


Abstract
In patients with non–small cell lung cancer (NSCLC), surgical resection offers the best chance of cure. The preoperative assessment of mediastinal lymph node involvement is crucial to selecting those patients for whom surgery is indicated. Methods: To evaluate the possible clinical role of 99mTc-tetrofosmin scintigraphy in the presurgical detection of mediastinal node metastases from NSCLC, we performed a prospective comparative study with CT on 83 patients (48 men, 35 women; age range, 38–81 y) with primary NSCLC (36 adenocarcinomas, 39 epidermoid squamous cell carcinomas, and 8 large cell anaplastic carcinomas). They underwent chest SPECT 20 min after 99mTc-tetrofosmin injection (740 MBq intravenously). The metastatic involvement of mediastinal nodes was assessed by histologic examination after mediastinoscopy or thoracotomy. Both chest CT and 99mTc-tetrofosmin scintigraphy were performed within 2 wk before the surgical staging. Results: Metastatic mediastinal lymph nodes were found in 35 patients. 99mTc-Tetrofosmin imaging in assessing the mediastinal involvement yielded a sensitivity of 85.7%, a specificity of 89.6%, and an accuracy of 88.0%; CT results were 68.6%, 75.0%, and 72.3%, respectively. SPECT accuracy was significantly higher than CT accuracy (P < 0.05). However, precise anatomic localization of 99mTc-tetrofosmin uptake in the mediastinum was not always present on SPECT images. 99mTc-Tetrofosmin SPECT precisely detected the presence or absence of lymph node metastases in 33 of the 36 patients with positive CT findings (enlarged mediastinal nodes with a short axis ≥ 1 cm), with an accuracy (91.7%) significantly higher (P < 0.05) than that of CT (66.7%). Conclusion: 99mTc-Tetrofosmin SPECT is a useful presurgical noninvasive method to assess mediastinal lymph node involvement in NSCLC. In particular, it could play a clinical role in reducing the number of invasive staging surgical procedures in selected patients, especially in those with enlarged lymph nodes at CT. Fusing SPECT with CT images could further improve the interpretation of the scintigraphic data.
Lung cancer is one of the major causes of death in many countries, both in women and in men (1). Non–small cell lung cancer (NSCLC) is the most frequent histologic type: early detection and radical surgery offer the best chance of cure for patients (2). Accurate preoperative tumor staging is important for selecting those patients who are likely to benefit from surgery. In particular, the evaluation of mediastinal lymph node metastases is crucial for the assessment of the resectability of the primary tumor and therefore for disease prognosis (3); patients with preoperative mediastinal metastases at mediastinoscopy should preferably enter a multimodality treatment, including induction chemotherapy followed by a definitive locoregional treatment, either surgery or radiation therapy or both (4,5).
Chest CT is the most commonly used noninvasive imaging method for mediastinal staging in NSCLC, but its limits are widely acknowledged: The criterion used for diagnosis is based only on lymph node size, and thus it is less accurate than that used in invasive surgical staging (6,7). Therefore, there is a need for noninvasive imaging methods able to accurately assess metastatic mediastinal involvement in patients with NSCLC and thus reduce the number of staging mediastinoscopies and mediastinotomies and avoid unnecessary thoracotomies (8).
Nuclear medicine procedures have also been used in NSCLC staging; some authors (9) have demonstrated the usefulness of 18F-FDG PET in the preoperative assessment of patients affected by this type of cancer, also suggesting that the addition of this procedure to conventional imaging methods can improve the selection of surgically curable patients (9). The usefulness of some myocardial perfusion imaging tracers such as 201Tl (10,11) and 99mTc-sestamibi (12,13) has also been reported in mediastinal lymph node detection using SPECT acquisition; in particular, recent data have demonstrated a higher specificity and accuracy for 99mTc-sestamibi SPECT than for CT, but a lower sensitivity (13).
More recently, another cationic lipophilic complex, 99mTc-tetrofosmin, largely used for myocardial perfusion scintigraphy, has also been used as a tumor-seeking agent; previous clinical studies have demonstrated that 99mTc-tetrofosmin clears rapidly from the lungs and the liver, thereby permitting early high-quality images of the chest (14). Published data indicate that 99mTc-tetrofosmin clearance from the lungs and the liver appears to be faster than the 99mTc-sestamibi clearance (14,15). 99mTc-Tetrofosmin accumulates in different kinds of neoplasms (16) and proved useful in imaging lung cancer (17,18).
The aim of this prospective study was to evaluate the usefulness of 99mTc-tetrofosmin imaging in the presurgical assessment of mediastinal lymph nodes in patients with NSCLC and to compare scintigraphic data with CT results.
MATERIALS AND METHODS
Eighty-three patients (48 men, 35 women; age range, 38–81 y) with primary NSCLC were prospectively studied with chest CT and 99mTc-tetrofosmin SPECT for lymph node mediastinal staging.
All the patients had been selected on the basis of the presence of clinical signs and radiographic or CT signs suggestive of lung cancer and with a definitive diagnosis of NSCLC ascertained from specimens obtained by percutaneous guided CT or bronchoscopy biopsy. In all cases, distant metastases had also been ruled out by CT and bone scintigraphy. The patients’ demographic and clinicopathologic characteristics are summarized in Table 1.
Demographic and Clinicopathologic Characteristics of Study Population
Both chest CT and 99mTc-tetrofosmin scintigraphy were performed during the 2 wk before mediastinoscopy or thoracotomy. All patients gave written informed consent before entering the study.
A commercial tetrofosmin preparation (Myoview; Amersham International) was used. The labeling and quality control procedures were performed according to the manufacturer’s instructions. The scintigraphic images were obtained using a rectangular, large-field-of-view, double-head gamma camera (Millennium MG; General Electric Medical Systems, or Helix; Elscint) equipped with low-energy, high-resolution, parallel-hole collimators. After an intravenous injection of 740 MBq of 99mTc-tetrofosmin, SPECT images of the chest were acquired 20 min later over 360° (180° per head) using the following parameters: a 64 × 64 word matrix, a 3° angular step, and 30 s/frame. After prefiltration with a count-optimized Metz filter, images were reconstructed with a ramp filter to produce 2-pixel-thick transaxial slices. Coronal and sagittal views were then obtained.
SPECT images were always preceded by simultaneous acquisition of anteroposterior (600 s) planar lung images starting 10 min after 99mTc-tetrofosmin injection. However, for the present study we have reported only the SPECT results.
Two experienced nuclear medicine physicians evaluated the SPECT scintigrams; they were unaware of the mediastinal CT findings and, obviously, the final pathologic diagnosis, which was always made after scintigraphy, but they were informed of the clinical reason for the scintigraphy and of the site of the suspect primary lesion. At qualitative analysis, SPECT images were classified as positive for lymph node mediastinal involvement when there were 1 or more foci of well-defined increased 99mTc-tetrofosmin uptake in the mediastinum compared with background activity; disagreements were resolved by consensus, with a third observer as referee.
Chest CT was performed after intravenous injection of nonionic iodinated contrast medium with a window for the mediastinum and a window for the lung parenchyma and evaluated by experienced radiologists. For the interpretation of the CT images, the mediastinal lymph nodes were divided into 2 groups: Those with a diameter of less than 1 cm on the shortest axis were considered normal in size and those with a diameter of 1 cm or more were considered enlarged.
All patients underwent surgical evaluation by means of mediastinoscopy with mediastinal lymph node sampling (14 patients) or thoracotomy (69 patients); surgical node specimens were examined by histopathology with hematoxylin–eosin staining. The results of SPECT were compared with those of CT and both with the histopathologic findings; per-patient sensitivity, specificity, accuracy, and positive and negative predictive values were then determined for each procedure; accuracy values of CT and SPECT were mutually compared by the McNemar test for correlated proportions.
RESULTS
According to histopathologic results, mediastinal lymph node metastases were present in 35 of the 83 patients (42%): in 19 of 36 (53%) patients with adenocarcinoma, in 12 of 39 (31%) with epidermoid squamous cell carcinoma, and in 4 of 8 (50%) with large cell anaplastic carcinoma.
99mTc-Tetrofosmin SPECT yielded a per-patient sensitivity of 85.7%, a specificity of 89.6%, and an accuracy of 88.0% in detecting mediastinal lymph node metastases, whereas CT showed a sensitivity of 68.6%, a specificity of 75.0%, and an accuracy of 72.3% (Table 2). SPECT accuracy was thus significantly higher than that of CT (P < 0.05). We had no difficulty in localizing the foci of increased 99mTc-tetrofosmin uptake in the different regions of mediastinum; nevertheless, unlike CT, which has a better spatial resolution than SPECT, 99mTc-tetrofosmin imaging could not always determine the exact anatomic location of metastatic lymph nodes.
SPECT and CT Results
CT and SPECT results were further compared on a per-patient basis according to whether CT findings were positive or negative (Table 3). Twenty-three of the 24 patients with true-positive findings at CT also had true-positive findings at 99mTc-tetrofosmin scintigraphy (Fig. 1 illustrates 1 of these concordantly positive patients). Thirty-three of the 36 patients with true-negative findings at CT also had true-negative findings at 99mTc-tetrofosmin SPECT, which had false-positive results in 3 patients; 2 of these latter patients had no specific histologic findings in the dissected lymph nodes, whereas anthracosis was ascertained in the third patient. In 10 of the 12 patients with false-positive results at CT, the disease was correctly staged by 99mTc-tetrofosmin imaging (Fig. 2 shows 1 of these patients in whom only the 99mTc-tetrofosmin SPECT findings were true-negative), whereas 2 patients had false-positive results at both imaging procedures. In 1 of these latter patients, the mediastinal lymph nodes were affected by silicosis, whereas in the remaining patient histology found no specific abnormalities. Finally, in 8 of the 11 patients with false-negative findings at CT, the disease was correctly diagnosed by SPECT. The smallest metastatic lymph node ascertained at scintigraphy had a short-axis diameter of 7 mm.
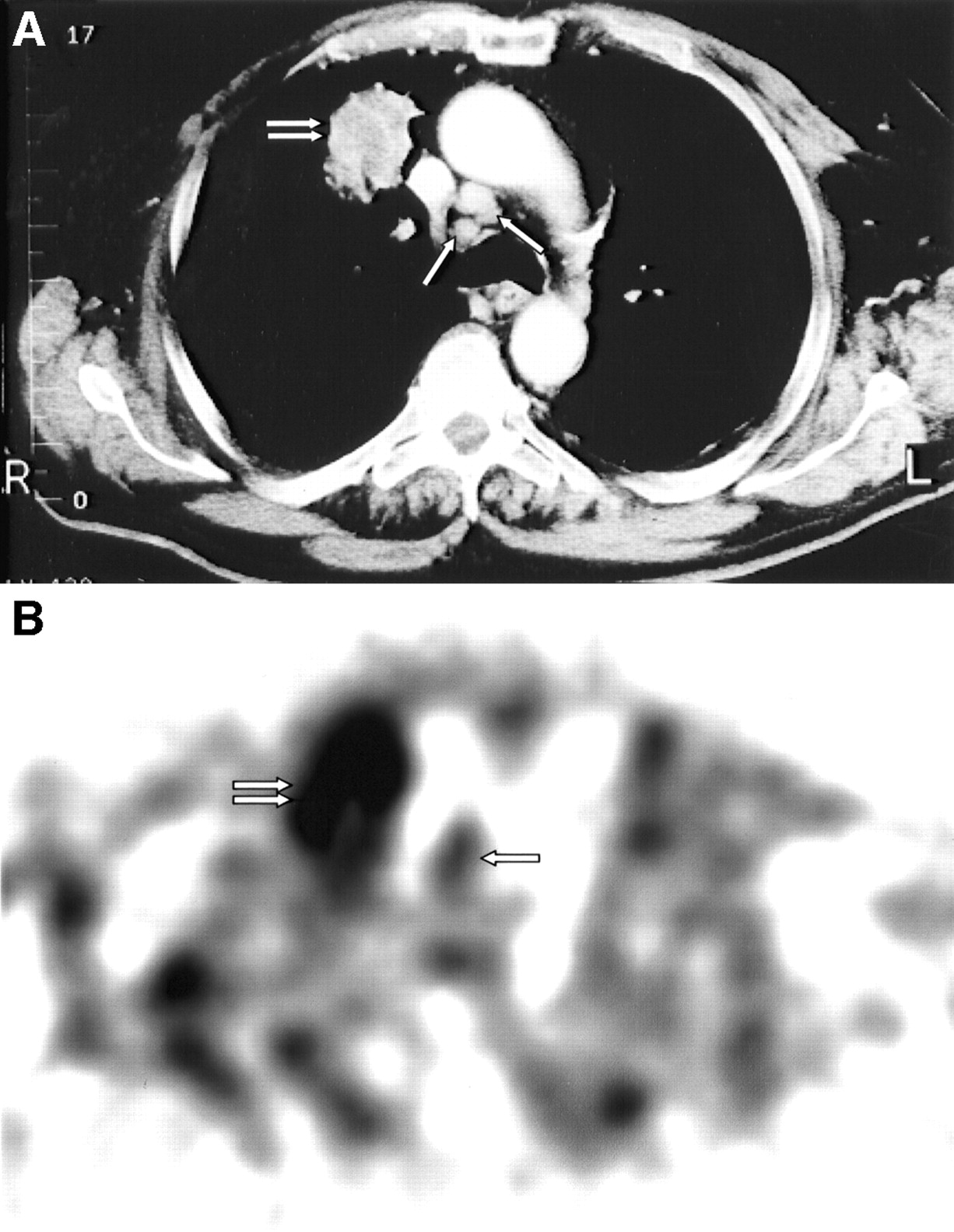
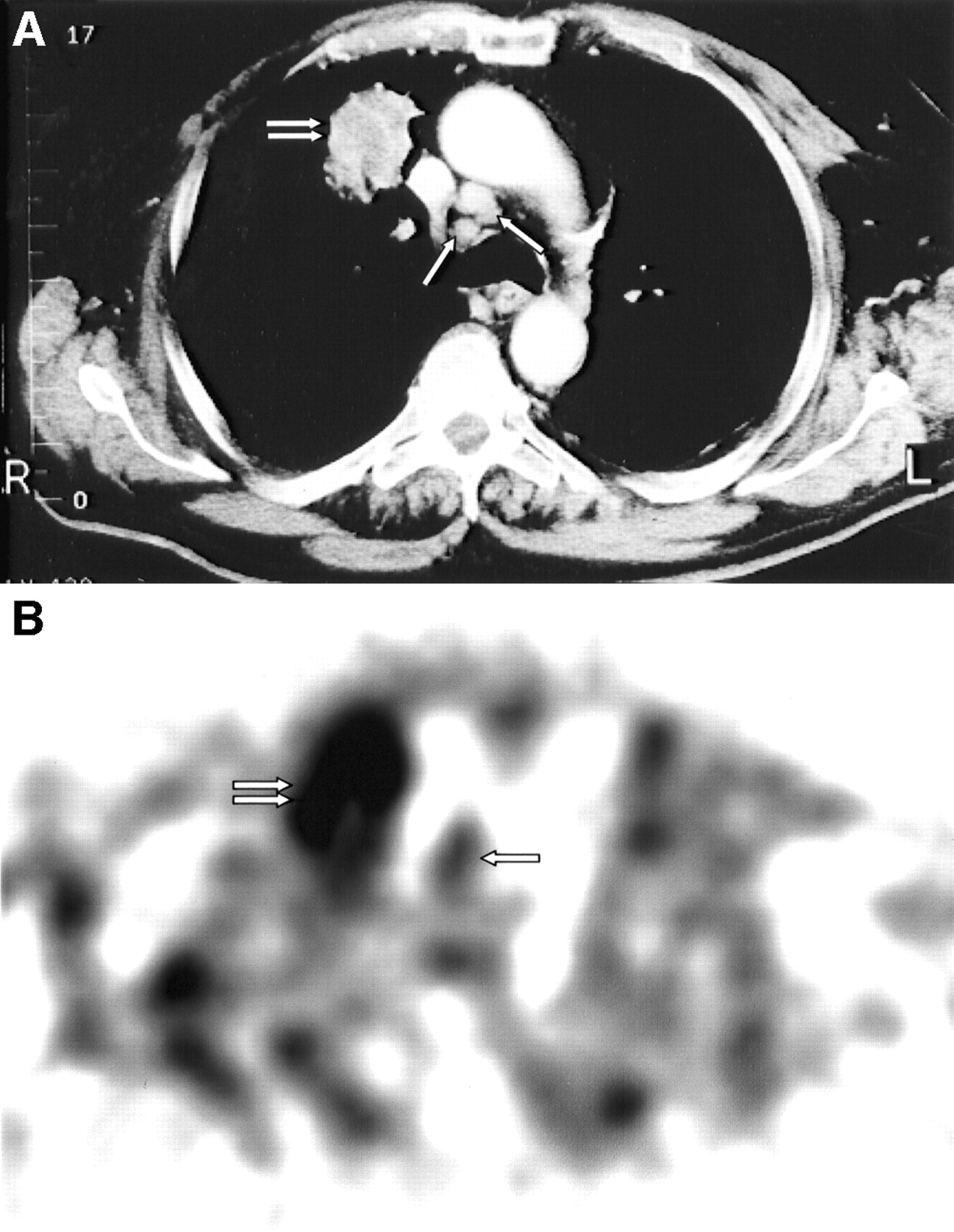
A 77-y-old man with adenocarcinoma of right upper lobe. (A) CT scan shows primary tumor (double arrow) and enlarged paratracheal lymph nodes (single arrows). (B) 99mTc-Tetrofosmin SPECT in transaxial view demonstrates wide area of increased abnormal uptake corresponding to primary tumor (double arrow). Focal area of increased uptake corresponding to paratracheal metastatic lymph nodes (single arrow) was also observed in anterior upper right mediastinum.

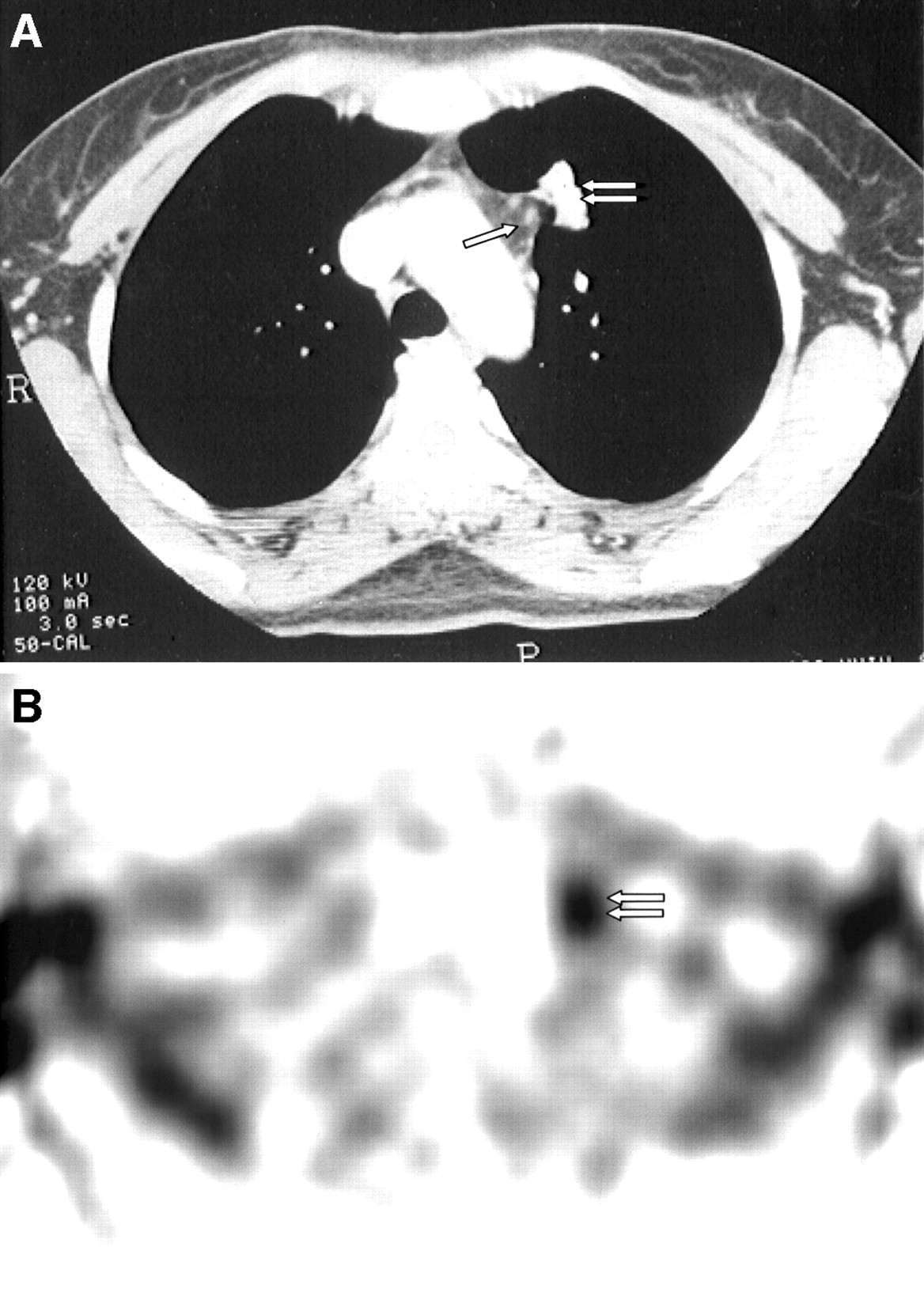
A 45-y-old woman with epidermoid squamous cell carcinoma of left upper lobe. (A) CT scan shows primary tumor (double arrow) and enlarged paraaortic lymph nodes (single arrow). (B) 99mTc-Tetrofosmin SPECT in transaxial view demonstrates area of increased abnormal uptake corresponding to primary tumor (double arrow) but no accumulation in mediastinum. Metastases were excluded at histology in dissected mediastinal nodes positive at CT.
Comparison of CT and SPECT Results on Per-Patient Basis
Thus, 99mTc-tetrofosmin SPECT was able to correctly evaluate the presence or absence of lymph node metastases in 33 of the 36 patients with positive findings at CT (i.e., those with enlarged mediastinal nodes with a short axis of 1 cm or more), with a sensitivity of 95.8% and a global accuracy of 91.7%—the latter result being significantly higher (P < 0.05) for 99mTc-tetrofosmin SPECT than for CT (66.7%). Scintigraphy also proved highly specific (91.7%) in the 47 patients with negative CT findings (normal-sized nodes) but was less sensitive (72.7%) than in the former group, with an accuracy of 87.2%, whereas the CT accuracy was 76.6%. SPECT data were different from CT findings in 22 of the 83 patients studied (i.e., 26.5% of patients), giving correct results in 18 of 22, with 10 downstaged and 8 upstaged.
DISCUSSION
The aim of the preoperative staging of NSCLC is to identify patients who will benefit from surgical treatment so that those who will not can avoid the morbidity and mortality associated with major thoracic surgery (19). In particular, determining mediastinal lymph node involvement is important for determining both tumor resectability and disease prognosis; when mediastinal node metastases are present at the moment of initial diagnosis, the 5-y survival rate after surgery is only 8%, whereas when no lymph node metastases are present, the survival rate approaches 50% (20).
The first step in mediastinal staging in patients with NSCLC involves radiologic imaging with CT; the malignancy criterion is based on lymph node size by measuring the short-axis diameter in the axial images, and a dimension of ≥1 cm is considered suspect for cancer. However, benign nodes may also be enlarged for other reasons, such as reactive hyperplasia, anthracosis, inflammation, or infection; on the other hand, malignant lymph nodes may also be normal in size (7).
Per-patient CT accuracy was 72.3% in our series, and these data are in line with previous results from other studies and with the many prospective data from the Radiologic Diagnostic Oncology Group (21). Moreover, it has been shown that MRI is not superior to CT in mediastinal node staging in NSCLC because of its limited spatial resolution and inability to obtain images during held respiration. These limitations can cause the separate nodes to become blurred on images and to appear as 1 large node (19).
The shortcomings of anatomic images obtained by conventional methods have led clinicians to explore alternative imaging techniques and, in particular, to consider whether functional images may have an additional role in the assessment of mediastinal lymph node involvement in patients with NSCLC. A wide range of radiopharmaceuticals has been used for this purpose, such as 67Ga-citrate, 201Tl-chloride, 99mTc-sestamibi, 111In-pentetreotide, radiolabeled monoclonal antibodies, and, more recently, 18F-FDG (9,22). However, the recommended nuclear medicine imaging procedures with these tracers for mediastinal lymph node detection should be those that are most reliable and easily available; those that are more expensive and unnecessary should be avoided (23).
99mTc-Tetrofosmin is largely used for myocardial perfusion scintigraphy; it accumulates in viable myocardium, and the uptake is proportional to regional blood flow (14). The biodistribution and cellular uptake characteristics of 99mTc-tetrofosmin allow different clinical applications, and its use has also been reported in patients with different tumor types (16). In tumor cell lines, uptake of 99mTc-tetrofosmin depends on both cell membrane and mitochondrial potentials, but only a small fraction of the radiopharmaceutical accumulates inside the mitochondria; the low uptake observed in dead cells indicates that 99mTc-tetrofosmin accumulates in viable tumor tissue (24).
In 2 recent studies performed on a small number of patients with lung cancer, 99mTc-tetrofosmin was used to detect mediastinal lymph node metastases. Shiun et al. (25) reported data on 34 patients with large primary tumors (T2 or greater), in whom 99mTc-tetrofosmin SPECT showed a sensitivity of 85.0%, a specificity of 85.7%, and an accuracy of 85.3%; Buccheri et al. (26), in studying 16 patients with pathologically staged mediastina, found sensitivity, specificity, and accuracy values of 73%, 100%, and 81%, respectively.
Our series was a larger number of patients and demonstrated that 99mTc-tetrofosmin SPECT was superior to CT, which is considered the radiologic procedure of choice for diagnosing mediastinal node metastases from NSCLC. In this comparative study, 99mTc-tetrofosmin imaging resulted in a nonsignificant increase in accuracy in patients with normal-sized lymph nodes at CT, although it is important to emphasize that in 8 of the 11 patients who had mediastinal lymph node metastases but false-negative CT findings, SPECT correctly diagnosed the metastases. However, when SPECT was used to evaluate the mediastinum in the patients for whom CT showed enlarged nodes, a significantly higher accuracy was obtained. This outcome is interesting, since the most important role of a new imaging technique for assessing mediastinal lymph nodes would be to evaluate enlarged nodes and to distinguish tumoral nodes from those with hyperplasia due to nonmalignant conditions, thus reducing the need for invasive staging procedures (8).
Our clinical series proved the usefulness of the noninvasive functional imaging method with the radiopharmaceutical 99mTc-tetrofosmin, uptake of which is related to tumoral cell viability. However, 99mTc-tetrofosmin SPECT presents some diagnostic limitations. In particular, its high accuracy refers only to a per-patient evaluation. Even though the analysis is made with 3-direction sections, 99mTc-tetrofosmin SPECT has a limited spatial resolution, which makes it difficult to define the exact number of involved nodes and thus to calculate the data on a per-node basis. On the other hand, knowledge of the number of mediastinal lymph node metastases is not crucial for NSCLC staging.
We found no difficulty in localizing the foci of increased tetrofosmin uptake in the different regions of the mediastinum; however, the exact anatomic location with respect to the surrounding vascular structures within the mediastinum could not always be estimated. Thus, in this sense, although SPECT imaging is simple to perform, SPECT findings may not always be easily interpreted. Unlike CT, 99mTc-tetrofosmin SPECT lacks anatomic landmarks, potentially leading to an incorrect interpretation of the images because of interference from the great vascular structures. However, in only 3 of the 5 false-positive SPECT results of our series were no specific histologic findings found. It is possible that we erroneously considered some areas of 99mTc-tetrofosmin physiologic uptake as a pathologic accumulation in the mediastinum. However, this interpretation is speculative only when referring to interference from vascular structures, since it is well known that 99mTc-tetrofosmin can also accumulate in lymph nodes with nonspecific changes.
Correlation of images obtained by SPECT and CT and, even more, the combination of image registration and fusion (i.e., precise matching of the data from the 2 imaging modalities) can more accurately identify the tumoral site (27). SPECT/CT fusion has also been used in the application of radiolabeled antibodies in lung cancer, proving useful in evaluating mediastinal adenopathy and especially in distinguishing a normal blood pool from pathologic areas of accumulation (28). We think that the application of SPECT and CT image fusion to 99mTc-tetrofosmin studies, too, could lead to better anatomic localization of areas of abnormal activity at SPECT, thus helping to differentiate tumoral lesion from physiologic radiopharmaceutical uptake; moreover, image fusion is easy to perform using dedicated devices (29,30).
CONCLUSION
The results of this study indicate that 99mTc-tetrofosmin SPECT is a useful noninvasive imaging method for detecting mediastinal lymph node involvement in patients with NSCLC, with a diagnostic accuracy higher than that of CT. If included in preoperative staging, this technique could play a clinical role in reducing the number of invasive procedures such as mediastinoscopy and mediastinotomy in selected patients, particularly in those with enlarged nodes at CT. Fusing SPECT with CT data could improve the interpretation of the scintigraphic images by allowing more exact anatomic localization of metastatic lymph nodes in the mediastinum, thus further increasing 99mTc-tetrofosmin accuracy.
Footnotes
Received Nov. 26, 2002; revision accepted Mar. 28, 2003.
For correspondence or reprints contact: Orazio Schillaci, MD, Viale G. Mazzini 121, 00195 Rome, Italy.
E-mail: oschil{at}tiscalinet.it or orazio.schillaciuniroma2.it




{kind=link}
{kind=link}