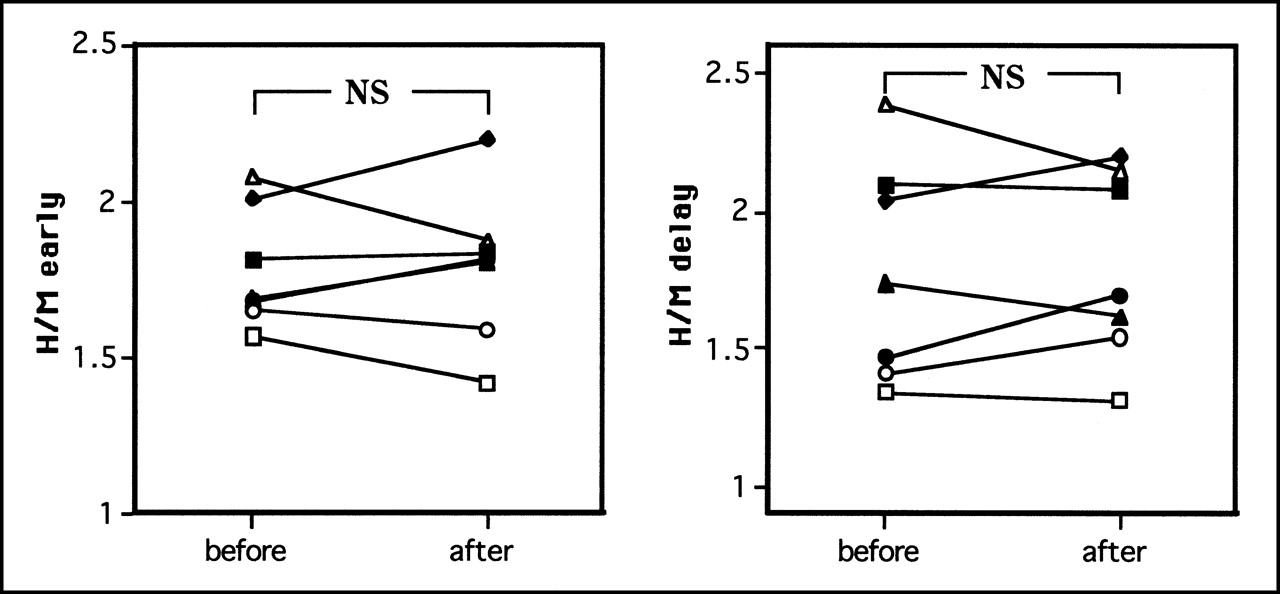
Changes in early (left) and delayed (right) H/Ms of 123I-MIBG before and after CABG. Both early and delayed images showed no significant difference between H/M before operation and H/M after operation.
HRV
HRV could be analyzed in only 6 of 12 patients because the other 6 patients had frequent arrhythmias such as premature atrial and ventricular beats or paroxysmal atrial fibrillation. Table 3 shows the HRV values of several variables: low frequency, high frequency, SDNN, and SDANN. Each variable was significantly decreased after the operation, but none of the HRV parameters correlated significantly with 123I MIBG uptake after the operation.
Changes in HRV Before and After Surgery for Repair of Ascending Aortic Aneurysm
DISCUSSION
Cardiac 123I-MIBG uptake is reduced under various pathologic conditions, such as cardiomyopathy (6,8), diabetic neuropathy (9), Parkinson’s disease (10), and mechanical sympathetic neuronal damage (3–5,11). In the cardiomyopathic heart, the main cause of reduced 123I-MIBG uptake is damage to local or diffuse sympathetic nerve terminals on the heart accompanied by myocardial degeneration. In diabetic neuropathy or Parkinson’s disease, on the other hand, systemic sympathetic neuronal damage involves cardiac sympathetic neurons, resulting in depressed 123I-MIBG uptake. Heart transplantation results in complete cardiac denervation because of the removal of all cardiopulmonary nerves. An arterial-switch operation for transposition of the great arteries also induces complete cardiac sympathetic denervation as determined by 123I-MIBG scintigraphy (11). Replacement of the ascending aorta inflicts some mechanical damage to the cardiopulmonary nerves surrounding the aorta. The results of this study indicated that cardiac sympathetic denervation occurred after surgical repair of the ascending aortic aneurysm in patients with thoracic aortic aneurysm or annuloaortic ectasia. In the control patients, 123I-MIBG uptake was not decreased after the operation, indicating that 123I-MIBG uptake has no influence on open-chest surgery using cardioplegia. Hence, reduced uptake after the operation is caused by interruption of the sympathetic nerves alongside the ascending aorta.
Three patients with aortic aneurysms showed complete denervation after the operation, but 9 others showed lower uptake but not complete absence. Because H/Ms did not significantly differ between the patients with repair of the aortic arch and ascending aorta and patients with repair of the ascending aorta only (i.e., H/M was not related to aortic cross-clamp time), the extent of the direct operative interruption could not explain the wide variation in postoperative cardiac 123I-MIBG uptake. In contrast, a longer cardiopulmonary bypass time and a greater postoperative total catecholamine dose reduced 123I-MIBG uptake in this study. We speculated that, among the patients with surgical repair of the ascending aorta, one of the parameters for operative invasion—cardiopulmonary bypass time—and catecholamines, which exert some direct toxic effects on sympathetic nerves (12), contributed to the additional cardiac denervation.
The lower delayed H/M in the patients with aortic regurgitation in this study was expected because volume-overloaded heart failure usually involves reduced delayed uptake and rapid washout of 123I-MIBG (13). Autonomic neuropathy or mechanical neuronal damage involves reduction of both early and delayed 123I-MIBG uptake, whereas depressed cardiac systolic function usually involves predominantly a reduction of delayed 123I-MIBG uptake. The reduction of delayed 123I-MIBG uptake is usually reversed after cardiac status improves in patients with congestive heart failure (14). However, the patients in this study showed further reductions in delayed H/M after aortic valve replacement in spite of their improved cardiac status. This finding supports the contention that cardiac denervation occurred in patients with surgical repair of aortic aneurysms. Hence, the difference between preoperative and postoperative H/Ms was more prominent in the early images than in the delayed ones, as shown in Figure 3.
SPECT images could reveal how the cardiac denervation occurred. The partially denervated hearts always involved apical as well as inferoposterior defects of 123I-MIBG—a finding similar to that in patients with diffusely autonomic dysfunction, such as that from diabetes mellitus (15) or Parkinson’s disease (16). The finding may stem from the interruption of not only the left cardiopulmonary nerves on the anterior surface of the aorta connecting to the right coronary nerves but also the dorsal plexus, including the right cardiopulmonary nerves behind the aorta connecting to the left coronary nerves (1).
HRV indices are generally reduced in patients with cardiac autonomic nervous dysfunction, such as occurs after heart transplantation (17) or from diabetic neuropathy (18). Patients who have recently undergone heart transplantation have a low HRV with no definite spectral components (19). The HRV indices in this study also indicated decreased sympathetic activity after the operation, but the extent of decrease from the preoperative level was limited (P = 0.05). A previous study reported that a reduction in the time-domain SDNN paralleled the severity of the disease in patients with myocardial infarction (20). The absence of any statistical difference in the correlation between HRV and 123I-MIBG uptake may have been caused by the small number of patients included in our HRV analysis.
Patients with aortic aneurysms have ischemic heart disease as a complication more frequently than do patients without aortic aneurysms (21). Because cardiac denervation has been reported to be associated with silent ischemia (9,22), patients should be carefully followed when this condition is detected. Further studies will focus on whether the prognosis is associated with the occurrence of complete denervation or whether reinnervation occurs in patients after undergoing thoracic aortic replacement.
CONCLUSION
We conclude that cardiac sympathetic nerves are totally or partially denervated after surgical repair of ascending aortic aneurysm and that, in addition to the surgical interruption of cardiopulmonary nerves surrounding the ascending aorta, the degree of denervation influences cardiopulmonary bypass time during the operation and total postoperative catecholamine dose. The clinical significance of the denervation remains unclear.
Footnotes
Received Dec. 12, 2000; revision accepted May 14, 2001.
For correspondence or reprints contact: Mitsuru Momose, MD, Nuklearmedizinische Klinik und Poliklinik der Technische Universität München, Klinikum rechts der Isar, Ismaninger Strasse 22, 81675 München, Germany.




{kind=link}
{kind=link}
{kind=link}
{kind=link}