


Abstract
The chemotactic cytokine interleukin-8 (IL-8) plays an important role in attraction and activation of polymorphonuclear leukocytes in infection and inflammation. A pilot study was conducted to determine if radiolabeled IL-8 would depict infection in humans. Methods: Human recombinant IL-8 (rhIL-8) labeled with 131I (specific activity, 0.4–0.7 MBq [11–18 μCi] 131I/μg IL-8) was injected intravenously into 8 diabetic patients with active foot infections and evidence of osteomyelitis, 2 patients with successfully treated osteomyelitis, and 1 patient with cellulitis of the thumb. Results: Focal accumulation of 131I-rhIL-8 was seen in 8 of 8 patients with active foot infection and diffuse uptake was seen in the thumb of the 1 patient with cellulitis. In the 2 patients with successfully treated bone infection, multiphase 99mTc-hydroxyethylene diphosphonate bone scans were negative early, but late-phase (>3 h) uptake depicted degenerative lesions that did not image with 131I-rhIL-8. Conclusion: 131I-rhIL-8 accumulates rapidly within infected foci in osteomyelitis and cellulitis but not in successfully treated infections or degenerative joint disease.
Interleukin-8 is a chemotactic cytokine that exhibits a high affinity for receptors on the plasma membranes of neutrophils (1,2). Cellular activation occurs after IL-8 binding in the presence of calcium and protein kinase, resulting in neutrophil activation and chemotaxis in infection and inflammation (2). IL-8 thus functions to mediate neutrophil recruitment, accumulation, and activation. We have previously shown that radiolabeled IL-8 rapidly images sterile abscesses in an animal model (3). In this article we describe the use of 131I-labeled human recombinant IL-8 (131I-rhIL-8) for the scintigraphic depiction of infection in humans.
Materials and Methods
Patients
Eight diabetic patients with documented, active foot infections and evidence of osteomyelitis and 2 diabetic patients with successfully treated osteomyelitis were selected for 131I-rhIL-8 imaging. The diagnosis of osteomyelitis was based on clinical, laboratory, and imaging studies including plain x-rays and multiphase bone scans (Tables 1 and 2). Each patient gave human experimentation committee–approved written, informed consent before administration of supersaturated potassium iodide solution (2 drops, 3 times per day) beginning 24 h before and continuing for 7 d after the intravenous injection of 37 MBq (1 mCi) 131I-rhIL-8. Blood samples were obtained immediately after 131I-rhIL-8 injection and at 0.5, 1, 2, 3, 6, 24, and 48 h later. Urine was collected between 1 and 24 h, 24 and 48 h, and 48 and 72 h after 131I-rhIL8 administration. Laboratory studies were performed to assess red and white cell counts (including differential cell counts), platelets, urea nitrogen, creatinine, serum electrolytes, calcium, phosphorous, alkaline phosphatase, alanine aminotransferase (ALT), lactate dehydrogenase (LDH), aspartate aminotransferase (AST), and bilirubin levels at multiple selected time points after 131I-rhIL-8 injection.
Clinical Findings in 11 Patients
IL-8 in Infection
Image Acquisition and Analysis
Whole-body and spot images were obtained using a gamma camera equipped with a high-energy, parallel-hole collimator and interfaced to a computer (Vertex; ADAC Corp., Milpitas, CA; or ZLC; Siemens Corp., Hoffman Estates, IL). A 20% window centered around the 364-keV photopeak of 131I was used to obtain images of 250,000–300,000 counts. All patients were scanned at 5, 30, 60, 120, 180, and 360 min; at 24 and 48 h, scans were obtained for the first 3 patients studied. Relative activity was determined by computer-assisted region of interest (ROI) analysis of areas of 131I accumulation and the background-corrected counts per pixel were plotted over the 24-h postinjection imaging interval. Multiphase bone scans were performed with 925 MBq (25 mCi) 99mTc-hydroxyethylene disphosphonate (99mTc-HDP) injected intravenously with blood-flow (6 s per frame × 20 frames), blood-pool (200,000 counts), and delayed images obtained at 2–3 h and, in some instances, at 24 h after injection.
Radiolabeling Procedures
rhIL-8 was obtained from Pepro Tech Inc. (Rocky Hill, NJ). 131I was purchased as NaI (480–630 MBq [13–17 mCi] per μg iodine) from Amersham Corp. (Arlington Heights, IL). Radioiodination of rhIL-8 was performed using previously described methods (3). Specific activity ranged from 0.4 to 0.7 MBq (11–18 μCi) 131I per μg IL-8. The chemotactic activity of the product was assayed using purified human neutrophils as responder cells and nonlabeled IL-8 as a chemotaxis standard (3).
Results
Clearance of 131I-rhIL-8
A biexponential, rapid fall of blood 131I levels was seen after injection of 131I-rhIL-8. There was an initial phase within the first 50 min (half-life, 5.3 min) and a second phase with a half-life of 6.6 h (Fig. 1A). The activity of 131I-rhIL-8 was equally divided between plasma and red blood cells (RBCs) in blood. Cumulative urinary clearance of 131I radioactivity (±SD) was 59.0 ± 13.7 percentage injected dose at 72 h (Fig. 1B).
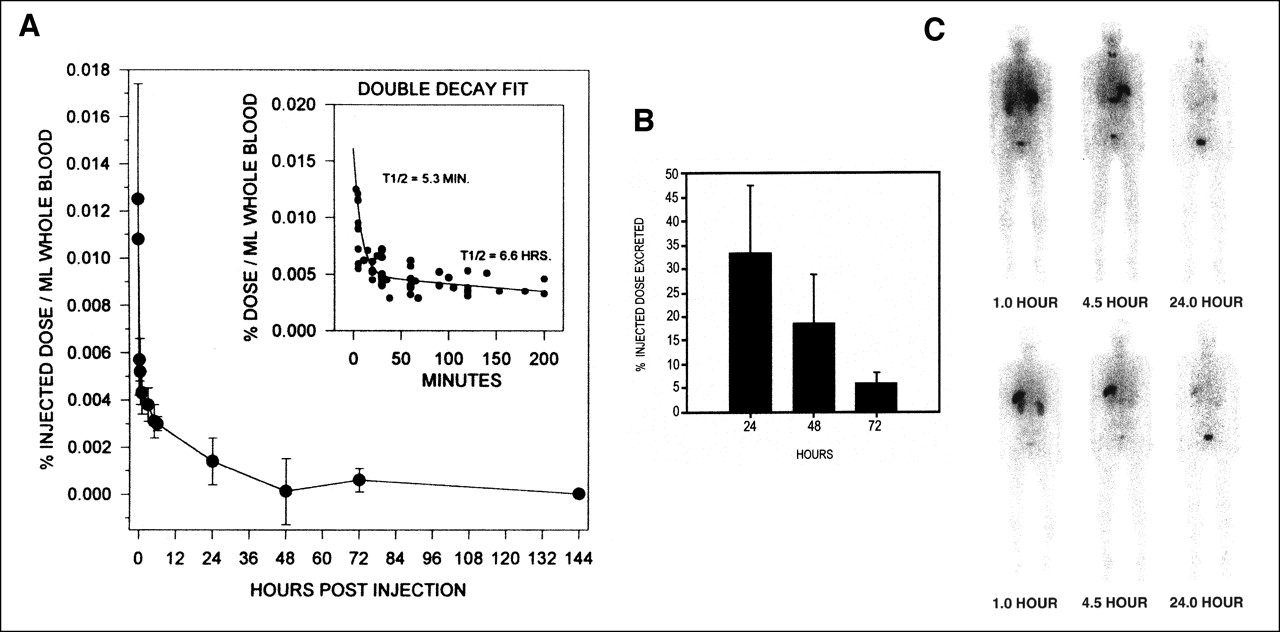
Blood clearance of 131I-rhIL-8 (A), urinary excretion of 131I radioactivity (B), and anterior (top row) and posterior (bottom row) body images over 24-h interval show faint uptake in lungs and prominent accumulation in spleen with discernable activity in small bowel, kidneys, and bladder (C). T1/2 = half-life.
Effect of 131I-rhIL-8 on Laboratory Values
White blood cell (WBC) counts fell briefly in 6 of the 11 patients (mean decrease, 600 cells per mm3; decrease range, 200–1,000 cells per mm3) after rhIL-8 injection. In all but 2 patients, WBC levels returned to baseline (patient 1, 7,200 vs. 7,500 [baseline] cells per m3; patient 2, 6,000 vs. 7,000 [baseline] cells per m3) by 60 min. No differences were noted from baseline in levels of RBC, platelets, urea nitrogen, creatinine, serum electrolytes, calcium, phosphorous, alkaline phosphatase, ALT, AST, LDH, or serum bilirubin after 131I-rhIL-8 injection.
131I-rhIL-8 Imaging of Human Infection
Accumulation of 131I radioactivity was seen in nasal and oropharyngeal areas of the head and neck. Uptake was also seen in the stomach, spleen, and bladder. Faint, transient, early lung uptake was also seen after injection. The distribution of 131I radioactivity changed little over a 24-h imaging interval (Fig. 1C). Focal accumulation was seen in the areas of foot infection in the 8 patients with confirmed osteomyelitis (Fig. 2A). The intensity of uptake appeared to be related to the duration of infection, with the most acute infections showing the most prominent accumulation of 131I activity (Fig. 2B). ROI analysis of the areas of infection showed a progressive increase of 131I radioactivity that peaked between 3 and 6 h after 131I-rhIL-8 injection. In 2 patients with successfully treated osteomyelitis, there was no 131I accumulation in either of the areas of prior infection. There was also no 131I accumulation in the 1 patient with degenerative joint disease of the foot identified on the 3-h delayed images of a multiphase bone scan (Figs. 2C and 2D). Acute cellulitis of the thumb after a rose thorn puncture wound was depicted as diffuse uptake of 131I-rhIL-8.

Focal uptake of 131I-rhIL-8 in acute infection of left foot (A), less intense but focal 131I-rhIL-8 uptake (arrow) in patient with chronic infection in foot (B), 3-h delayed 99mTc-HDP bone scan shows multifocal degenerative changes in ankles and feet in patient with chronic infection (arrow) of right foot (C) and corresponding 131I-rhIL-8 images depict infection (arrow) but do not image extensive degenerative arthritis (D).
Discussion
IL-8 is 1 of >40 chemotactic cytokines that act to induce neutrophil and other WBC activation and migration (1,2). Secretion of certain cytokines results in the selective recruitment of neutrophils into infected or inflamed tissues (1,2). In earlier studies, it has been shown that radioiodinated IL-8 will localize sterile and infected abscesses in animal models (3,4). In this study, we have shown that radiolabeled IL-8 successfully depicts infections in 8 of 8 patients with active foot infection and osteomyelitis documented by routine clinical, laboratory, radiographic, and multiphase bone scans. Accumulation of 131I-rhIL-8 was rapid with discernable depiction of infection as early as 3 h after injection. The physical properties of 131I limit spatial resolution for small structures such as foot bones, but the intense uptake in these infected feet was encouraging. Clearly, better resolution to separate soft tissue from bony infection might be achieved with a 123I or 99mTc radiolabel. Blood 131I radioactivity fell rapidly with uptake in the stomach, most likely reflecting deiodination. The fact that blood-pool activity did not appear to hamper imaging and uptake of IL-8 into sites of known infection was indicative of the rapid clearance and mechanism of local IL-8 receptor binding and activation of neutrophils (1,2). Splenic uptake is in keeping with the observation that IL-8 binds to erythrocytes, although in our studies and those of others, blood-pool activity does not appear to interfere with 131I-rhIL-8 imaging (3,4). Furthermore, the lack of accumulation of IL-8 in areas of degenerative joint disease confirmed previous studies that have shown a specific receptor-mediated mechanism for localization of 131I-rhIL-8 (3).
There were no significant side effects from 131I-rhIL-8. Peripheral WBC counts fell slightly in 6 patients (mean, 4% decrease; range, 3%–14%) after IL-8 injection at doses of 1μg/kg. When they occurred, the fall in peripheral WBC counts was small, transient, and unaccompanied by any observable untoward effects. At doses 10-fold greater than those administered in this study, a biphasic neutrophil response has been described with a fall of WBC at 30 s after IL-8 administration to <10% of baseline followed by a return to baseline levels within 15 min (5). Our findings also confirmed the absence of hemodynamic changes after bolus (10 μg/kg) or constant infusion of IL-8 in baboons (5).
These data confirm, in humans, the findings of our initial animal studies (3) and the studies of others (4) that radiolabeled IL-8 can be used to depict foci of infection. van der Laken et al. (4) have shown early scintigraphic localization of radiolabeled IL-8 in rabbits with focal infections induced by Escherichia coli and Staphylococcus aureus. In these models, early localization of tracer has been shown with high target-to-nontarget radioactivity ratios, especially in studies using infected abscess models (4).
This study was not undertaken to formally evaluate efficacy of 131I-rIL-8 for the localization of osteomyelitis or in infection detection in humans but rather to provide pilot biodistribution data (under radioactive drug research committee approval) in one example of human infection to determine if such a trial is warranted. On the basis of the data now available, we believe that a trial is warranted, although a smaller peptide fragment of IL-8 or a related cytokine, perhaps labeled with a metal chelate of either indium or technetium, may be preferable to an iodinated cytokine or cytokine analog as an optimal diagnostic imaging agent.
Conclusion
In this preliminary study, we showed that 131I-rhIL-8 depicts acute infection in humans, confirming studies in animals. However, the mechanisms of localization and the clinical value of IL-8 in the diagnostic evaluation of either infection or inflammation in humans have yet to be established.
Footnotes
Received Feb. 7, 2001; revision accepted Jul. 10, 2001.
For correspondence or reprints contact: Milton D. Gross, MD, Nuclear Medicine Service (115), Department of Veterans Affairs Health System, 2215 Fuller Rd., Ann Arbor, MI 48105.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Exploratory Randomised Trial of Tranexamic Acid to Decrease Postoperative Delirium in Adults Undergoing Lumbar Fusion: A trial stopped early
- In Vivo Leukocyte Labeling: The Quest Continues
- 99mTc-Labeled Interleukin 8 for the Scintigraphic Detection of Infection and Inflammation: First Clinical Evaluation
- Kinetics of 99mTc-Labeled Interleukin-8 in Experimental Inflammation and Infection
- Labeling Method Largely Affects the Imaging Potential of Interleukin-8