


Abstract
The aim of this trial was to evaluate in developing countries from different regions the diagnostic performance of 99mTc-sestamibi scintimammography (SM) in palpable breast lesions and to verify the clinical usefulness of a joint evaluation with mammography and SM. Methods: From 10 countries, a total of 238 patients with palpable breast masses (n = 245) were included in this prospective multicenter trial. Prone SM was performed 10 min and 60–90 min (157 patients) after injection using an isotime acquisition of 10 min. Mammography was assessed by the same dedicated imaging radiologist according to breast imaging reporting and data system (BI-RADS) categories for malignancy and breast density. Masked SM findings and mammography findings were checked for a correlation with histopathology findings for excisional biopsy samples. Diagnostic values for breast cancer detection were calculated per lesion. Results: Histopathology revealed 189 cancerous lesions and 56 benign lesions. The sensitivity and specificity of SM were 0.83 and 0.77, respectively. SM diagnostic values did not depend on the incidence of breast cancer in the country of origin or on the timing of imaging (early vs. delayed scans). On mammography, the technique yielded a sensitivity and specificity of 0.85 and 0.66, with 27 mammograms classified as BI-RADS category 1, 33 as category 2, 5 as category 3, 56 as category 4, and 124 as category 5. Thirty-seven lesions were considered to show increased radiologic density. No significant difference was found in SM diagnostic values among different BI-RADS categories or between the groups with low and high breast density. A sensitivity of 96% was calculated when SM and mammography results were combined, with 75% of all false-negative mammography findings classified as true-positive results by SM. Conclusion: SM complements mammography in patients with palpable masses and negative mammography findings.
Breast cancer is by far the most common malignancy among women worldwide, and 41% of all new cases are diagnosed in developing countries (1). In these countries, 323,000 cases were detected in 1990, leading to 140,000 deaths (1,2). Furthermore, as the population increases and ages, the number of new cases in these countries is expected to increase dramatically (3).
Mammography represents the only validated imaging technique for breast cancer screening. Several randomized controlled trials have reported about a 30% mortality reduction in women older than 50 y using this procedure (4). However, the technique is less reliable for detecting lesions in women younger than 50 y, in whom dense, glandular breasts are a common radiographic finding, yielding a false-negative rate of 25%–45% (5). Therefore, frequent delays in the diagnosis of breast cancer are seen in this group and are associated with significantly shorter survival (6). Furthermore, the positive predictive value of mammography is reported to be <40% (7), resulting in many unnecessary biopsies.
Since the publication of the encouraging results of Khalkhali et al. (8) for 99mTc-sestamibi scintimammography (SM), several investigators have reported on the clinical value of the technique and its possible complementary role to mammography for the evaluation of primary breast cancer (9–12). One of the proposed clinical indications for SM was palpable masses not clearly seen or classified as indeterminate or benign on mammography (10,11). Therefore, a multicenter trial sponsored by the International Atomic Energy Agency was set up to evaluate—in developing countries from different geographic regions—the diagnostic values of SM in palpable breast lesions and the clinical usefulness of an imaging protocol based on the joint application of mammography and SM.
MATERIALS AND METHODS
Trial Design and Patients
The study was organized as a prospective open-label multicenter trial. To be included, a patient had to be a nonpregnant woman who had given informed consent and who had a palpable breast lesion as determined by an experienced surgeon, mammograms obtained within 4 wk of SM, and a histopathologic report on an excisional biopsy specimen. Exclusion criteria included previous surgery for a palpable breast lesion, fine-needle biopsy within 1 wk before SM or core biopsy during the preceding 4 wk, prior chemo- or radiotherapy, and lack of a histopathologic report. We received data for 346 patients from 10 countries in Africa, Asia, Europe, Latin America, and the Middle East: Chile (n = 44), China (n = 36), Colombia (n = 39), Cuba (n = 16), Greece (n = 42), India (n = 23), Peru (n = 44), Tanzania (n = 13), Turkey (n = 52), and Uruguay (n = 37). The age-standardized annual incidence rates of breast cancer, as estimated in 1990 (1), in participating countries is summarized in Table 1 and ranges from 11.77 (China) to 87.59 (Uruguay), with a median of 29.19.
Age-Standardized Annual Incidence Rates of Breast Cancer in Participating Countries
The efficacy population of the trial consisted of 238 patients (245 lesions, 7 patients with bilateral tumors), after 108 patients were excluded because of inappropriate scintigraphy technique (n = 14), lack of mammograms (n = 49), incomplete mammograms with a recommendation for additional imaging (n = 8), lack of tissue diagnosis (n = 20), or nonpalpable lesions (n = 17).
The median age of the patients was 50 y (range, 19–84 y). In 12% of patients, a family history of breast cancer was documented. Oral contraceptives and hormone replacement therapy had been used in 16% and 8% of patients, respectively. Prior surgery for cancer of the contralateral breast had been performed on 4% of patients. Pre-, peri-, and postmenopausal status was present in 41%, 7%, and 52% of patients, respectively.
SM
Labeling and quality control of 99mTc-sestamibi were performed according to the manufacturer’s instructions (DuPont Pharmaceuticals Co., Billerica, MA). The radiochemical purity of the radiopharmaceutical was always ≥90%.
99mTc-sestamibi was injected through an indwelling catheter into the arm contralateral to the palpable breast lesion, and the catheter was then flushed with 10 mL saline. In patients with bilateral lesions, the injection was into a dorsal vein of the foot. The dose ranged from 740 to 1,110 MBq (20–30 mCi).
Planar scanning was started 10 min after injection of the tracer, beginning with the affected breast. Lateral views were acquired with the patient lying prone, using a commercially available pad set (Pinestar Technology, Greenville, PA) designed to support the patient’s head, shoulders, and arms, allowing the imaged breast to depend while compressing the opposite breast. An anterior thoracic view including both axillae was also obtained while the patient was supine with her arms raised behind her head. Delayed imaging, 60–90 min after injection, was performed on 157 patients (160 lesions). Images were acquired on a 256 × 256 matrix, using a 10% window centered on an energy peak of 140 keV. We used an isotime acquisition of 10 min for each view. A low-energy high-resolution collimated gamma camera was used, with appropriate zooming for lateral views to include axillae, breast, and chest wall. The distance between the breast and the detector was minimized.
Mammography
For all patients, mammography was performed using craniocaudal and mediolateral oblique views. Mammograms were sent to a core-center dedicated breast-imaging radiologist, who evaluated them according to the breast imaging reporting and data system (BI-RADS) developed by the American College of Radiology (Reston, VA) (13). The radiologist was unaware of histopathology and SM findings, but physical examination data were available to him. Mammograms were considered positive for malignancy if the BI-RADS score was ≥4. When additional imaging was recommended, patients were scored as BI-RADS category 0 and excluded from the efficacy population (n = 8). Breast density was also scored according to the BI-RADS system, with 1 = entirely fatty, 2 = fatty with scattered fibroglandular tissue, 3 = heterogeneously dense, and 4 = extremely dense (13). Increased radiologic density was documented for patients with scores of 3 or 4.
Masked Interpretation of SM
The SM films were read by 2 independent, experienced nuclear medicine physicians who were unaware of the clinical status of the patient, physical examination findings, mammography findings, and histopathologic results. Initial and delayed images were scored separately by the readers, who did not know whether the images were from the same patient. However, only the information from the early views was used for comparison with other methods. For each lesion, a maximum of 4 images was evaluated: initial and delayed in lateral and anterior projections.
All studies were displayed as hard-copy films for analysis. A positive result for malignancy was defined as 1 or more focal areas of increased breast uptake regardless of intensity. Disagreements between readers were resolved by consensus, with a third experienced observer used as a referee. The assessors also scored the images for quality and excluded scans considered technically inadequate (n = 14).
Histopathology
All patients underwent excisional biopsy, with final diagnosis performed by the institutional pathologist. The largest dimension of the tumor was considered the pathologic size. If 2 or more lesions were excised from the same breast, the size of the larger was used for staging. However, every palpable lesion was correlated with SM and mammography findings.
Data Analysis
Data were collected on case report forms, entered into a database, and converted to appropriate software datasets for analysis. Agreement between either imaging technique—SM or mammography—and histopathology was assessed on a 2 × 2 table, which was the gold standard. Sensitivity, specificity, and their corresponding 95% confidence intervals (CIs) were calculated with InStat (version 3.01; GraphPad Software, Inc., San Diego, CA) for Windows 95 (Microsoft, Redmond, WA). This software was also used for performing the Fisher exact test to compare SM results in different subsamples. Group differences were considered significant at P < 0.05.
The probability of breast cancer given the result of SM or mammography was calculated using Arcus Quickstat (version 1.2; Longman Software Publishing, Cambridge, U.K.) for Windows 95 as follows: LRpos = sensitivity/1 − specificity, where LRpos is the likelihood ratio of a positive test, and LRneg = 1 − sensitivity/specificity, where LRneg is the likelihood ratio of a negative test. The corresponding 95% CIs were also estimated. To assess the performance of the technique in the same patient sample, we compared paired proportions—sensitivity and specificity—with Arcus Quickstat, using the McNemar test with Liddell correction. Interreader agreement for evaluation of SM scans was quantified with the same software using the κ statistic. Mammography and SM findings were also classified on a 4 × 4 table indicating false-negative, false-positive, true-negative, and true-positive results.
RESULTS
Histopathology
Histologic examination revealed 189 malignant lesions and 56 benign lesions (23%). Among the first group, there were 160 invasive ductal carcinomas, 13 invasive lobular carcinomas, 4 ductal carcinomas in situ, 4 tubular carcinomas, 3 mucinous cancers, 2 papillary carcinomas, 1 medullary carcinoma, 1 malignant cystosarcoma phylloides, and 1 sarcoma. The benign lesions included 28 fibroadenomas (4 corresponded to lesions > 30 mm in premenopausal patients), 13 fibrocystic changes, 6 inflammatory lesions, 4 cases of scleradenosis, 3 papillomas, 1 hamartoma, and 1 lipoma. The sizes of tumors ranged from 7 to 80 mm, with a median of 25 mm.
Masked Interpretation of SM
SM was true-positive for 157 of 189 malignant lesions and true-negative for 43 of 56 benign lesions. Sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio are presented in Table 2. Of the 32 false-negative results, we found 22 invasive ductal carcinomas, 3 lobular invasive carcinomas, 3 ductal carcinomas in situ, 1 mucinous carcinoma, 1 papillary carcinoma, 1 cystosarcoma phylloides, and 1 sarcoma. The median lesion size in this group was 18 mm, with a range of 10–50 mm. Six (19%) of 32 tumors were >30 mm. The false-positive results were obtained for 6 fibroadenomas, including the 4 lesions > 30 mm; 3 papillomas; 2 fibrocystic lesions; 1 case of mastitis; and 1 case of scleradenosis.
Diagnostic Results for SM and Mammography
Overall agreement between masked readers for all breasts was 91%, with a κ value of 0.79 and a 95% CI of 0.67–0.92.
We grouped the results of the masked interpretation according to countries with a higher incidence of breast cancer (Chile, Cuba, Greece, Peru, and Uruguay) and countries with a lower incidence of breast cancer (China, Colombia, India, Tanzania, and Turkey), as shown in Table 3 (1). Differences in diagnostic values between groups were not statistically significant.
Diagnostic Results for SM According to Breast Cancer Incidence in Country of Origin
Time of Imaging
A double-phase technique performed on 160 lesions yielded a sensitivity and specificity of 0.82 (95% CI, 0.74–0.88) and 0.80 (95% CI, 0.61–0.92), respectively, for early images and 0.79 (95% CI, 0.70–0.85) and 0.80 (95% CI, 0.61–0.92), respectively, for delayed images. No significant differences in diagnostic results between early and delayed images were observed.
Mammography
Mammography results were true-positive for 161 of 189 malignant lesions and true-negative for 37 of 56 benign lesions. The sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio are presented in Table 2. Among false-negative mammograms, 23 (82%) of 28 were in premenopausal women.
Table 4 summarizes SM findings according to BI-RADS category, with categories 2 (33 lesions) and 3 (5 lesions) grouped. Differences between values were not statistically significant.
SM Diagnostic Values with Respect to BI-RADS Mammography Category
Thirty-seven mammograms (15%) were considered to show increased radiologic density (34 were scored as category 3 and 3 as category 4). The remaining 208 mammograms were considered to show low radiologic density (56 were scored as category 1 and 152 as category 2). Sensitivity and specificity are presented in Table 5. No significant differences between diagnostic values were found.
SM Results with Respect to Radiologic Density of Breast Tissue
When mammography and masked interpretation of SM were compared, 21 malignant lesions classified true-positive by SM had been classified false-negative by mammography (Table 6). Hence, for 75% of all false-negative mammograms, SM correctly identified cancer, leading to a sensitivity of 96% when the results of SM and mammography were combined (Figs. 1 and 2). These 21 lesions were studied in 8 participating centers; 11 lesions were from the higher incidence group of countries, and the remaining 10 were from the lower incidence group. In 9 (43%) of these 21 cases of cancer, mammography showed dense breast tissue, and 17 (81%) of the patients were premenopausal.

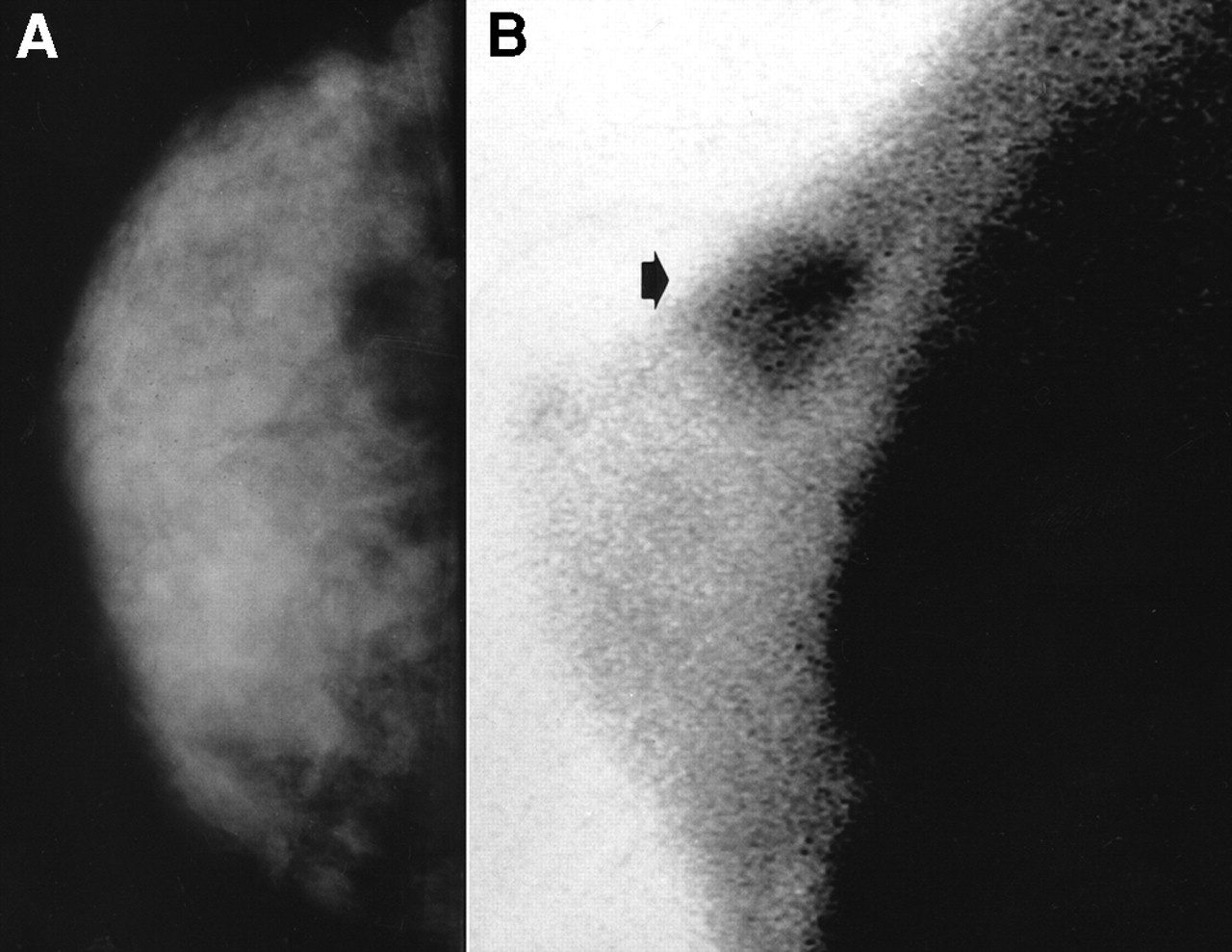
A 46-y-old premenopausal patient with palpable lesion of right breast. (A) Craniocaudal mammogram shows fibroglandular tissue without significant abnormalities (BI-RADS 1). (B) SM shows focal tracer accumulation in breast (long arrow) and axillary region (short arrow). Histopathologic examination found invasive ductal carcinoma, with 2 metastatic lymph nodes of 16 examined.
Comparison of Results for Masked SM and Mammography
DISCUSSION
SM has emerged in the last few years as a new procedure for the evaluation of patients with suspected breast cancer (9–12). However, the low sensitivity documented for the detection of nonpalpable tumors appears to be the major drawback of the procedure (10,14,15). In this trial, masked interpretation of SM resulted in a sensitivity of 0.83, which is similar to that reported for palpable lesions by the European multicenter trial (10) and by other investigators such as Kao et al. (9), Prats et al. (11), and Danielsson et al. (12). Recently, Khalkhali et al. (14) reported a sensitivity of 0.75–0.76 for palpable breast lesions in a masked study of a population with 48.4% disease prevalence.
The diagnostic performance of SM increases with tumor size, with most false-negative results being attributed to a lesion size < 10 mm (16,17). In our series, false-negative findings occurred for tumors with a smaller median size than that of the whole population; however, 19% of them were larger than 30 mm. This fact could be related to tumor overexpression of the multidrug resistance gene or to lesions with low desmoplastic activity or cellular proliferation (18,19).
The specificity of SM in this study was 0.77, which is similar to that obtained by Prats et al. (11) and by Palmedo et al. (10). However, the relatively wide 95% CI can be attributed to the low prevalence (23%) of benign lesions in our series of patients, which included only those with palpable masses. Therefore, a higher proportion of cancer is expected from the study sample. Nevertheless, patient referral bias from the reference centers of participating countries could also have contributed to the observed low prevalence of benign disease, because 6 of 10 centers included patients from national reference oncology departments. The false-positive results occurred for 6 cases of fibroadenoma, all 3 papilloma lesions, 2 fibrocystic lesions, 1 case of mastitis, and 1 case of scleradenosis. Highly mitotic juvenile fibroadenomas, hyperproliferative lesions associated with atypia, and inflammatory disorders had been considered potential sources of false-positive results by several investigators (7,11). However, in our series, only 1 of 6 patients with inflammatory breast lesions had a false-positive result. In our experience, inflammatory lesions can be distinguished from malignant tumors because the former take up tracer in a diffuse pattern that frequently involves the whole breast. Nevertheless, although not observed in the current sample, a malignant lesion involving the whole breast has the potential of showing diffuse sestamibi accumulation. Concerning the false-positive findings in cases of large fibroadenoma, our results agree with those of Prats et al. In this group of lesions, all fibroadenomas with sizes > 30 mm were classified as false-positive by SM.
Diagnostic values of SM were similar in the group of countries with a lower incidence of breast cancer and the group with a higher incidence. Therefore, SM results seemed to be independent of population characteristics such as ethnicity and breast cancer incidence.
When imaging timing was considered, SM results were almost identical in the early and delayed phases of the study. For this reason, we agree with Khalkhali et al. (14) in recommending early scintigraphic imaging for the evaluation of malignancy in patients with primary breast tumors.
We did not find a significant difference in diagnostic values between mammography and SM. This finding is comparable to that published by Cwikla et al. (20) for a patient population with suspected breast cancer.
Although it has been proved that mammography is highly sensitive for the detection of clinically occult breast cancer (4), the overall sensitivity of the technique for palpable breast cancer has been reported to be <0.83 (21–24). This value agrees with our observed sensitivity of 0.85. Thus, normal mammography findings cannot exclude cancer when it is clinically suspected. Furthermore, although placing breast lesions into BI-RADS categories is useful for standardizing the terminology in the mammography report, this classification is not suitable for ruling out malignancy in the nonscreening context of patients with palpable breast lesions. Therefore, cancer incidence in BI-RADS categories 1–3 estimated in this trial was 43%, which compares with a value of <4% obtained in a nonsymptomatic population (13). Besides, the high frequency of premenopausal women (82%) among patients with false-negative mammography findings may also contribute to the observed cancer incidence in the group scored as BI-RADS 1–3. The sensitivity of mammography is well known to be lower for premenopausal patients with palpable lesions than for postmenopausal patients (23). Even though specificity was lower for mammography than for SM—0.66 versus 0.77—the difference was not statistically significant because the small number of benign lesions in the trial created a relatively high degree of uncertainty in the specificity estimation. Khalkhali et al. (14) also found a lower specificity for mammography than for SM in their population with palpable abnormalities.
When the sensitivity of SM was compared with the BI-RADS classification of mammography, we did not find any significant differences among categories. Therefore, the mammographic patterns of malignancy appeared to be independent of sestamibi uptake. Moreover, we showed SM to have comparable diagnostic accuracy in patients with high radiologic breast density and in patients with nondense breasts. Similar results were reported by Khalkhali et al. (25) and by Mulero et al. (26).
This trial showed that for 75% of patients with false-negative mammography findings, scintigraphy was able to identify a breast carcinoma. This group of patients contained a relatively high number that were premenopausal and had radiologically dense breasts, and the patients were from 8 participating countries with differing incidences of breast cancer (48% of the low-incidence group). Consequently, SM has the potential to reduce the number of false-negative mammography findings in younger women with dense breasts, for whom mammography has been proven to have significant limitations (5). Palmedo et al. (10), from the European trial, also found positive SM findings in 60% of patients with false-negative mammography findings. That report proposed a diagnostic protocol in which SM could be used jointly with mammography to evaluate patients with palpable breast lesions and indeterminate mammography findings. A similar protocol was proposed by Prats et al. (11), who also included scintigraphic evaluation of patients with palpable lesions (>1 cm) and mammography findings indicating a low probability of malignancy.
By general agreement, when factors (e.g., age < 40 y and dense breasts) that can produce false-negative mammography results are present in patients with palpable breast lesions, the patients may be targeted for further investigation by other modalities such as sonography and fine-needle aspiration biopsy (FNAB) (23,27). We believe that, to be included in a diagnostic protocol for palpable breast lesions, SM should have a diagnostic impact comparable with that of the nonnuclear techniques, especially in populations with a high incidence of breast cancer. In our study, adding SM to mammography increased the sensitivity for detection of breast carcinoma to 96%. The term triple diagnosis refers to a combination of clinical breast examination, mammography, and FNAB. The systematic use of such a diagnostic protocol has been recommended because its sensitivity is in the range of 93%–95% (12,28). Furthermore, when all 3 tests indicate that a lesion is benign, the probability of diagnostic error has been shown to be <1% (27). Cost analysis revealed that this diagnostic strategy could yield an important average per-case savings compared with routine confirmatory open biopsy (29). However, successful FNAB requires that the clinician be experienced with the procedure (because there is a learning curve and initial attempts frequently produce acellular specimens) and that an experienced cytopathologist be available (23,27). Both requirements may be hard to meet in community-based centers in developing countries with a low incidence of breast cancer. Consequently, SM may be of clinical value for investigating palpable masses in such populations (Fig. 3), because diagnostic values are independent of breast cancer incidence and mammography findings. Recently, Allen et al. (30) quantitatively analyzed the cost-effectiveness of SM, verifying the potential value of the technique in avoiding unnecessary biopsies when used after indeterminate mammography findings. Moreover, the technique is easy to interpret and has excellent interobserver agreement, as shown both by this study and by the European trial (10).
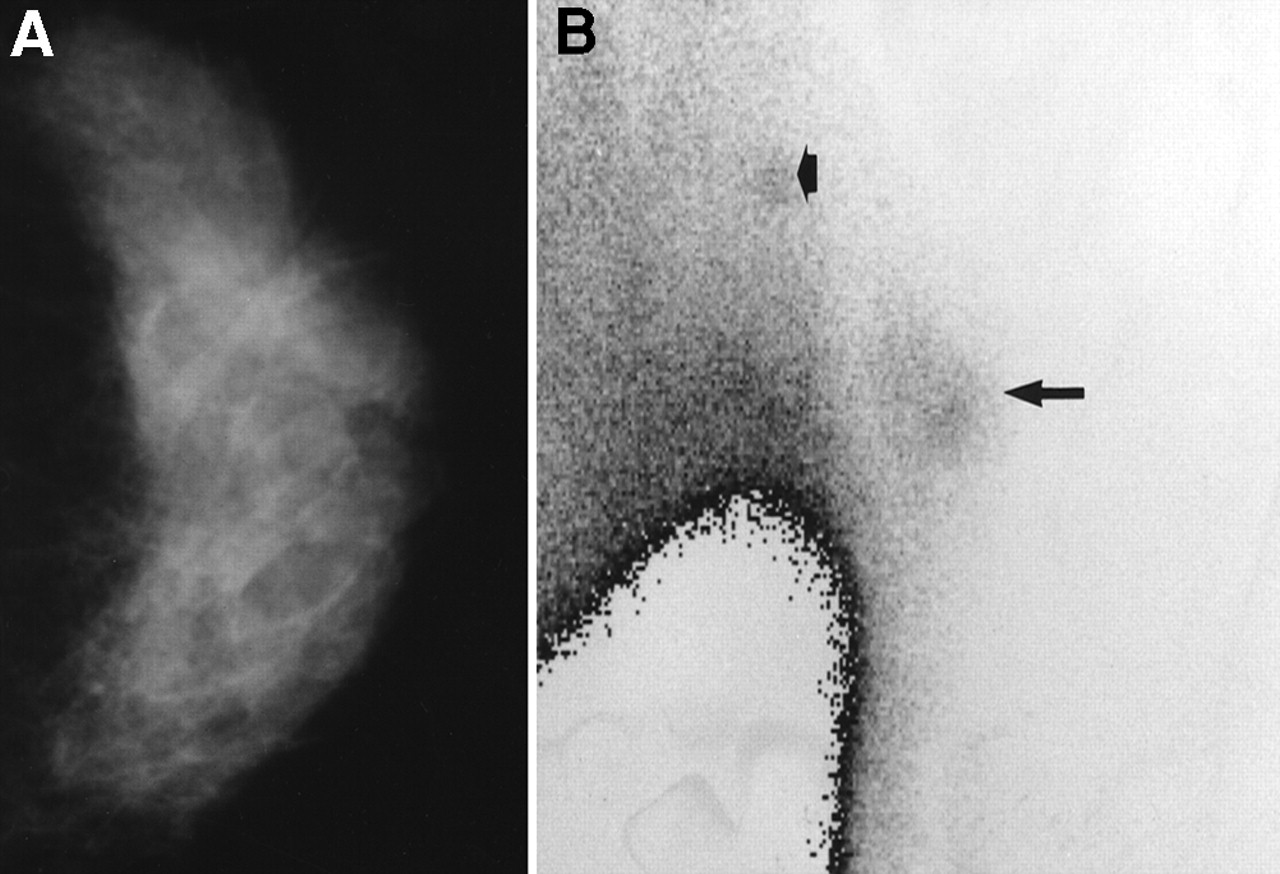
A 42-y-old patient with palpable lesion of left breast. (A) Mammogram shows high radiologic density with no suggestive abnormalities (BI-RADS 1). (B) Left lateral prone SM shows tumor uptake (arrow) corresponding to invasive ductal carcinoma.
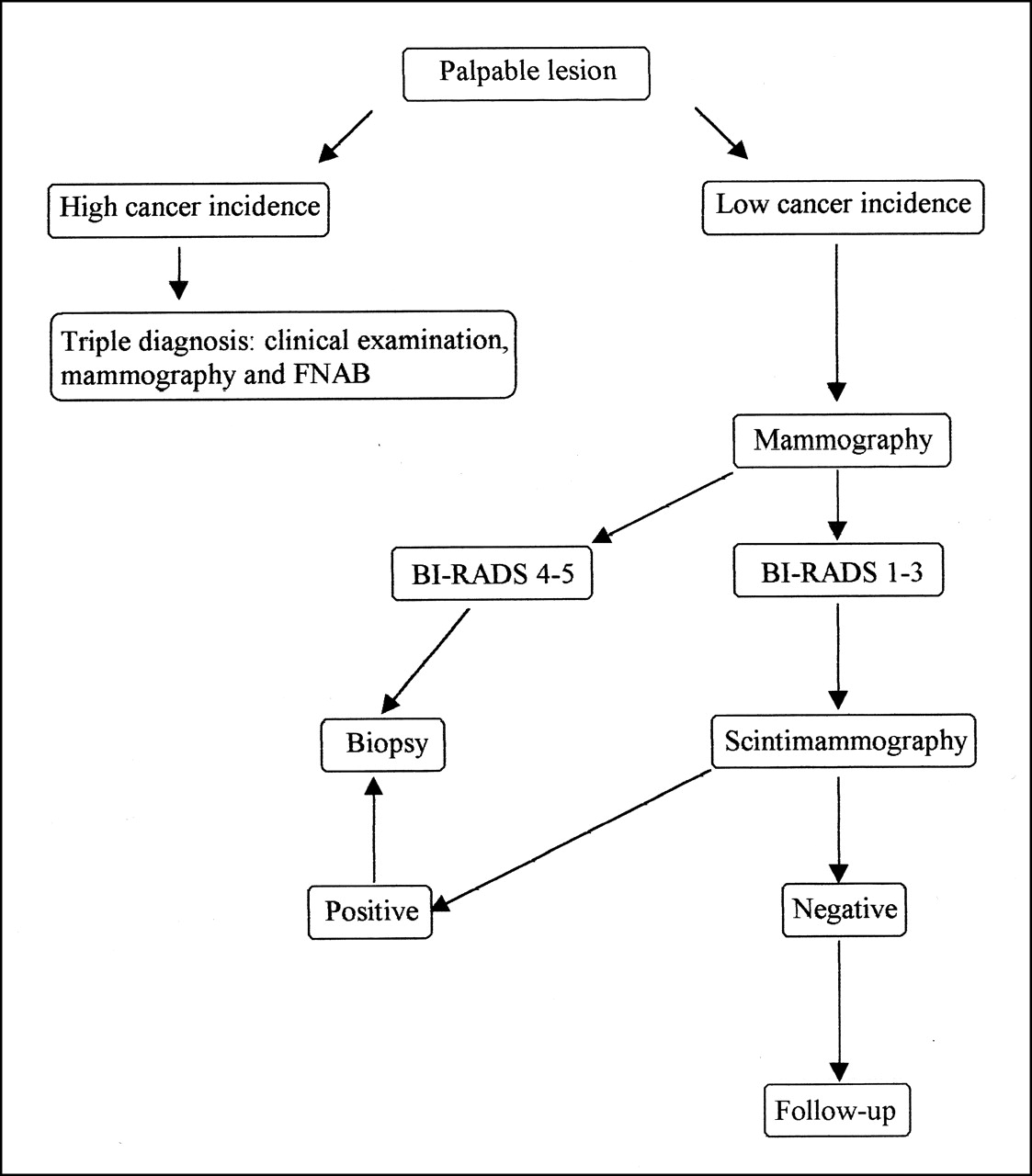
Flow chart shows diagnostic role of joint use of mammography and SM in evaluation of patients with palpable breast lesions.
CONCLUSION
SM provides clinically valuable information on patients with palpable breast lesions. The sensitivity of the technique does not depend on the epidemiologic or ethnic characteristics of the population or on the radiologic density of breasts. SM has a complementary role to mammography in patients with negative mammography findings (BI-RADS 1–3). The technique has the potential to be used to assess palpable masses in community-based centers in countries with a low incidence of breast cancer.
Acknowledgments
The authors thank the following principal investigators from participating countries: Vassilios Papantoniou, MD (Alexandria University Hospital, Athens, Greece); María E. Solano-Bravo, MD (Clinical Investigations Center, Havana, Cuba); and Huiqing Zhu, MD (Hua Shan Hospital, Shanghai Medical University, Shanghai, China). The authors also thank Jamshed Bomanji, PhD (Institute of Nuclear Medicine, University College London Medical School, London, U.K.), for technical assistance. This study was supported by grants from the International Atomic Energy Agency in the framework of the coordinated research project “Evaluation of 99mTc-Radiopharmaceuticals in the Diagnosis and Management of Breast Cancer Patients” (E1.30.17).
Footnotes
Received Feb. 22, 2001; revision accepted Jul. 13, 2001.
For correspondence or reprints contact: Omar Alonso, MD, Centro de Medicina Nuclear, Hospital de Clínicas, Avenida Italia s/n, Montevideo 11600, Uruguay.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Inconclusive Triple Diagnosis in Breast Cancer Imaging: Is There a Place for Scintimammography?
- Staging of Regional Lymph Nodes in Melanoma Patients by Means of 99mTc-MIBI Scintigraphy
- Diagnostic Value of 99mTc-Methylene Diphosphonate and 99mTc-Pentavalent DMSA Compared with 99mTc-Sestamibi for Palpable Breast Lesions