


Abstract
The purpose of this study was to retrospectively predict the chemotherapeutic response to paclitaxel for non–small cell lung cancer (NSCLC) using 99mTc-tetrofosmin (TF) uptake and to detect the expression of 170-kDa multidrug resistance–mediated P-glycoprotein (MDR-Pgp). Methods: Before chemotherapy with paclitaxel, 20 patients with stage IIIb or IV NSCLC were enrolled in this study to undergo early and delayed 99mTc-TF chest imaging for calculating tumor-to-normal lung ratios (T/NL) and retention indices (RI) for assessment of the MDR-Pgp in NSCLC. Results: The early and delayed mean T/NLs were 1.59 ± 0.25 and 1.50 ± 0.25, respectively, for 10 patients with a good response and 1.09 ± 0.09 and 1.03 ± 0.05, respectively, for 10 patients with a poor response. The differences were shown to be significant (P < 0.001) by independent Student t tests. However, no significant differences (P = 0.801) between good-response patients (−5.70% ± 3.67%) and poor-response patients (−5.23% ± 4.51%) were found in RI. In addition, other prognostic factors (age, sex, tumor size, stage, and cell type) were not significantly different between good-response patients and poor-response patients. Conclusion: 99mTc-TF chest images are potential tools for understanding MDR-Pgp expression in NSCLC and for predicting the chemotherapeutic response to paclitaxel.
The majority of patients with non–small cell lung cancer (NSCLC) present with disease that is beyond the scope of surgical cure. Despite having few or no symptoms, 60%–70% of newly diagnosed patients have locally advanced, inoperable, or distant metastatic disease. Recently, evidence has been put forward that chemotherapy does have a role in unresectable NSCLC (stage IIIb or IV) (1,2).
Recent articles have reported that the multidrug resistance–1 (MDR1) gene encoding human multidrug resistance–mediated P-glycoprotein (MDR-Pgp) may play an important role in the multidrug resistance of lung cancer (3,4). The ideal therapeutic goal in advanced NSCLC is to achieve the highest response with the lowest possible morbidity from the side effects of chemotherapy. Therefore, some investigators have suggested that determinations of MDR-Pgp at the time of diagnosis may provide valuable information for the design of treatment protocols (5–7). A review of the literature indicates that P-glycoprotein recognizes certain chemotherapeutic agents as substrates and prevents the accumulation of some lipophilic cationic radiopharmaceuticals such as 99mTc-tetrofosmin (TF). Some investigators have found negative and positive 99mTc-TF tumor uptake to be consistent with relatively high and low expressions, respectively, of MDR-Pgp (8–12). In addition, recent attempts using 99mTc-TF to detect lung cancer have been successful (13–19).
In a previous study, we depended on this theory to successfully predict the chemotherapeutic response to cisplatin and etoposide in small cell lung cancer in humans (20). However, to our knowledge, no study using 99mTc-TF chest images to predict the chemotherapeutic response to paclitaxel (Taxol; Bristol-Myers Squibb Co., Princeton, NJ) in NSCLC patients has been reported in the literature. Therefore, the aim of this study was to explore the potential role of 99mTc-TF chest imaging in predicting the NSCLC patient response to chemotherapy with paclitaxel.
MATERIALS AND METHODS
Patients
Twenty patients (13 men, 7 women; age range, 43–70 y) with advanced NSCLC (stage IIIb or IV), including eight cases of squamous cell carcinoma and 12 of adenocarcinoma, who were to undergo chemotherapy for bronchogenic carcinoma were enrolled in this study. The dose of paclitaxel was 135 mg/m2 as a 3-h infusion on day 1, and 75 mg/m2 cisplatin was given on day 2. The regimen was repeated every 3–4 wk for up to six to eight cycles unless tumor progression was evident (21). The patients were required to provide a complete history and undergo physical examination. Patient enrollment criteria included no prior chemotherapy, radiotherapy, or surgery; an Eastern Cooperative Oncology Group performance status of 0–2; adequate hematologic (granulocyte count ≥ 1500/μL, platelet count > 100000/μL), hepatic (bilirubin ≤ 1.25 × the upper normal limit), and renal (serum creatinine ≤ 1.25 × the upper normal limit) functions; and adequate cardiac function, with no active arrhythmia or congestive heart failure. All patients were premedicated with dexamethasone (20 mg), cimetidine (300 mg), and diphenhydramine (50 mg) before initiation of the paclitaxel infusion (21,22). Paclitaxel was well tolerated, and none of the patients experienced an allergic reaction. Granulocytopenia was generally mild. Before chemotherapy, early and delayed 99mTc-TF chest imaging was performed on all patients to evaluate MDR-Pgp.
Interpretation of Chemotherapy Response
The response of NSCLC to chemotherapy was evaluated clinically and radiologically within 4 wk after the last treatment (23). In our study, modified evaluation criteria were used (19). A good response was a 50% or greater decrease in the sum of the products of the maximum perpendicular diameters of all measurable lesions and no new lesions. A poor response was less than a 50% decrease in the sum of the products of the maximum perpendicular diameters of all measurable lesions or the appearance of new lesions.
99mTc-TF Chest Imaging
A commercial 99mTc-TF preparation was obtained (Myoview; Amersham International plc, Buckinghamshire, UK). The labeling and quality control procedures were performed according to the manufacturer’s instructions. The radiochemical purity of 99mTc-TF used in this study was consistently higher than 90%. The chest images were obtained 10 min and 2 h after intravenous injection of 740 MBq (20 mCi) 99mTc-TF. Each patient was positioned supine on the imaging table with the chest strapped to prevent motion. The equipment consisted of a rotating, large-field-of-view dual-head gamma camera (Helix HR; Elscint, Haifa, Israel) fitted with a low-energy, high-resolution general-purpose collimator (HPC 46; Elscint). A single 20% energy window was set at 140 keV. Then, the anterior and posterior views of the chest were obtained simultaneously.
The findings from 99mTc-TF chest images were evaluated quantitatively as follows. (1) The tumor-to-normal lung (T/NL) ratio was obtained on early and delayed chest images. Based on chest radiography findings, two regions of interest (ROIs) with the same size were carefully drawn over the tumor on the anterior and posterior views. Then, another two ROIs of the same size were drawn over the contralateral normal lungs on both the anterior and posterior views using a mirroring technique. The T/NLs were calculated using the following formula with geometric mean counts of the anterior and posterior counts: [(the mean counts in the ROI over the tumor in the anterior view)1/2 × (the mean counts in the ROI over the tumor in the posterior view)1/2]/[(the mean counts in the ROI over the contralateral normal lung in the anterior view)1/2 × (the mean counts in the ROI over the contralateral normal lung in the posterior view)1/2] (2) The retention index (RI) was calculated by the following formula: [(delayed T/NL − early T/NL) × 100]/early T/NL (20). The values of T/NL and RI were expressed as the mean ± SD. To test for differences between these parameters, an independent Student t test was used.
RESULTS
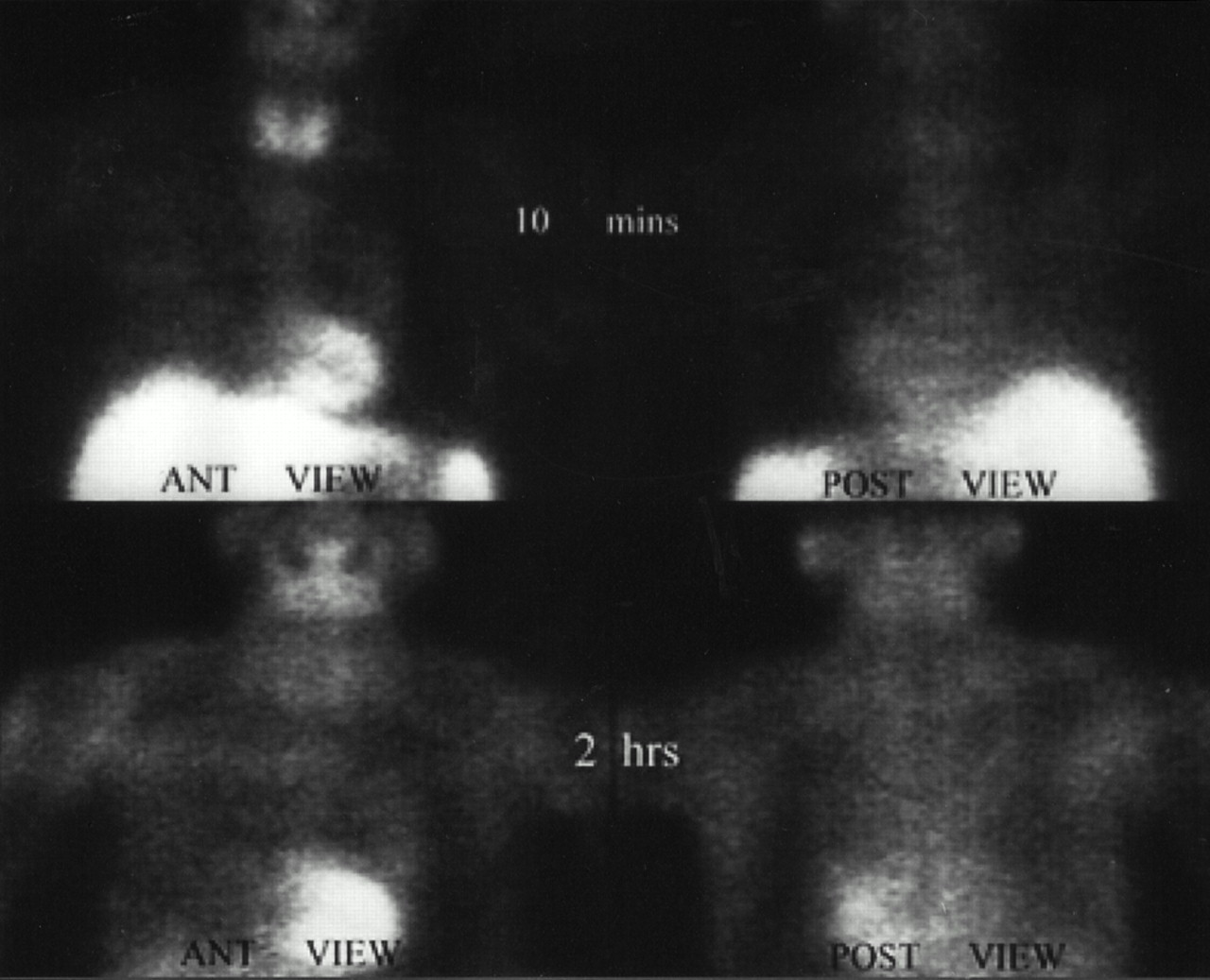
Detailed patient data are shown in Table 1. The mean early and delayed T/NLs of the 99mTc-TF chest images of patients with a good response were 1.59 ± 0.25 and 1.50 ± 0.25, respectively, and those of patients with a poor response were 1.09 ± 0.09 and 1.03 ± 0.05, respectively. Both early and delayed T/NLs in good-response patients (Fig. 1) were significantly higher than those in poor-response patients (Fig. 2) (P < 0.001). The RI of 99mTc-TF chest images in patients with a good response was −5.70% ± 3.67%, and that in patients with a poor response was −5.23% ± 4.51%. However, the difference in RI was not significant (P = 0.801).
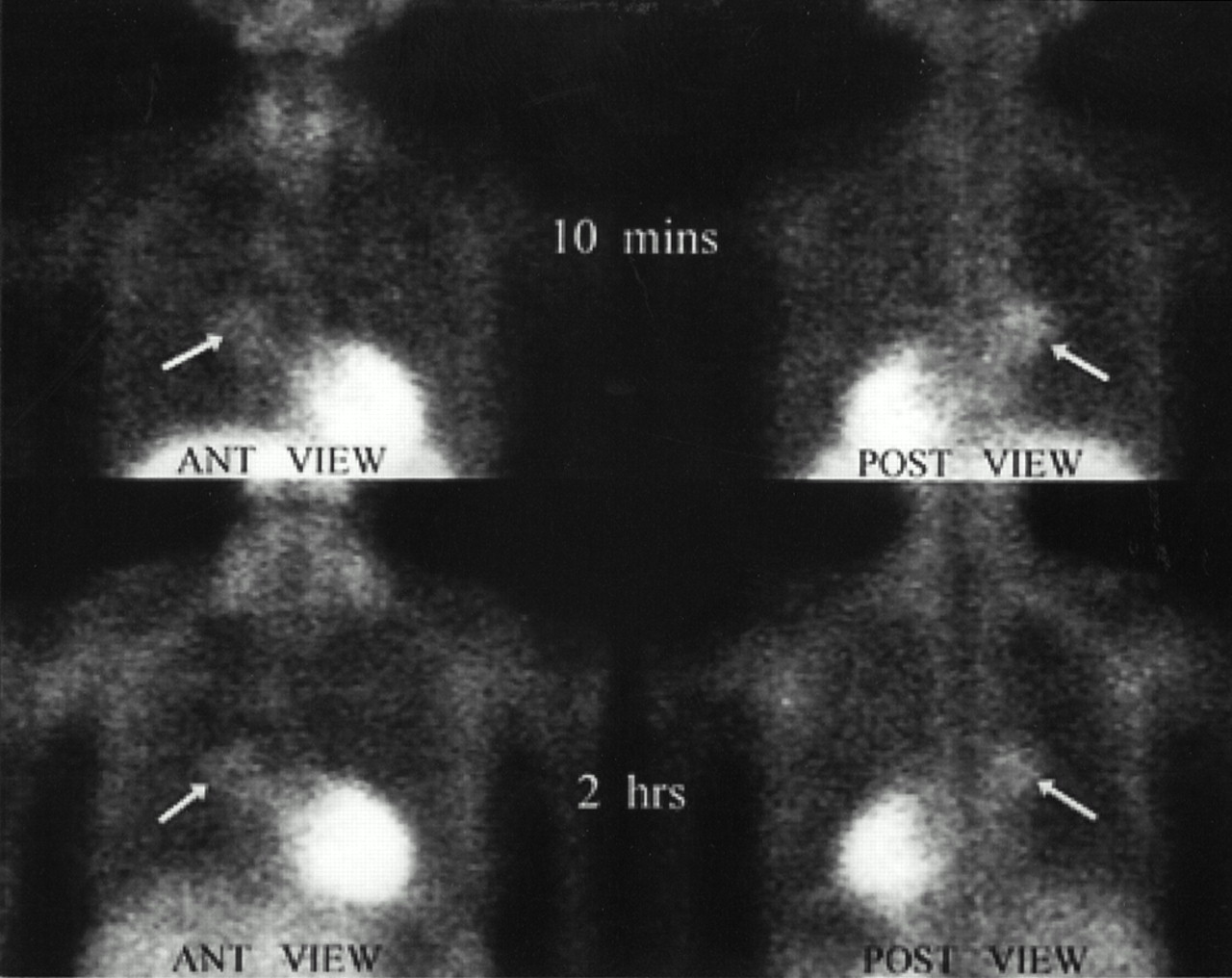
In patient 1, who had good response to paclitaxel, both early and delayed anterior and posterior 99mTc-TF chest images show significant 99mTc-TF uptake by lung cancer (arrows).
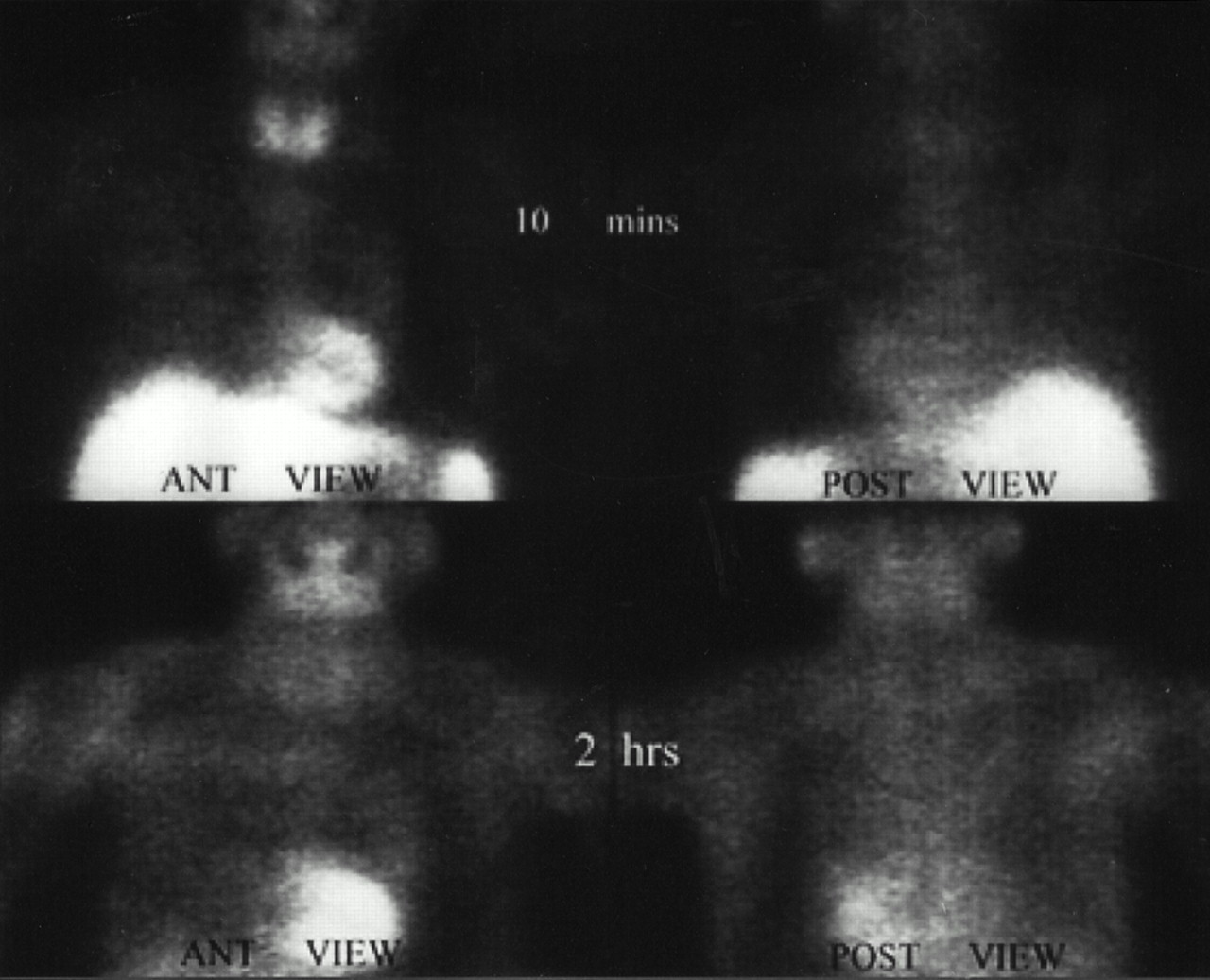
In patient 11, who had poor response to paclitaxel, both early and delayed anterior and posterior 99mTc-TF chest images show no definite 99mTc-TF uptake by lung cancer.
Patient Data
We compared the differences between other prognostic factors, including sex, age, tumor size, stage, and cell type, in the good-response and poor-response patients. No significant differences were found (P > 0.05 for each factor).
DISCUSSION
The taxanes are an important new class of anticancer agents that promote polymerization of cellular microtubules, preventing mitosis and resulting in cell death. Investigators from the Eastern Cooperative Oncology Group and M.D. Anderson Cancer Center, Houston, TX, administered paclitaxel, the first taxane for treating NSCLC (1,2), to previously untreated patients with stage IV NSCLC. Both groups observed objective response rates of more than 20%. These represent the highest response rates against NSCLC achieved in any drug discovery phase II trial conducted by the Eastern Cooperative Oncology Group during the past 10 y using similar study populations (1,22). However, many toxic reactions, such as leukopenia, hypersensitivity reactions, neurotoxicity, mucositis, alopecia, diarrhea, myalgias, and cardiac toxicity, were encountered during the clinical trials of paclitaxel (24,25). The mechanism of acquired resistance to paclitaxel is conferred by a multidrug-resistant phenotype that involves amplification of membrane P-glycoprotein and reduced ability to accumulate and retain paclitaxel because of the energy-dependent P-glycoprotein efflux pump, which has a central role in the transport of chemotherapy drugs through the cell membrane (26–28). Therefore, to achieve a satisfactory response, one must understand the presence of MDR-Pgp in NSCLC before initiating chemotherapy with paclitaxel.
In reports in the literature, 99mTc-TF chest images used for detecting lung cancer have shown large variations in sensitivity, specificity, and accuracy. Some studies dealing with 99mTc-TF chest images for the detection of lung cancer have been published (13–18). In these studies, the sensitivity has ranged from 77% to 90%. The discrepancies between the results of our recent study, which had a diagnostic sensitivity of 61% (19), and the results of these publications (13–18) are difficult to explain. One possible explanation may be differences in case selection criteria with varying MDR-Pgp expression (8–12). The retention of 99mTc-TF in cancer cells depends on the activity of the 170-kDa P-glycoprotein coded on the MDR1 gene, which functions as an adenosine triphosphate–dependent efflux pump for many chemotherapy drugs. Mostly lipophilic cations, such as 99mTc-TF, have also been reported to be ligands for this MDR-Pgp (8–12), because accumulation of the complex in cancer cells has been reported to be inversely related to the level of MDR-Pgp.
In our study, low T/NLs on 99mTc-TF chest images indicated resistance to paclitaxel and a poor response, whereas patients with high T/NLs had a good chemotherapy response to paclitaxel. Low and high T/NLs have been thought to be consistent with relatively high and low expressions of MDR-Pgp and the mechanism of resistance to paclitaxel chemotherapy because of MDR-Pgp overexpression (26–28). Therefore, we used semiquantitative 99mTc-TF chest images to accurately predict the response to chemotherapy with paclitaxel. Although quantification of MDR-Pgp molecules with other conventional methods was not performed, our findings were supported by the results of previous studies in vitro (8–12).
In this study, we calculated T/NLs from planar chest images instead of SPECT images, because the method used has been published and can easily be practiced clinically (20,29). Although the advantage of SPECT is the absence of superimposition of counts of an ROI on surrounding tissue, we chose not to use SPECT because SPECT images after reconstruction have modified the real counts in ROIs and because selection of SPECT slices for summation is often difficult.
CONCLUSION
Our results emphasize the importance of pretreatment chest imaging with 99mTc-TF for predicting the chemotherapeutic response to paclitaxel more accurately than is possible through other factors, such as sex, age, tumor size, stage, and cell type. In accordance with our findings, a low T/NL in advanced NSCLC may mean that selection of an expensive paclitaxel treatment protocol is not necessary.
Acknowledgments
This study was supported in part by grants from the National Science Council, Taipei, Republic of China (NSC88-2314B-075A-006), and Taichung Veterans General Hospital (TCVGH-886705C).
Footnotes
Received Mar. 3, 2000; revision accepted Jul. 28, 2000.
For correspondence or reprints contact: Chia-Hung Kao, MD, Department of Nuclear Medicine, Taichung Veterans General Hospital, 160 Taichung Harbor Rd., Section 3, Taichung, Taiwan.




{kind=link}
{kind=link}