


Abstract
Survival of lung cancer patients remains poor despite increasingly aggressive treatment. Conventional staging has well-described limitations. 18F-FDG PET has been shown to stage lung cancer more accurately than does CT scanning, but the impact on patient treatment and outcome is poorly defined. This study evaluated this impact in routine clinical practice within a tertiary oncology facility. Methods: For 153 consecutive patients with newly diagnosed non–small cell lung cancer, the treatment plan based on conventional staging methods was compared with the treatment plan based on incorporation of PET findings. Survival was analyzed using the Cox proportional hazards regression model. Results: For broad groupings of stage, 10% of cases were downstaged and 33% upstaged by PET. When assessable, the PET stage was confirmed in 89% of patients. PET had a high impact on 54 patients (35%), including 34 whose therapy was changed from curative to palliative, 6 whose therapy was changed from palliative to curative, and 14 whose treatment modality was changed but not the treatment intent. For 39 patients (25%), a previously selected therapy was altered because of the PET findings. The Cox model indicated that the pre-PET stage was significantly associated with survival (P = 0.013) but that the post-PET stage provided much stronger prognostic stratification (P < 0.0001) and remained significant after adjustment for treatment delivered. Conclusion: Staging that incorporated PET provided a more accurate prognostic stratification than did staging based on conventional investigations. Further, the additional information provided by PET significantly and appropriately changed management in the majority of patients.
Lung cancer is the most common cause of cancer death in western society and is increasing in incidence. Surgery remains the mainstay of attempts to cure non–small cell lung cancer (NSCLC), but postsurgical prognosis remains poor (1). Radical radiotherapy, particularly if combined with platinum-based chemotherapy, can be curative in patients with unresectable disease (2,3). Planning surgical treatment or radical radiotherapy involves staging the extent of locoregional disease in the thorax and excluding wider metastatic disease in appropriate patients.
Contrast-enhanced CT is the standard noninvasive method to stage cancer in the thorax and upper abdomen. However, both the negative and the positive predictive values of CT for staging cancer in the mediastinum have been relatively poor in most reported series (4). Unlike conventional CT, PET has been shown to have a high predictive accuracy, as verified surgically, for staging the locoregional extent of lung cancer (5,6). The spatial resolution of PET is generally insufficient to exclude small-volume disease, and false-positive results can occur as a result of inflammatory processes, yet PET has been shown to be substantially more accurate than CT in almost all comparative studies of the two, and there is evidence that the results of PET affect clinical decision making (5,7,8). Most series, however, have comprised primarily early-stage disease suitable for curative surgery and not the broad spectrum of disease seen at radiation oncology facilities.
In this article, we detail our analysis of 153 consecutive patients undergoing 18F-FDG PET for primary staging of recently diagnosed, non–small cell lung cancer for which either surgery or radiotherapy was being considered. This study looked at the ability of PET to affect patient management and, more important, to provide prognostic stratification as determined by survival.
MATERIALS AND METHODS
Patient Population
All patients referred for PET evaluation of suspected lung cancer between September 10, 1996, and December 21, 1998, were prospectively entered into a database. From this database, patients were eligible for this study if they had a new diagnosis of potentially curable and as yet untreated NSCLC. Patients were excluded if they had mixed tumors containing both NSCLC and small cell lung cancer. Patients with unresectable systemic metastases that had been confirmed on biopsy or on the basis of unequivocal conventional imaging appearances were also excluded. Some patients had undergone wedge resection of the primary lesions before the PET scan but were included if the mediastinum had not been dissected. In all, 153 patients met the eligibility criteria (102 men, 51 women; mean age ± SD, 66 ± 9 y). The histologic types were squamous cell carcinoma in 74 patients; adenocarcinoma in 54 patients; large cell carcinoma in 21 patients; and non–small cell carcinoma, not otherwise specified, in 4 patients.
During the study interval, limited availability of PET imaging slots meant that approximately only 70% of all patients referred to our hospital for potentially curative treatment could be scanned (9). Eligible patients were allocated PET imaging on the basis of first come, first served. Collection of impact data and outcome was approved by our institutional ethics committee. The scans were obtained as part of routine clinical practice at our institution.
PET Scan Acquisition and Processing
PET scans were acquired on a PENN-PET 300-H scanner (UGM Medical Systems, Inc., Philadelphia, PA). Emission data were processed using iterative reconstruction both with and without attenuation correction. The performance characteristics of this scanner and the processing methods have been described previously (10–12). The scan incorporated the lower neck, thorax, and upper abdomen for all patients but was extended to include any sites of equivocal abnormality on conventional staging. The brain was not included in the imaging field. An experienced nuclear medicine physician reviewed both image sets on a computer console, allowing interactive review of orthogonal slices. PET scans were reported in combination with the results of previous imaging and clinical information. Standard uptake values were not routinely calculated. Once issued, the PET scan report was entered into the database and was not reinterpreted in the light of subsequent clinical information.
Determination of Disease Stage
Staging was performed according to the 1997 update of the international staging system for lung cancer (13) and routinely involved CT with dynamic contrast material (unless contraindicated because of contrast allergy) and bone scanning in all but patients with asymptomatic stage IA disease. All routine staging investigations were reviewed at a weekly meeting of a multidisciplinary lung unit that included specialists on lung cancer staging and treatment. Although many of the CT scans were obtained in community practices before the patients were referred to our tertiary oncology facility, almost all scans were acquired using helical scanners and, unless deemed to be inadequate for treatment planning, were not repeated. CT or MRI of the brain was performed on only those patients for whom cerebral metastasis was clinically suspected. Each patient was assigned a pre-PET tumor, node, metastasis (TNM) stage on the basis of all available clinical conventional staging information. Mediastinal and hilar lymph nodes were regarded as positive for tumor on CT if they were >1 cm in maximum transverse diameter. When imaging findings were equivocal and could not readily be resolved (e.g., borderline enlargement of an adrenal gland), the patient was assigned the lower stage, and curative treatment, if otherwise appropriate, was planned to give the patient the benefit of the doubt. Equivocal findings were, however, recorded in the database to determine whether incremental PET findings were limited to confirmation of disease at these sites. After the PET scan, the patient was assigned a post-PET TNM stage that relied fully on the results of PET when there was discordance with other staging procedures. As with conventional staging investigations, equivocal PET abnormalities were considered negative and the patient was given the most favorable stage.
To simplify the presentation of data, we have not shown subclassification of stages into A and B groupings but, rather, have used broad groupings of stage (I–IV). The fine groupings were, however, recorded for each patient. Unless otherwise mentioned, the findings on statistical analysis for broad groupings were also pertinent to fine groupings.
Assessment of Impact
Our routine clinical request form asks clinicians to indicate what their management plan would be if PET were unavailable. This information, when available for the study participants, was entered into a database, and an oncologist experienced in managing lung cancer categorized the pre-PET treatment intent by synthesizing the available clinical and imaging information. For 42 patients (27%), a pre-PET treatment plan had not been recorded on the request form, and we relied on the patient’s pre-PET medical record and discussions with the referring clinician. In this manner, we could determine a pre-PET plan of management and treatment intent for all patients. The post-PET plan and intent was determined from the medical record or direct contact with the referring clinician. In all but 3 patients, the treatment delivered corresponded to the treatment planned after the PET result became available. One patient refused the recommended treatment, and 2 others had medical conditions that precluded it.
The impact on management was considered high when the treatment intent or modality was changed (e.g., from palliative to curative treatment or from surgery to radiotherapy), medium when the method of treatment delivery was changed (e.g., a change in radiation treatment volume), and low when the PET results did not indicate a need for change. PET was considered to have had no impact when the management plan was not changed despite being inconsistent with the post-PET stage.
Follow-Up
When appropriate, details of the date and cause of death were obtained. For patients treated radically, the site or sites of first progression were recorded. Progression was defined as the enlargement of previous masses or the appearance of new lesions. Stable residual abnormalities within the thorax were not recorded as residual disease unless verified by pathologic analysis.
Statistical Methods
Survival was estimated using the Kaplan–Meier product-limit method and compared using the Cox proportional hazards regression model. When indicated, the models were stratified by treatment given. The prognostic significance of individual factors has been summarized using hazard ratios representing the death rate for a given group relative to a baseline group, and the significance of these factors was tested by measuring the change in the log likelihood associated with their removal from the model. To assess the prognostic value of incorporating the PET findings into the staging process, we compared estimated survival for the pre-PET stage with that for the post-PET stage. We also compared survival based on whether curative or palliative treatment was planned before and after PET. The 95% confidence interval (CI) is given for the main results. Unless otherwise specified, 2-sided probability values are reported with no adjustment for multiple comparisons, and group data are expressed as mean ± SE.
RESULTS
Survival was measured from the date of the staging PET scan to the date of death from any cause. The data were analyzed with a closeout (study censor) date of July 1, 1999. Thus, the potential follow-up interval from the date of the PET scan to the closeout date ranged from 6 to 34 mo (2.8 y), with a median of 17 mo (1.4 y). All but 2 (1%) of the 153 patients entered into the study had a known status at the closeout date. Both patients who were lost to follow-up before the closeout date had gone overseas. For the 2 patients who were lost to follow-up, survival was censored at the date of last contact. Both were free from disease progression at that time. For patients who were still alive at the study closeout, survival was censored at that date.
Comparison of Pre- and Post-PET Stages
The post-PET stage was different from the conventionally determined stage in 65 (42%) of 153 patients. When the subclassifications within stages were not considered, 10% of cases were downstaged, 58% remained at the same stage, and 33% were upstaged (Table 1). The probability of a change in stage did not appear to depend on the original stage (P = 0.35, test for trend). The presence of an equivocal finding on conventional staging did not alter the likelihood of stage migration after PET. When conventional staging was equivocal, 8% were downstaged and 33% upstaged by PET, compared with 12% downstaged and 32% upstaged by PET when conventional staging was definite (P = 0.69). Systemic metastases were, however, more likely to be detected in patients with locally advanced disease. Stage IV disease was found in 7 (11%) of 65 patients with stage I or II disease on conventional staging versus 19 (24%) of 80 patients with stage III disease (P = 0.034). Although patients with confirmed systemic metastases on conventional staging investigations were generally excluded from this study, 8 patients with potentially resectable disease, including isolated cerebral metastasis, were included. When subclassifications within stages were considered, stage migration was even greater, with 40% of cases being upstaged and 10% downstaged. This finding had some implications for therapeutic planning.
Comparison of Cancer Stage Before and After PET
Accuracy of PET
The accuracy of the post-PET stage could be assessed either by histopathology or by demonstration of progressive disease on serial imaging in 81 (53%) of 153 patients and was confirmed in 72 (89%) of these. Of the 32 patients for whom PET had a high impact on management, the post-PET stage was confirmed in 28 (88%). The 4 patients for whom the post-PET stage was incorrect were also incorrectly evaluated by conventional staging. For all patients whose PET findings were ignored, the stage of disease was validated by serial imaging (n = 9), histopathology (n = 4), or postmortem examination (n = 1). Most patients for whom PET altered the radiation treatment volume were not evaluable because the treatment volume was enlarged to include normal-sized nodes. However, follow-up validated the PET findings in all 15 assessable patients in this group, for whom areas of structural abnormality were excluded from the field on the basis of negative PET findings.
Impact of PET Results on Treatment Planning
The PET results were believed to have a high impact on 54 patients (35%). This group included 34 (22%) of 153 patients for whom the intent was changed from curative treatment to palliative treatment or to supportive care after PET showed more extensive disease than had been suspected clinically. Furthermore, 6 patients (4%) for whom only palliative therapy was initially considered suitable received curative treatment after PET suggested less extensive disease than conventional staging had suggested. Finally, in 14 patients (9%) the treatment modality was changed but not the treatment intent.
PET had a medium impact on 39 patients (25%) that primarily included changes in radiation treatment volume. PET had low impact on 46 patients (30%), whose treatment proceeded as planned because the PET results were concordant with the results of conventional staging investigations. For 14 patients (9%), PET was considered to have no impact, because additional information from PET was not used in treatment planning. In these 14 patients, the accuracy of PET was confirmed by clinical follow-up, which ended with death from progressive metastatic disease in all but 1 patient, from whom chest wall disease detected on PET was subsequently successfully resected after local progression.
Prediction of Survival by PET
Seventy-eight of the 153 patients were known to have died before the closeout date. For the whole study cohort, estimated survival at 1 y was 61% ± 4%, and estimated survival at 2 y was 37% ± 5%.
Estimated survival rates by the pre- and post-PET stages are illustrated in Figures 1 and 2. Prognostic stratification by PET was particularly evident in the first 12 mo after the PET scan. The unifactor analysis shows that the post-PET stage was a considerably stronger prognostic factor than the pre-PET stage (Table 2). Within the broad stage groups, each increase in the pre-PET stage was associated with an estimated average increase of 29% in the rate of death (95% CI, 3%–61%; P = 0.013), whereas each increase in the post-PET stage was associated with an estimated 69% average increase in the rate of death (95% CI, 34%–114%; P < 0.0001).
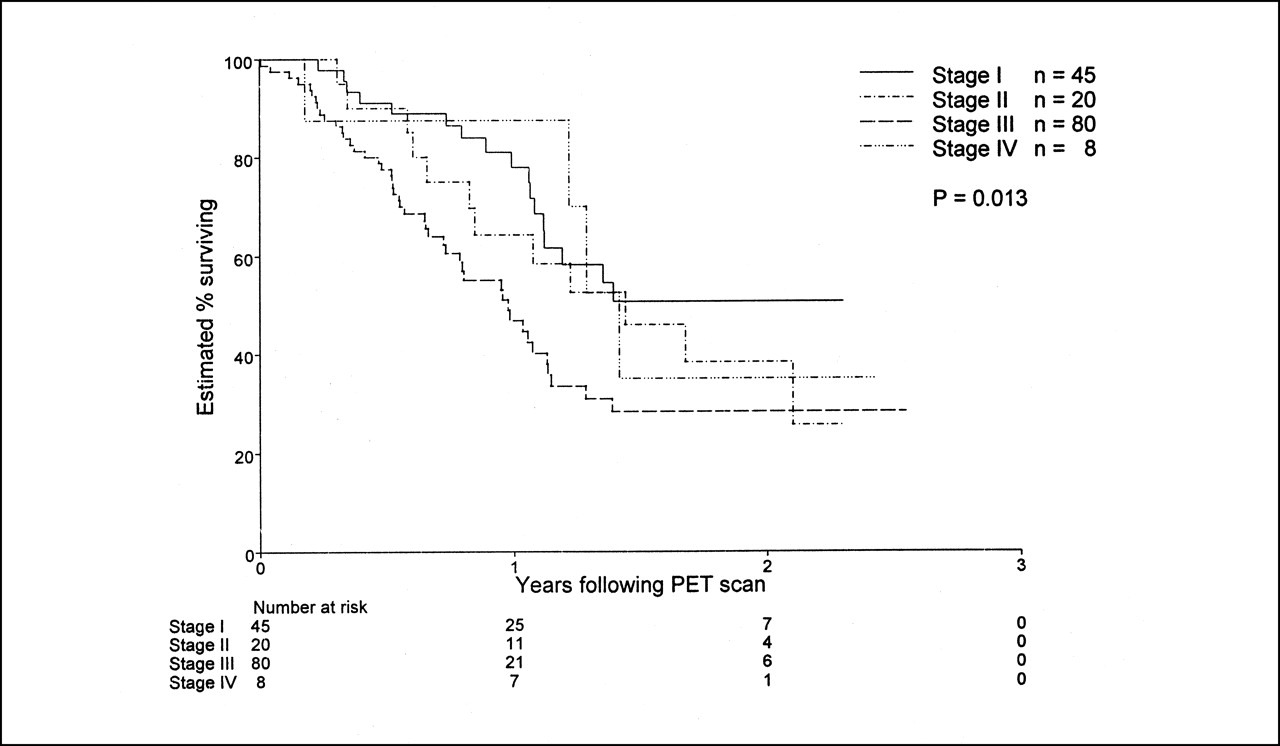
As expected, clinical stage as assessed by conventional staging techniques, primarily including dynamic contrast CT and bone scintigraphy, was significantly associated with survival in the 153 patients evaluated.
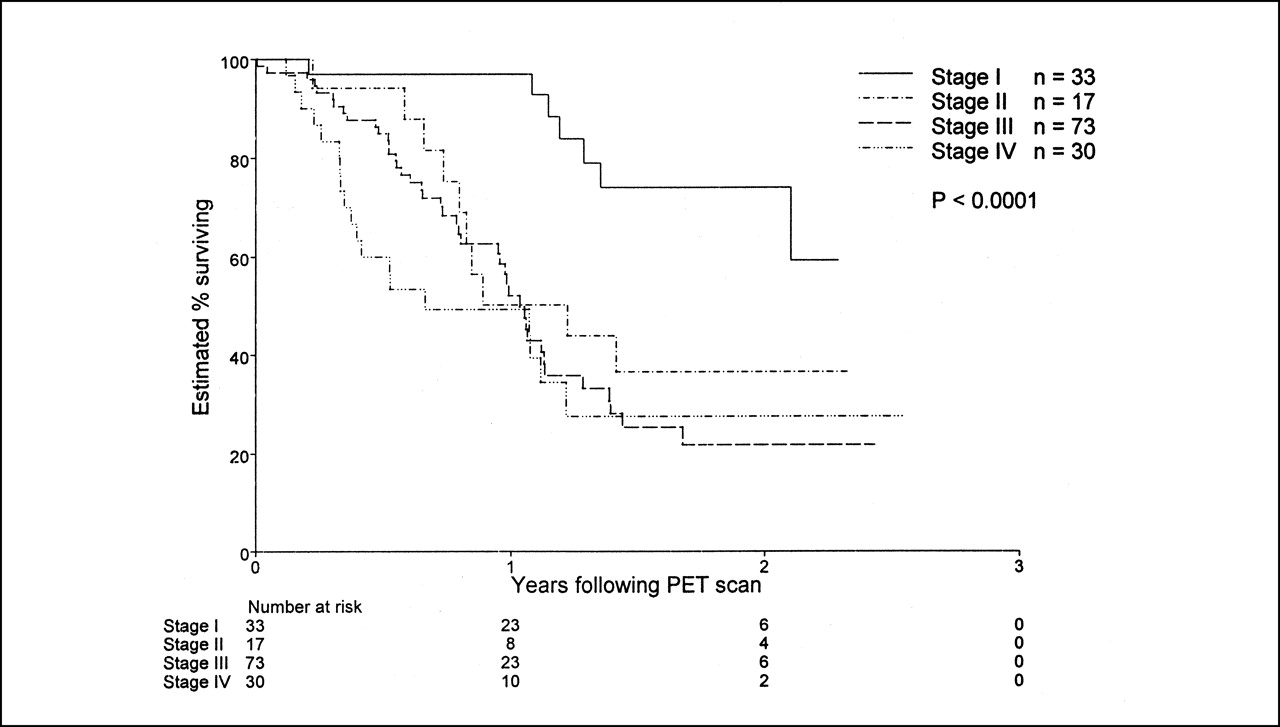
Assessment of survival by post-PET clinical stage, which incorporated FDG PET information, led to markedly stronger prognostic stratification than observed with conventional staging techniques. Early separation of each clinical stage suggests more accurate definition of disease burden.
Unifactor Analysis of Overall Survival
The superior prognostic stratification by PET was confirmed by the multifactor analysis looking at the joint significance of the pre- and post-PET stages. Each increment in pre-PET stage increased the death rate by an estimated average of 6%, compared with an estimated average 66% increase in death rate for each increment in post-PET stage. After adjustment for the post-PET stage, the pre-PET stage was not significantly associated with survival (P = 0.64), whereas after adjustment for the pre-PET stage, the post-PET stage remained highly significantly associated with survival (P = 0.0001). After adjustment for treatment given, each increase in the pre-PET stage was associated with an estimated average increase of 14% in the rate of death (95% CI, 11% decrease to 45% increase; P = 0.14), whereas each increase in the post-PET stage was associated with an estimated average 46% increase in the rate of death (95% CI, 10%–94%; P = 0.0035).
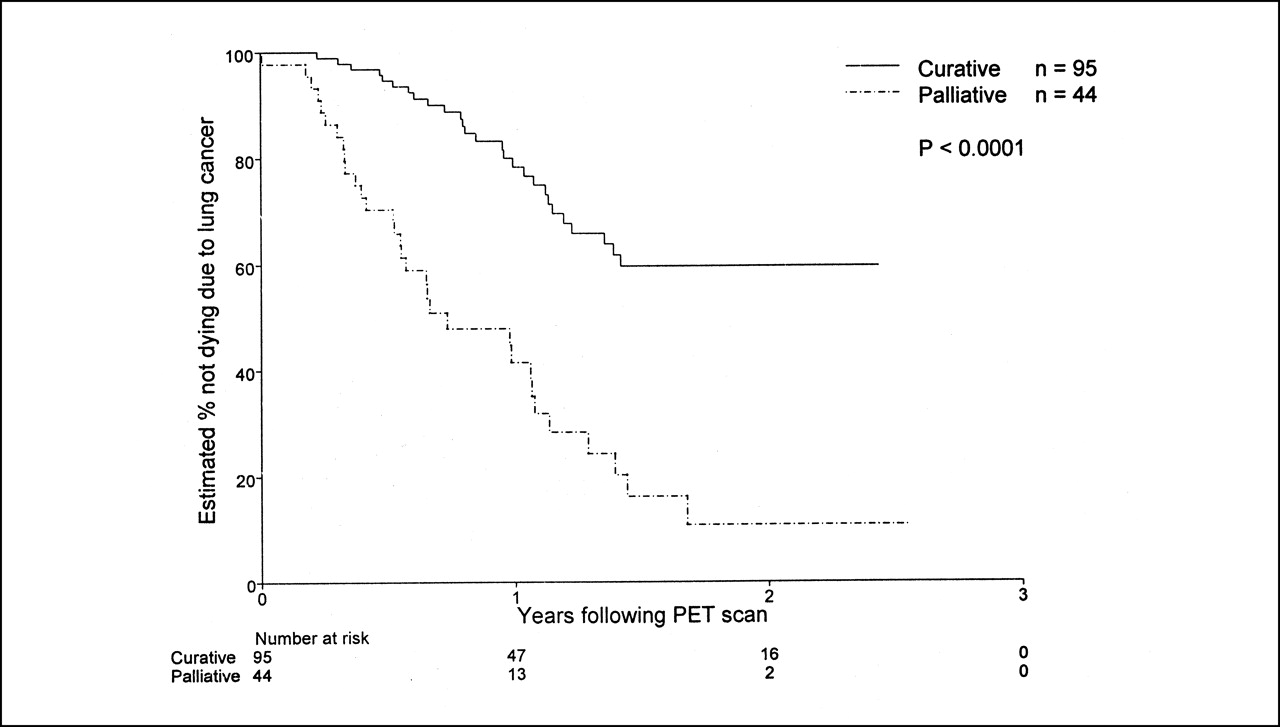
After the PET results became available, only 109 patients (71%) were considered by the referring clinician to have disease suitable for curative treatment, whereas 44 (29%) were considered to have disease suitable for only palliative treatment. The treatment intent after PET was highly predictive of survival, with the death rate for the palliative group being an estimated 2.6 times that of the curative group (P < 0.0001) (Table 3). Excess deaths occurred in the group receiving palliative care, starting early after the PET scan (Fig. 3).

After PET, only 109 patients received curative treatment whereas 44 received palliative radiotherapy. These 44 included 34 whose treatment was changed from curative after PET showed more extensive disease than expected. Marked difference in survival was noted between these groups.
Association Between Post-PET Treatment Intent and Survival
A potentially more powerful comparison of the prognostic significance of PET was obtained by excluding the 14 patients for whom the treatment plan was not changed despite being inconsistent with the PET stage and by censoring the survival durations for the 8 patients who died without disease progression. An even more striking difference in survival duration was found between the post-PET palliative patients and the curative patients (estimated hazard ratio, 4.11; P < 0.0001) (Fig. 4).
Of 109 patients who received curative treatment, 14 had PET findings suggesting that palliative treatment ought to have been given. Giving curative rather than palliative treatment to this group may have adversely affected its survival. Excluding these patients from analysis showed even more dramatic difference in survival between curative and palliative groups.
DISCUSSION
Like previous studies (14), this study showed that PET findings result in a change in stage in a substantial proportion of patients. Stage migration occurred across all conventional stage groupings. By detecting more extensive disease than was clinically suspected, the PET findings led to a change in broad stage grouping in 33% of patients and a change from curative to palliative treatment in 22% of patients (Fig. 5). By suggesting the presence of false-positive structural imaging results, the PET findings allowed downstaging in 10% of patients and delivery of potentially curative therapy. In addition to these changes in treatment intent, changes in treatment modality or in delivery of a chosen treatment occurred as a result of a change in the assessment of disease extent, including cases in which PET did not alter the stage classification. These data confirm and expand our findings from an earlier prospective trial (15).

Example of high-impact study. This patient was assessed as having stage IIB disease on basis of CT findings and was being considered for radical radiotherapy. In addition to confirming mediastinal nodal disease (vertical arrow), PET showed previously unrecognized metastases on left adrenal (oblique arrow) and dome of right hepatic lobe (horizontal arrow). Accordingly, patient received only palliative radiotherapy. Follow-up confirmed progressive systemic metastasis within 6 mo.
Overall, PET altered management in 61% of patients. Our findings extend the evidence that PET findings affect clinical decision making in surgical candidates (5,7,8) to a broader spectrum of lung cancer patients typical of a tertiary oncology facility providing radiation oncology services. This information is important because only a minority of patients with newly diagnosed NSLC are suitable for surgery. A recently published survey relating to the treatment of lung cancer within the population served by our facility found that surgery was performed on only 30% of all patients with newly diagnosed non–small cell lung cancer, whereas slightly more than 50% received radiotherapy as part of their treatment (16).
Previous studies have generally used pathologic staging as the gold standard to validate CT and PET findings. A recent metaanalysis supported the superior accuracy of PET, in comparison with CT, for preoperative staging of mediastinal nodal status (17), and a recent prospective study found unrecognized systemic metastases in 11% of patients who were determined, by conventional staging, to have resectable disease (18). However, because our population included many patients unsuitable for surgery, pathologic validation was not available for the majority of the cohort. Rather, we relied on clinical follow-up and survival data to assess the validity of PET findings and the appropriateness of management changes.
Because a long sequence of events intervenes between a diagnostic test and a clinical outcome, documentation of changes in outcome is often difficult even with accurate tests. Despite this potential limitation, our findings still strongly suggest that PET results are highly predictive of survival whereas conventional staging offers only modest prognostic stratification. This stratification (Figs. 2–4) by PET was clearly evident starting early in the follow-up period, suggesting that the differing survival reflects the effect of correctly identifying patients with a poor prognosis based on the extent of their disease rather than the effect of assigning patients to a less efficacious therapy. This suggestion is consistent with the analysis adjusting for treatment given, in which the post-PET stage was still a highly significant prognostic factor. Because long-term survival depends not only on the accuracy of staging but also on the effectiveness of available therapies, the convergence of survival curves over time for patients in whom PET showed more advanced disease (Fig. 2) may well reflect the limitations of currently available therapies rather than the failure of imaging to correctly determine disease stage and, therefore, long-term prognosis.
Our clinical follow-up and survival data suggest that management changes influenced by PET findings were usually appropriate. Patients who received palliative treatment based on PET findings had an excess early mortality consistent with a higher disease burden and were spared the toxicity of what would likely have been futile aggressive treatment. The benefit from modifying radiation treatment volumes to incorporate areas found to be abnormal by PET but not by CT cannot be independently assessed by this study, but intuitively, failure to treat active sites of disease ought to be detrimental. The poor outcome of patients with untreated abnormalities found by PET but not verified by other techniques suggests that the positive predictive value of PET is probably sufficient to justify management changes without resorting to pathologic confirmation in all instances. Further, on the basis of Bayesian principles, the likelihood that additional PET-detected abnormalities are true-positive would be expected to increase in concert with increasing extent of locoregional disease (9).
This study did not provide information on the independent role of PET compared with conventional staging, because the PET results were interpreted along with other clinical information and not in a masked manner. Rather, the study looked at the incremental diagnostic information provided by PET and its impact on patient management in routine clinical practice. Although the conventional staging methods, including CT, were not standardized, their results had been judged adequate to guide specialists in lung cancer management in consultation with radiologic experts on lung cancer diagnosis and staging. This is consistent with usual clinical practice at a tertiary oncology facility.
This study could not evaluate the true accuracy of PET and conventional staging because not all discordant results were verified through biopsy. Accordingly, some of the results of mediastinal staging may have been falsely positive because of granulomatous disease. However, in the population served by our PET facility, the incidence of tuberculosis is low and histoplasmosis is not endemic. Analysis of our surgical patients has yielded a false-positive rate of <5% (R. Hicks, unpublished data, 2000) for mediastinal lymph node involvement. False-positive results outside the thorax appear to be even less common. Nevertheless, no patient was denied potentially curative surgery purely on the basis of PET findings. In patients whose disease had already been deemed inoperable because of the CT findings, or who could not undergo surgery because of coexistent disease, surgical staging purely to determine the accuracy of PET before radiotherapy was deemed inappropriate. In patients for whom the PET treatment volume was increased to incorporate PET-positive but CT-negative disease, treatment is likely to have altered the natural history of these sites. The subgroup of patients for whom PET findings were ignored because they could not be independently confirmed by imaging or biopsy provided the greatest insight on the relative accuracies of PET and conventional staging. In all 14 patients for whom PET revealed abnormalities outside the surgical field or radiation treatment volume, progressive disease was subsequently documented, and 13 of these patients died of distant metastatic disease. Overall, the accuracy of PET could be verified in 72 (89%) of 81 evaluable patients, including 57 (93%) of the 61 for whom PET did alter or should have altered management.
The most rigorous determination of the impact of PET on patient outcome would be a randomized trial comparing patient cohorts staged with and without PET. On the basis of the current evidence of the superior diagnostic accuracy of PET, in comparison with CT, our institutional clinical research committee deemed it unethical to deny patients either PET scanning, if it would otherwise be available to them, or the results thereof. The applicability of randomized controlled trials to diagnostic procedures has also recently been questioned (19). Nevertheless, preliminary data on such a trial in surgical patients show a reduction in unnecessary thoracotomies (20).
CONCLUSION
These data suggest that, when added to conventional staging techniques, PET provides incremental staging information that more accurately stratifies prognostic risk and highly influences treatment delivery. By allowing patients with a poor prognosis to be converted from futile curative therapy, PET spares them unwarranted morbidity and spares the community the costs associated with such treatment. The role of PET scanning is not limited to surgical candidates but provides useful information also for patients scheduled for radiotherapy.
Acknowledgments
The authors thank the cyclotron staff of the Peter MacCallum Cancer Institute and the Austin & Repatriation Medical Centre (Melbourne, Australia) for providing a reliable supply of FDG and the referring clinicians for providing follow-up information. The authors are also grateful for the tireless efforts of their technologist and secretarial staffs to continually do more with less. This study was supported by a grant from the Consultative Committee for Diagnostic Imaging on behalf of the Australian Department of Health and Aged Care.
Footnotes
Received Feb. 22, 2001; revision accepted Jul. 16, 2001.
For correspondence or reprints contact: Rodney J. Hicks, MD, Centre for Positron Emission Tomography, Peter MacCallum Cancer Institute, 12 Cathedral Pl., East Melbourne, Victoria 3002, Australia.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- 18F-FDG-Avid Thyroid Incidentalomas: The Importance of Contextual Interpretation
- The Injustice of Being Judged by the Errors of Others: The Tragic Tale of the Battle for PET Reimbursement
- Lung cancer survival in Norway, 1997-2011: from nihilism to optimism
- 15-Year Experience of 18F-FDG PET Imaging in Response Assessment and Restaging After Definitive Treatment of Merkel Cell Carcinoma
- 18F-FDG PET Provides High-Impact and Powerful Prognostic Stratification in the Staging of Merkel Cell Carcinoma: A 15-Year Institutional Experience
- Let's Get SEERious: More Accurate Staging With Consequent High Management Impact Is Not Just Stage Migration
- Effect of PET/CT on Management of Patients with Non-Small Cell Lung Cancer: Results of a Prospective Study with 5-Year Survival Data
- 18F-FDG PET/CT Has a High Impact on Patient Management and Provides Powerful Prognostic Stratification in the Primary Staging of Esophageal Cancer: A Prospective Study with Mature Survival Data
- Doing More Harm than Good? Do Systematic Reviews of PET by Health Technology Assessment Agencies Provide an Appraisal of the Evidence That Is Closer to the Truth than the Primary Data Supporting Its Use?
- Impact of Tumor Size and Tracer Uptake Heterogeneity in 18F-FDG PET and CT Non-Small Cell Lung Cancer Tumor Delineation
- 18F-FDG PET/CT for the Prediction and Detection of Local Recurrence After Radiofrequency Ablation of Malignant Lung Lesions
- Are Health Economics Making Us Sick?
- Primary Analysis of the Phase II Component of a Phase I/II Dose Intensification Study Using Three-Dimensional Conformal Radiation Therapy and Concurrent Chemotherapy for Patients With Inoperable Non-Small-Cell Lung Cancer: RTOG 0117
- From RECIST to PERCIST: Evolving Considerations for PET Response Criteria in Solid Tumors
- Bone Marrow Hypermetabolism on 18F-FDG PET as a Survival Prognostic Factor in Non-Small Cell Lung Cancer
- Microvessel Density: Correlation with 18F-FDG Uptake and Prognostic Impact in Lung Adenocarcinomas
- Etiology of Solitary Extrapulmonary Positron Emission Tomography and Computed Tomography Findings in Patients With Lung Cancer
- The Role of PET Scan in Diagnosis, Staging, and Management of Non-Small Cell Lung Cancer
- In Vitro Proton Magnetic Resonance Spectroscopic Lactate and Choline Measurements, 18F-FDG Uptake, and Prognosis in Patients with Lung Adenocarcinoma
- Quantification of 18F-FDG Uptake in Non-Small Cell Lung Cancer: A Feasible Prognostic Marker?
- {gamma}-Camera 18F-FDG PET in Diagnosis and Staging of Patients Presenting with Suspected Lung Cancer and Comparison with Dedicated PET
- American Society of Clinical Oncology Treatment of Unresectable Non-Small-Cell Lung Cancer Guideline: Update 2003
- Implementing Biologic Target Volumes in Radiation Treatment Planning for Non-Small Cell Lung Cancer
- Imaging Proliferation in Lung Tumors with PET: 18F-FLT Versus 18F-FDG
- Lung cancer * 7: Management of lung cancer in elderly patients
- Use of a Dual-Head Coincidence Camera and 18F-FDG for Detection and Nodal Staging of Non-Small Cell Lung Cancer: Accuracy as Determined by 2 Independent Observers
- 18F-FDG PET in Candidates for Radiation Therapy: Is It Important and How Do We Validate Its Impact?
- 3-Deoxy-3-[18F]Fluorothymidine-Positron Emission Tomography for Noninvasive Assessment of Proliferation in Pulmonary Nodules