


Abstract
After potentially curative therapy of non–small cell lung cancer (NSCLC), masses or symptoms suggestive of relapse are common but may be difficult to characterize. Early detection is important because salvage therapies are available for localized recurrence. This study evaluated whether 18F-FDG PET is useful and predictive of outcome in this setting. Methods: For 63 consecutive patients with suspected relapse >6 mo after definitive treatment of NSCLC, the apparent extent of disease on conventional restaging was compared with that on FDG PET. Patients with already confirmed systemic metastases were excluded unless locally aggressive treatment of these was being considered. Serial imaging and pathologic results were obtained during a median follow-up of 19 mo to validate diagnostic findings. Prognostic significance was tested using the Cox proportional hazards regression model. Results: PET had positive findings in 41 of 42 patients with confirmed relapse (sensitivity, 98%). No disease was evident during a minimum follow-up of 12 mo in 14 of 15 patients with clinically suspected relapse but negative PET findings (negative predictive value, 93%). PET induced a major management change in 40 patients (63%), including 6 whose treatment was changed from curative to palliative, 3 whose treatment was changed from palliative to curative, and 9 for whom negative PET findings prevented active management. Both the presence (P = 0.012) and the extent (P < 0.0001) of relapse on PET were highly significant prognostic factors. There was also significant prognostic stratification based on the treatment delivered after the PET study (P = 0.011), but after adjustment for this treatment, PET status remained highly predictive of survival. Conclusion: PET better assesses the status of disease and stratifies prognosis than does conventional staging, affects patient management, and should be incorporated into paradigms for suspected recurrence of NSCLC.
Attempted cure of non–small cell lung cancer (NSCLC) using a single therapy modality is often unsuccessful, irrespective of the modality chosen (1). The high rate of failure has stimulated the use of combined-modality therapies despite high cost and significant morbidity. Frequently, patients complain of residual symptoms or manifest diagnostic imaging abnormalities that prompt evaluation for residual or recurrent disease. CT is currently the standard diagnostic imaging test for reevaluating previously treated NSCLC patients, particularly if symptoms or surveillance suggest disease relapse. However, the ability of CT to differentiate between tumor and scar tissue after surgery or radiotherapy is limited (2). 18F-FDG PET has been shown to be more accurate than CT for staging newly diagnosed lung cancer (3). Preliminary data also suggest superiority over CT for restaging lung cancer (4,5) and a markedly inferior prognosis for patients with positive PET findings than for those with negative findings (6).
Although no conclusive data support the use of any therapies in relapsed lung cancer, some patients with localized relapse may be cured with appropriate aggressive therapy. Preliminary data suggest that PET can identify such patients (7). Detection of widespread disease would, however, make curative therapies futile and a waste of scarce health care resources in addition to unnecessarily subjecting the patient to morbidity. Conversely, the use of active therapies in the absence of malignancy is also clearly inappropriate.
In a previous prospective evaluation of the clinical impact of PET on the management of NSCLC (8), we showed that the results of PET had a substantial impact on the management of 34 patients with suspected relapse >6 mo after completion of therapy delivered with curative intent. The aim of the current study was to confirm the appropriateness of these management changes by longer follow-up of a larger patient cohort. In particular, we sought to further validate the utility of PET in such patients by examining the relationship between disease status as assessed by PET and patient survival.
MATERIALS AND METHODS
Patient Eligibility
Consecutive patients referred for clinical evaluation of suspected relapse of NSCLC between November 1996 and December 1998 were prospectively entered into a database. Patients were eligible for this study if they had a confirmed histologic diagnosis and had been treated with curative intent >6 mo before referral for a follow-up PET scan. Patients were excluded from analysis if they already had confirmed systemic metastatic disease based on either biopsy or unequivocal conventional imaging appearances, unless that disease was amenable to aggressive local therapy. FDG PET was performed for clinical indications in all patients. Follow-up of clinical outcome was approved by our institutional review board.
PET Scan Acquisition and Processing
PET scans were acquired on a PENN-PET 300-H scanner (UGM Medical Systems, Inc., Philadelphia, PA). Patients fasted for a minimum of 4 h before the scan. Emission data were acquired 1 h after intravenous administration of 74–120 MBq FDG. The scan routinely incorporated the lower neck, thorax, and upper abdomen, consistent with the usual extent of staging CT scans. If additional but unconfirmed sites of metastatic disease were suggested on conventional staging, the scan was extended to include the appropriate regions. PET was not used to evaluate the brain. The performance characteristics of this scanner and processing methods have been described previously (9–11).
The emission scan was reconstructed using the iterative technique of ordered-subset expectation maximization. Image sets, both with and without measured attenuation correction, were reviewed on a computer console using a display program that allows interactive review of orthogonal slices. An experienced nuclear medicine physician generated a clinical report after reviewing previous imaging results and clinical information. This included, in almost all cases, direct correlation with the recent CT scan. When the CT scan was unavailable, the report of the CT investigation was obtained. Standard uptake values were not routinely calculated. Once issued, the PET report was entered into the database and was not reinterpreted in the light of subsequent clinical information.
Determination of Disease Extent
The medical record was reviewed to determine the disease stage at initial diagnosis according to the 1997 update of the international staging system for lung cancer (12), and the primary treatment delivered subsequent to this diagnosis was recorded.
The staging schema used for classification of newly diagnosed NSCLC was believed to be inappropriate for the restaging setting. Rather, the patients were classified according to the extent of apparent relapse based on information available on conventional staging investigations performed before the PET scan (pre-PET extent category) and based on incorporation of the PET information with the previous information (post-PET extent category). The pre-PET extent category included biopsy results when they were available before the PET scan. The PET results were not interpreted in a masked manner; thus, this study evaluated the incremental, not the independent, information provided by PET.
Patients were classified as negative if imaging showed no abnormality suggestive of recurrence or, in the case of pre-PET evaluation, if biopsy of a residual structural abnormality had negative findings. Patients with abnormality confined to the previous primary tumor site and potentially suitable for salvage surgery or radical radiotherapy were classified as having local relapse. Patients with abnormalities involving intrathoracic lymph nodes and potentially amenable to radical radiotherapy were classified as having limited nodal relapse. Patients with intrathoracic lymph node abnormalities too extensive for radical radiotherapy or with lymphadenopathy beyond the thorax were classified as having extensive nodal relapse. Finally, patients with abnormalities involving major organs or the skeleton were classified as having systemic relapse.
Conventional restaging routinely involved CT with dynamic contrast medium, unless contraindicated because of contrast allergy. Bone scanning was performed only for patients with musculoskeletal symptoms or elevated alkaline phosphatase levels. CT or MRI of the brain was performed only for patients with clinically suspected cerebral metastasis. On CT scans, symptomatic or progressively enlarging lobular masses were considered suggestive of residual disease unless found to be negative for disease on histologic examination, whereas bandlike abnormalities were considered likely to reflect scarring. Mediastinal and hilar lymph nodes were regarded as positive for tumor on CT if they were >1 cm in maximum transverse diameter and larger than on the baseline evaluation. Histologically unconfirmed systemic metastases found on conventional staging were considered positive for disease if active treatment was planned on their basis but equivocal if, despite their presence, the referring clinician was still considering curative salvage treatment of suspected more localized relapse.
The post-PET extent of disease relied fully on the results of PET when these were discordant with other imaging findings, even when the results of prior biopsy had been negative. Focal areas of increased activity of greater intensity than mediastinal soft tissues on attenuation-corrected images were considered positive for active disease. However, diffuse changes in the lung or pleural reflections conforming to a prior radiotherapy treatment volume were generally reported as negative for active disease. These appearances are common after high-dose radiotherapy and are believed likely to be inflammatory. When a baseline PET scan was available, it was used for comparisons of the extent and intensity of ongoing abnormalities at previously documented sites of PET abnormality.
In addition to extent, the specific sites of abnormality indicating relapsed disease were recorded for both conventional imaging and PET. These sites were used for validation. Both the status of relapse and the distribution of disease were confirmed whenever possible by histologic examination. When histologic confirmation was unavailable, evidence of progression on serial imaging within 6 mo was considered to indicate a site of disease relapse, whereas no evidence of progression after at least 12 mo of follow-up was considered to confirm absence of active disease at that site. Patients who died without clear evidence of disease progression on conventional imaging were considered not assessable. Lack of imaging evidence of progressive disease after delivery of radical or high-dose palliative radiotherapy to a suspected localized recurrence was not considered to confirm this as a site of relapse unless relapse had been histologically confirmed before treatment began.
Assessment of Impact
Referring clinicians are asked to prospectively record a pre-PET management plan on our routine clinical request form. This plan was entered in a database. If not explicitly recorded on the referral request, treatment intent was categorized by an oncologist experienced in lung cancer management, who synthesized the available pre-PET clinical and imaging information. For 20 patients, a pre-PET management plan had not been recorded on the request form, and we relied on the patient’s pre-PET medical record. The post-PET plan and intent were determined from the medical record or contact with the referring clinician and in all but 1 patient reflected the treatment actually delivered.
The impact on management was considered high when the treatment intent or modality was changed (e.g., from palliative to curative treatment or from surgery to radiotherapy). Although not immediately altering treatment delivery, the change of a patient from expectant palliative treatment for suspected relapse to observation on the basis of negative PET findings was classified as of high impact because of the potential for psychologic reassurance of the patient from such a change. The impact was recorded as medium when the method of treatment delivery was changed (e.g., a change in radiation treatment volume). When the PET results did not indicate a need for change, the impact was considered to be low. PET was considered to have had no impact when the management chosen conflicted with post-PET disease extent and was believed to be inappropriate on the basis of a synthesis of all available information.
Patients within any given disease category could have a range of impact outcomes. For example, patients whose CT findings showed extensive local recurrence amenable only to palliative treatment could be converted to curative salvage surgery if PET showed a small recurrence, even though both the pre-PET extent and the post-PET extent would be categorized as localized recurrence. Alternatively, discordance between extent categories did not necessarily affect management. For example, the palliative radiotherapy planned for some patients with symptomatic local recurrence was still considered appropriate even though additional but asymptomatic sites of disease were detected.
Follow-Up
After treatment, progress updates were obtained from the medical record, family physician, or treating oncologist. When relevant, details of the date and cause of death were obtained. The disease status at the time of death was recorded. For patients treated with curative intent, the site or sites of first progression were recorded.
Statistical Methods
Survival was measured from the date of the restaging PET scan to the date of death from any cause. Survival estimates were obtained using the Kaplan–Meier product-limit method and compared using the Cox proportional hazards regression model. The prognostic significance of individual factors has been summarized using hazard ratios representing the relative death rate for a given group relative to a baseline group. The 95% confidence interval (CI) is given for the main results. Unless otherwise indicated, 2-sided probability values are reported with no adjustment for multiple comparisons.
RESULTS
Patient Population
In all, 63 patients met the eligibility criteria (41 men, 22 women; mean age ± SD, 66 ± 9 y). The histologic cancer types were squamous cell carcinoma in 36 patients; adenocarcinoma in 19 patients; large cell carcinoma in 7 patients; and non–small cell carcinoma, not otherwise specified, in 1 patient. The primary curative treatment had been surgery in 18 patients (29%), radical radiotherapy with or without concurrent chemotherapy in 33 patients (52%), and chemoradiotherapy plus surgery in 12 patients (19%).
Detection of Relapse
Relapse involving at least 1 site was confirmed in 42 (67%) of 63 patients by death from progressive disease (n = 30), by pathologic examination (n = 5), or by serial imaging (n = 7). PET was positive for disease in 41 (98%) of these patients. The 1 false-negative PET result was for a study that was limited because of the patient’s claustrophobia and that did not include the site of confirmed recurrence. Conventional staging suggested relapse in all 42 of these patients, yielding a sensitivity of 100%. In 1 patient whose CT scan showed a suspected isolated systemic metastasis but whose PET findings were negative, a small metachronous primary bronchial malignancy subsequently developed and was detected on follow-up bronchoscopy. The site of structural abnormality did not progress, and the PET result was considered true-negative for systemic relapse at this site but incorrect for extent because the developing metachronous primary tumor was missed.
At the study censor date and with a minimum follow-up of 12 mo, 17 patients (27%) had no evidence of relapse. The PET findings were negative in 14 of these patients, giving a specificity of 82%. All but 2 had abnormal CT findings suggestive of thoracic relapse, giving a specificity of only 12% for conventional imaging. Both of the patients without abnormal imaging findings had other clinical evidence of relapse (progressive loss of weight in one and a recurrent pleural effusion in the other). Three PET studies had false-positive findings, all in patients also incorrectly thought to have intrathoracic relapse on the basis of CT findings. One of these scans, seen early in our experience, clearly showed postirradiation changes and was incorrectly interpreted. Because of the discordance in the distribution of abnormality seen on CT compared with that seen on PET, ongoing observation rather than planned palliative radiotherapy was instituted for this patient when the hemoptysis that had led to her referral settled. The other 2 false-positive PET scans showed abnormalities confined to the neck that, in retrospect, may have reflected asymmetric uptake in strap muscles. Neither patient had active treatment, and they remained free from progression of disease in the neck after 707 and 840 d of follow-up. PET correctly excluded suspected intrathoracic relapse in both these patients. In 4 patients, the disease status could not be evaluated because of death from other illnesses (2 patients) or because of treatment introduced on the basis of imaging findings that were not pathologically confirmed (2 patients).
Comparison of Disease Extent as Evaluated Conventionally and by PET
The relapse extent determined by PET was different from the conventionally determined extent in 44 (70%) of 63 patients (95% CI, 57%–81%). Overall, 33% of patients had less extensive disease and 37% had more extensive disease than conventional evaluation suggested (Table 1). Within each category were also some differences in the distribution of active disease that had an impact on patient management. Overall, conventional staging was correct in its assignment of extent category in 12 (24%) of 49 evaluable patients, whereas PET was correct in 42 (86%) of 49 patients.
Comparison of Extent of Suspected Relapse as Assessed Before and After PET
The concordance between the pre- and post-PET evaluations of the extent of disease relapse is presented in Table 2. Validation of the extent of disease as assessed by conventional evaluation techniques and PET is also displayed. For 44 patients, the pre- and post-PET categories of the extent of disease relapse differed. For 36 (82%) of these patients, the accuracy of the extent of disease could be validated. In 31 (86%) of 36 patients, follow-up has shown that PET was correct, whereas for only 1 patient (3%) was the pre-PET classification correct (P < 0.0001). This patient was the one with claustrophobia. For 4 other patients, the extent of disease as assessed by both PET and CT appears to have been incorrect. For 12 patients, the extent category was concordant on conventional and PET imaging but either the distribution of disease or the level of confidence in the imaging result was sufficient to change management after PET. Similarly, there were 5 patients for whom the extent category differed but for whom management was not altered because the treatment planned was still deemed to be appropriate even after PET.
Concordance and Validation of Pre-PET and Post-PET Extent of Suspected Relapse Grouped by Impact of PET Scan
Impact of PET Results on Patient Management
The PET results had a high impact on management in 40 patients (63%). The pre- and post-PET treatment plans for these patients are summarized in Table 3. Of note, 6 patients were changed from curative to palliative care after PET showed more extensive disease than had been suspected on conventional evaluation. Additionally, 8 patients for whom active palliative therapy was being considered and 1 patient for whom an invasive diagnostic procedure was planned received no active therapy after negative results were found on PET. Thus, 9 patients were spared the morbidity of these interventions. An example is shown in Figure 1. Another 6 patients whose disease was considered to have relapsed but for whom active palliative treatment was not planned unless their symptoms increased also had negative PET findings. Because of the potential psychologic impact on patients of being cleared of active disease, the impact of PET in these instances was also classified as high.
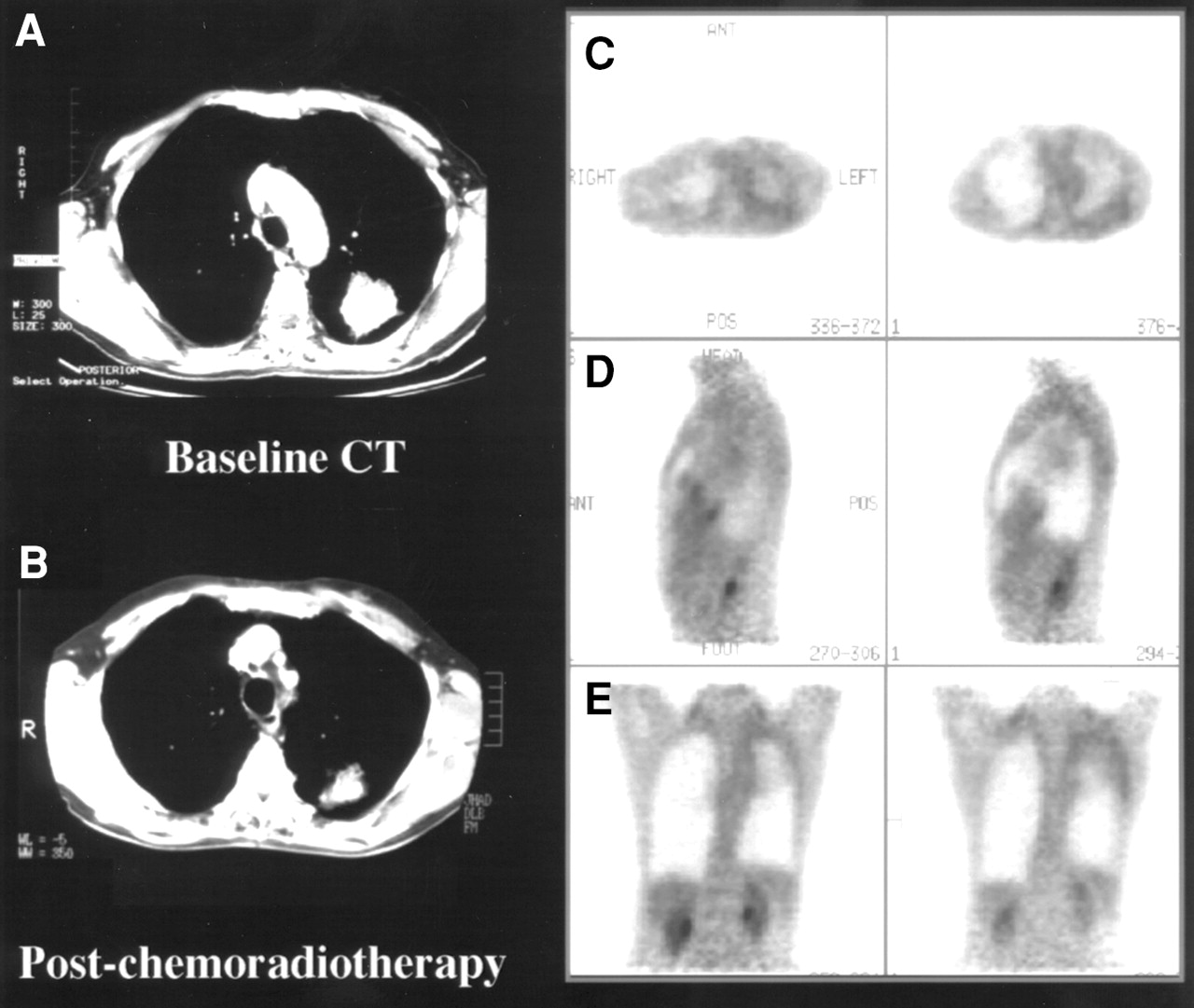
Hemoptysis and residual mass 9 mo after radical chemoradiotherapy for left upper lobe NSCLC suggested local relapse despite partial CT response between baseline (A) and posttreatment (B) scans. Representative transaxial (C), sagittal (D), and coronal (E) planes of PET scan showed low-grade pleural changes consistent with postradiotherapy effects but no evidence of recurrent disease. Palliative radiotherapy was cancelled, and patient remained well >12 mo after PET without evidence of active disease.
Summary of 40 Patients for Whom PET Changed Treatment Intent or Modality (High Impact)
PET had a medium impact on management in 8 patients (13%). Management changes in these patients primarily included changes in radiation treatment volume. PET had a low impact (i.e., did not change the planned management) on 13 patients (21%), for whom either the relapse extent was concordant with that found on conventional restaging (7 patients) or the documentation of a different distribution of disease did not alter the appropriateness of the planned treatment (6 patients). Although PET had shown more extensive disease in 5 of 6 of these patients, the planned palliative treatment was considered appropriate because the additional sites of disease were asymptomatic at that time. The remaining patient had PET findings showing local recurrence after previous resection of a T2 N2 tumor. Although the mediastinum was negative for tumor on PET, we believed that the residual enlarged nodes found in the mediastinum on CT scanning needed to be included in the radical radiotherapy volume.
PET had no impact on management in 2 other patients (3%) who had discordant PET and CT findings. These 2 patients received active treatment despite negative PET findings and remain free from progression at >19 mo. One underwent resection of a lung mass and associated nodes with pathologic confirmation of a complete response to previous chemoradiation, whereas the other received radical radiotherapy of a chest wall mass that was negative for tumor on PET.
The post-PET management plan differed from the treatment actually delivered in 1 patient who died before commencing palliative radiotherapy. This patient was found to have local relapse on both pre-PET and post-PET assessment, and the treatment decision was therefore unaffected by the PET result. Another patient thought to have only local relapse on CT was found to have possible right peritracheal nodal disease also on PET and was to undergo palliative radiotherapy, but because her hemoptysis settled, this therapy was not subsequently delivered. Definite recurrent disease had not been evident during a follow-up of 722 d, and the findings of both studies are therefore considered to have been false-positive. This patient was the one mentioned earlier with the false-positive result related to suspected postradiotherapy inflammatory change.
Confirmation of PET Results in Patients with High- and Medium-Impact Studies
Of the 40 patients in the high-impact group, confirmation of the true disease status was assessable by histology or by serial imaging in 37 (93%). Of these 37 patients, PET was shown to be correct in 33 (89%). The 4 instances in which PET was incorrect included the study that was false-negative but technically limited by claustrophobia, the 2 studies that showed false-positive lower neck uptake, and a study in which PET correctly excluded systemic metastasis but failed to detect a metachronous lung primary. All 4 assessable cases in which PET modified delivery of a planned therapy (medium impact) were confirmed.
Prediction of Survival by PET
Survival data were analyzed with a closeout (study censor) date of July 1, 1999. Thus, the potential follow-up ranged from 6 to 31 mo (0.5–2.6 y), with a median of 19 mo (1.5 y). All 63 patients entered into the study had a known status at the closeout date. All patients with negative PET findings were followed for a minimum of 12 mo after the scan (range, 371–849 d).
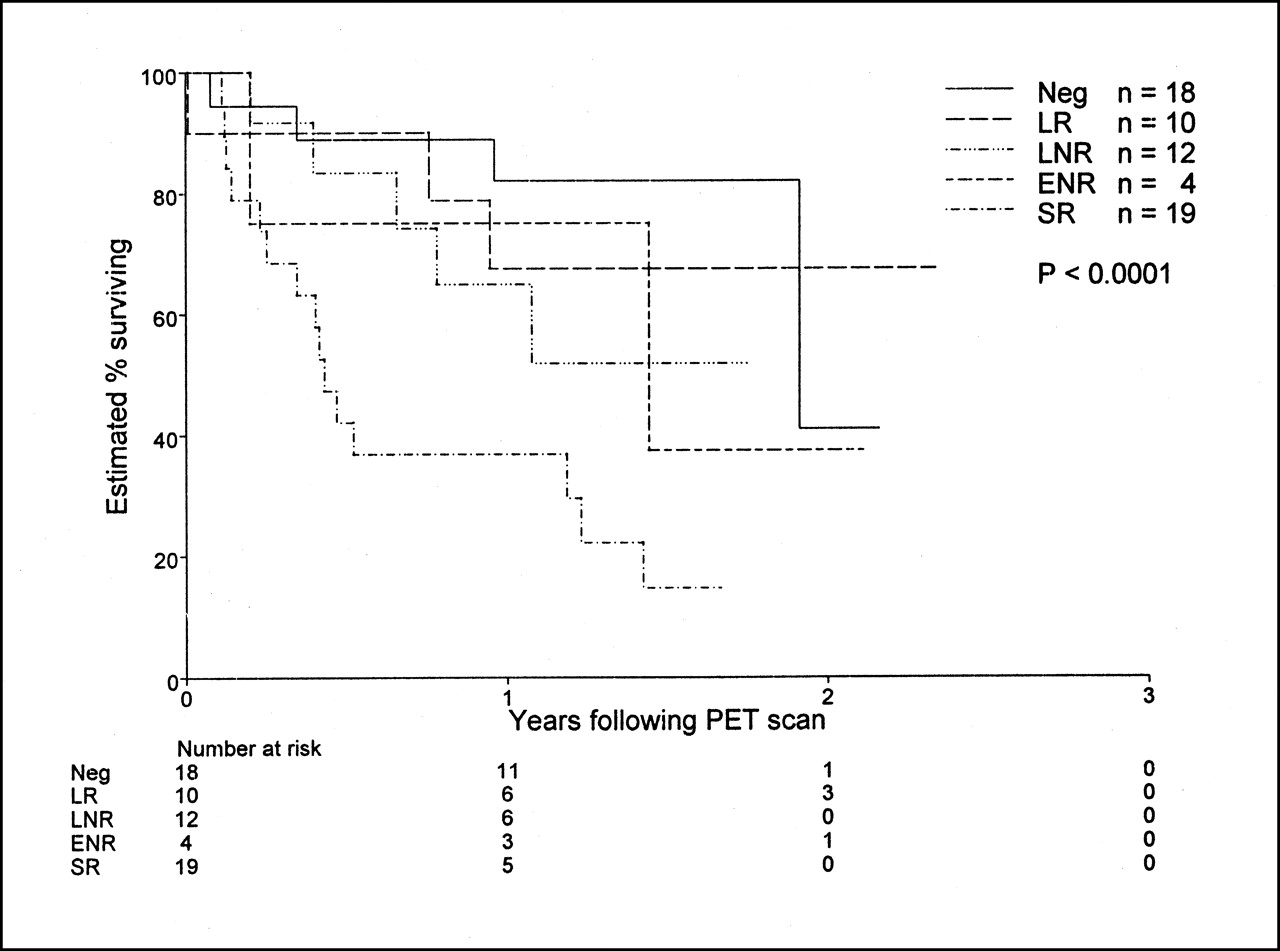
Estimated survival at 1 y was 62% (95% CI, 50%–75%), and estimated survival at 2 y was 40% (95% CI, 22%–59%). Neither the stage at initial diagnosis nor the primary treatment delivered was associated with survival in this selected patient cohort. Positive PET findings were, however, associated with a poorer prognosis than were negative findings (Fig. 2). Further, the extent of relapse assessed after the PET scan was a highly significant prognostic factor (P < 0.0001) (Table 4; Fig. 3).
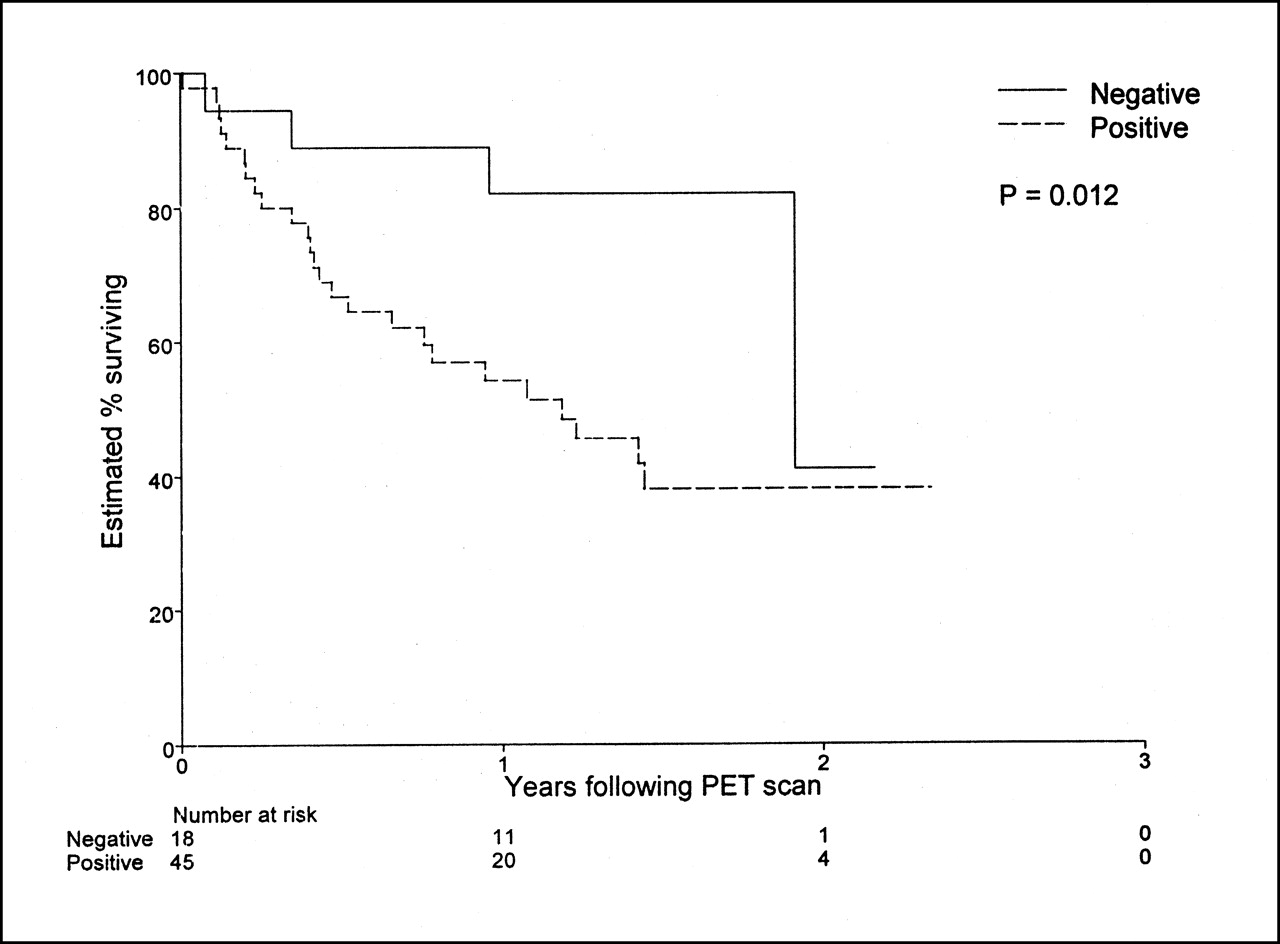
Graph shows strong prognostic stratification by whether PET was positive or negative for relapse in 63 consecutive patients in whom relapse was suspected on basis of conventional imaging findings (n = 61) or clinical features (n = 2).

Graph shows strong relationship between apparent extent of disease on PET scanning and survival in 63 consecutive patients in whom relapse was suspected on basis of conventional evaluation. This relationship remained significant after adjusting for pre-PET evaluation of extent of disease relapse or for treatment subsequently delivered. ENR = extensive nodal relapse; LNR = limited nodal relapse; LR = local relapse; SR = systemic relapse.
Association Between Apparent Extent of Relapse and Survival in 63 Patients with Suspected Relapse of NSCLC
There was also a significant difference in the prognosis of patients given no treatment, curative treatment, palliative treatment, or supportive treatment on the basis of PET (P = 0.011) (Table 5). Of note, the group receiving curative treatment had similar survival to the group not treated after having negative scan findings.
Association Between Treatment Delivered After PET and Survival in 63 Patients with Suspected Relapse of NSCLC
DISCUSSION
Previous studies evaluating the role of FDG PET scanning in NSCLC have evaluated mainly patients for whom surgical resection was being considered. The use of FDG PET for staging of lung cancer was recently reviewed (13). The role of this emerging oncologic imaging technique for restaging this disease is, however, less well defined but is becoming relevant as new salvage therapies are being evaluated for patients with early relapse after initial treatment given with curative intent (7). Our own preliminary data suggest that PET scanning in the early posttreatment phase (median, 70 d) can stratify patients by response into categories with widely differing survival probabilities (14), but the current report relates to a population of patients evaluated >6 mo after their primary treatment.
Our results suggest that PET is an accurate technique for detecting recurrent or persistent disease. The sensitivity of PET for relapse was 98% (41/42 patients), whereas the specificity was 82% (14/17 patients), giving an overall accuracy of 93%. Our sensitivity results are in keeping with those of earlier studies (4,5) in which FDG PET correctly detected intrathoracic relapse in 34 (97%) of 35 patients and 26 (100%) of 26 patients, respectively. The specificity in these earlier studies differed substantially, at 8 (100%) of 8 and 8 (61.5%) of 13, respectively. The study with lower specificity looked only at the intensity and not the pattern of uptake for diagnosing thoracic recurrence. Curvilinear pleural abnormalities within the prior radiation therapy field were graded as positive even though the authors of this report specifically commented that such abnormalities were, in their experience, most commonly inflammatory. In general, our practice has been to call these abnormalities negative, but postradiotherapy inflammatory changes accounted for 1 of 3 false-positive results in our series. The concordance of the distribution of disease relapse between PET and CT was not addressed in either of these studies, and because extrathoracic regions were not evaluated by PET, the occurrence of false-positive results in the lower neck could not be compared with that found in our study.
Our study suggests that PET, in addition to accurately confirming or excluding disease relapse, more accurately assesses the distribution of disease than do conventional techniques used for restaging when relapse of lung cancer is suspected. This accuracy is particularly important in patients for whom the PET result altered management. Of 28 evaluable patients whose PET findings were discordant with conventional imaging findings and led to altered treatment intent or modality (Table 2), the extent of disease suggested by imaging findings was correct in 25 (89%) for PET versus only 1 (3%) for CT.
Another study has also documented discordance between the PET and CT estimations of the extent of disease relapse (7). The rate of discordant findings between PET and CT was lower in that study (25%) than in ours (69%), probably because that study’s PET imaging protocol included only the lung fields, whereas we routinely included the lower neck, upper abdomen, and any areas that appeared clinically suggestive on conventional restaging investigations. The more extensive evaluation of our patients would be expected to increase the likelihood of detection of metastatic disease unrecognized on conventional restaging investigations and also to exclude disease in false-positive sites found by other modalities.
An earlier study on the use of FDG PET after primary treatment of NSCLC evaluated a variable time after this treatment ranging from 2 d to 108 mo (6) and also suggested powerful stratification of patients based on whether their PET findings were positive or negative. The current study evaluated the role of PET for detecting relapse >6 mo from primary treatment, when any acute effects from treatment would be anticipated to have largely subsided, and might not, therefore, be directly comparable. Nevertheless, our study supported the earlier study in finding powerful prognostic stratification between positive and negative PET results (Fig. 2). After correction for changes in management induced by the PET result, the extent of disease relapse determined by FDG PET remained predictive of survival.
The markedly better survival in patients who received no active treatment after negative PET findings than in patients who received either palliative or supportive care after positive FDG PET findings attests to the appropriate stratification of patient prognosis by PET results (Table 5). Of interest is the relatively good survival of patients assigned to salvage curative treatment after PET, a finding consistent with limited earlier data suggesting that patients with early relapse detected on PET can have good survival (7). This suggests that current nihilistic views regarding the management of relapsed lung cancer may reflect poor patient selection by conventional restaging techniques rather than inefficacy of available treatments.
Of potential economic and clinical importance was the observation that 15 patients (24%) in this series who were suspected to have relapsed by conventional evaluation subsequently received no active treatment after a negative PET evaluation. Only 1 of these patients had relapse confirmed on follow-up. Because the area of relapse was not imaged adequately on account of patient claustrophobia, serial CT was arranged and there was only a minor delay in initiation of active treatment. Survival for the group not treated actively was markedly superior to that for patients shown to have incurable relapse by PET (Table 5). By preventing treatment in these patients, PET is likely to have not only reduced expenditure but also spared these patients unwarranted toxicity.
Although comparison of a masked reading of PET with a masked reading of CT may be appropriate if PET were to be suggested as a replacement for CT, the main purpose of this study was to evaluate the incremental diagnostic value and impact of PET in routine clinical practice. The very high false-positive rate and associated poor specificity of CT in this series is likely related to the clinical selection of patients for PET in our facility. Patients with definite relapse on conventional restaging techniques or by biopsy are not offered PET in our facility unless curative treatment is being contemplated. We believe that this selection bias is appropriate given the relative costs of CT and PET.
The minimum follow-up of at least 12 mo in all patients with negative PET findings may be too short to exclude residual disease in these patients, but all PET studies were performed at least 6 mo after the completion of treatment. Therefore, progression-free survival in these patients was in excess of 18 mo, which would appear to be a reasonable time to detect relapse of this disease process. Because of intercurrent treatment or the intervening death of some patients, not all cases in which the PET stage differed from the conventionally found stage could be validated.
CONCLUSION
Our data suggest that the accuracy, prognostic stratification, and patient treatment selection capabilities of PET are superior to those of conventional restaging techniques. We suggest that PET should be performed on patients who have suspected relapse after potentially curative treatment, particularly if active treatment is being considered.
Acknowledgments
The authors thank the cyclotron staff of the Peter MacCallum Cancer Institute and the Austin & Repatriation Medical Centre (Melbourne, Australia) for providing a reliable supply of FDG and the referring clinicians for providing follow-up information. The authors are also grateful for the tireless efforts of their technologist and secretarial staffs to continually do more with less. This study was supported by a grant from the Consultative Committee for Diagnostic Imaging on behalf of the Australian Department of Health and Aged Care.
Footnotes
Received Feb. 22, 2001; revision accepted Jul. 18, 2001.
For correspondence or reprints contact: Rodney J. Hicks, MD, Centre for Positron Emission Tomography, Peter MacCallum Cancer Institute, 12 Cathedral Pl., East Melbourne, Victoria 3002, Australia.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- The Injustice of Being Judged by the Errors of Others: The Tragic Tale of the Battle for PET Reimbursement
- Response Assessment Criteria and Their Applications in Lymphoma: Part 1
- 18F-FDG PET/CT and Lung Cancer: Value of Fourth and Subsequent Posttherapy Follow-up Scans for Patient Management
- Follow-up or Surveillance 18F-FDG PET/CT and Survival Outcome in Lung Cancer Patients
- Improvement in PET/CT Image Quality with a Combination of Point-Spread Function and Time-of-Flight in Relation to Reconstruction Parameters
- Doing More Harm than Good? Do Systematic Reviews of PET by Health Technology Assessment Agencies Provide an Appraisal of the Evidence That Is Closer to the Truth than the Primary Data Supporting Its Use?
- The role of positron emission tomography in the management of non-small cell lung cancer
- From RECIST to PERCIST: Evolving Considerations for PET Response Criteria in Solid Tumors
- Partnerships in Oncology and Radiology: The Role of Radiology in the Detection, Staging, and Follow-up of Lung Cancer
- PET Evaluation of Lung Cancer
- Progress and Promise of FDG-PET Imaging for Cancer Patient Management and Oncologic Drug Development
- The Role of PET Scan in Diagnosis, Staging, and Management of Non-Small Cell Lung Cancer
- PET/CT Using 18F-FDG in Suspected Lung Cancer Recurrence: Diagnostic Value and Impact on Patient Management
- Quantification of 18F-FDG Uptake in Non-Small Cell Lung Cancer: A Feasible Prognostic Marker?
- American Society of Clinical Oncology Treatment of Unresectable Non-Small-Cell Lung Cancer Guideline: Update 2003
- Positron Emission Tomography Is Superior to Computed Tomography Scanning for Response-Assessment After Radical Radiotherapy or Chemoradiotherapy in Patients With Non-Small-Cell Lung Cancer
- Use of a Dual-Head Coincidence Camera and 18F-FDG for Detection and Nodal Staging of Non-Small Cell Lung Cancer: Accuracy as Determined by 2 Independent Observers