


Abstract
Our aim was to evaluate the early effect of local irradiation on normal bone marrow glucose metabolism in rodents, assessed by FDG biodistribution measured by tissue excision and γ counting. Methods: Sixty-one rats were divided into nine groups (n = 4–11 per group). Eight groups of rats received either local irradiation (10 Gy) or sham irradiation to the right femur on day 0. Irradiation was performed using a 60Co γ-ray unit under anesthesia. Each group of rats was fasted overnight and then injected with 5.5–7.4 MBq FDG on day 1, 9, 18, or 30 after the local or sham irradiation. A control group of rats that received neither local nor sham irradiation was studied with FDG on day 0. 18F activity in tissue 1 h after injection was measured using a γ counter. Smear specimens of bone marrow from bilateral femurs were examined by light microscopy. Results: Tracer uptake was relatively stable in marrow from the sham-irradiated rats. By contrast, FDG uptake of the irradiated marrow on day 1 was significantly higher (mean ± SD, 0.257 ± 0.036 percentage injected dose [ID] per gram of tissue per kilogram of rat weight [%ID/g/kg]) than that of the sham group on day 1 (0.187 ± 0.028 %ID/g/kg) and the control group (0.184 ± 0.009 %ID/g/kg) (P < 0.05). Tracer uptake in the irradiated marrow on day 9 was significantly lower (0.148 ± 0.023 %ID/g/kg) than that of the sham group on day 9 (0.193 ± 0.021 %ID/g/kg) and the control group (P < 0.01). In contrast, the nonirradiated contralateral marrow from irradiated rats showed increased FDG uptake on day 18 (0.274 ± 0.063 %ID/g/kg) that was significantly higher than that of the sham group on day 18 (0.208 ± 0.030 %ID/g/kg) and the control group (0.183 ± 0.018 %ID/g/kg) (P < 0.05). The irradiated marrow smear specimens initially revealed increased percentages of neutrophils on day 1 (45% of 500 nucleoid cells examined per slide) compared with that of the sham group (20%), followed by severely decreased overall cellularity on day 9. Conclusion: In this experimental system, normal marrow uptake of FDG transiently rose, then fell, and ultimately returned to baseline after external beam irradiation. Knowledge of this biphasic early irradiation effect on normal bone marrow may be important when the efficacy of radiation therapy on bone metastasis is evaluated using FDG PET after irradiation.
Bone marrow is a frequent site of metastatic cancers, especially from the breast, lung, and prostate (1). Many imaging modalities have been developed for detection, assessment, and after treatment of bone marrow metastases. PET using FDG has been shown to be a useful modality for staging malignant tumors and for evaluating efficacy of treatment (2,3).Recent reports show the usefulness of FDG PET in detecting bone metastases in patients with breast and lung cancer (4,5).
Normal bone itself has little uptake of FDG, whereas normal hematopoietic bone marrow has moderate to occasionally intense uptake of FDG in humans and in animals (6–8). With the increasing use of FDG PET studies in assessing cancer patients, we have sometimes observed increased FDG uptake in the bone marrow after chemotherapy accompanied by cytokine therapy (9,10). Multidrug chemotherapy itself does not change FDG uptake of bone marrow at least initially (2,10). However, little information exists concerning the effect of irradiation on glucose metabolism using FDG in normal bone marrow in rats or in humans (11–13).
Currently, it is difficult to noninvasively monitor the response of bone marrow metastases to irradiation or chemotherapy by conventional imaging methods. FDG PET can quickly and accurately assess treatment response, but a concern in such applications to bone metastases is that an acute or subacute change in FDG uptake in normal marrow as background could occur and make response assessment more difficult, as is the case with cytokine therapy. In this study, to assess the early effect of local irradiation on the normal bone marrow, we evaluated the changes in FDG uptake in bone marrow and other tissues in locally irradiated healthy rats.
MATERIALS AND METHODS
Animals and Irradiation Procedures
Sixty-one healthy female Sprague-Dawley rats (Harlan Sprague-Dawley, Indianapolis, IN) (weight, 250–300 g; age, >3 mo at the beginning of the study [day 0]) were divided into nine groups (n = 4–11 per group). Eight groups (groups 1–8) of rats were anesthetized by intramuscular injection in their left thigh muscles on day 0 with both ketamine hydrochloride (Fort Dodge Laboratories, Inc., Fort Dodge, IA) and xylazine (Bayer Corp., Shawnee Mission, KS) at concentrations of 45 and 25 mg/kg of body weight, respectively. Four groups of rats (groups 1–4; n = 7–11 per group) were subjected to localized irradiation on day 0 (irradiated groups). Localized irradiation was delivered by a 60Co γ-ray unit (Theratron AECL, Kanata, Ontario, Canada) to the right femurs. The rats were placed on a Plexiglas block (Rohm and Haas, Philadelphia, PA) that was set at a distance of 50 cm from the radiation source. The total dose of the irradiation was 10 Gy per rat, with an output of 137.0 cGy/min using a field size of 6 × 6 cm on the center of the right femur, in which the right thigh and calf muscle were included. The left femur was placed outside of this irradiation field. Dosimetry was performed using an ionization chamber connected to an electrometer system directly traceable to the National Institute of Standards and Technology calibration. The exposure dose of the contralateral left femur located outside of the irradiation field was also examined in 5 rats using a small thermoluminescence dosimeter for each rat. Four groups of rats (groups 5–8; n = 4–8 per group) did not receive irradiation (sham-irradiated groups); all procedures were performed in the same manner as in the irradiated groups with the exception of local irradiation on day 0. The other group of rats (group 0; control group) was studied without irradiation or sham irradiation.
FDG Biodistribution Study
The biodistribution study using FDG was performed in each group on a different study day. The control group (group 0) received FDG on day 0. Irradiated groups (groups 1–4) received FDG on day 1 (20–22 h), day 9 (9 d), day 18 (17 or 18 d), or day 30 (30 or 31 d) after irradiation. Sham-irradiated groups (groups 5–8) received FDG on day 1 (20–22 h), day 9 (9 d), day 18 (14 or 18 d), or day 30 (30 or 31 d) after sham irradiation. Each group of rats was fasted overnight before the FDG study. Each rat was injected intravenously with 5.55–7.40 MBq (150–200 μCi) FDG. One hour after FDG injection, all rats were killed, the normal tissues (liver, kidney, spleen, heart, lung, bilateral calf muscle, bilateral femur bone, bilateral femur bone marrow, and blood) were excised and weighed, and the 18F activity in tissue was determined with a γ counter. To obtain the bone marrow, we gently fractured bilateral femoral bones, examined them visually, and curetted the marrow both for smear specimens and for γ counting. The percentage of decay-corrected 18F activity per gram of tissue was determined and normalized for rat weight (percentage injected dose [ID] per gram per kilogram of rat weight [%ID/g/kg]) (7).
Marrow Specimen Examination
Twenty-six marrow smears from 13 representative rats were prepared for cytologic examination at the time of killing. Two specimens from bilateral femoral marrows (irradiated and nonirradiated or sham-irradiated and nonsham-irradiated) were examined per rat. Nine rats were from the irradiated groups of day 1, 9, or 18 (groups 1–3; 3 rats per group) and 4 rats were from the sham-irradiated group of day 18 (group 7). Slides were air-dried and then were stained with Quick III Hematology Stain (MidAtlantic Biomedical, Inc., Paulsboro, NJ). Masked evaluation of marrow smear specimens was performed by an experienced veterinary clinical pathologist using a light microscope. Bone marrow evaluation was performed as differential counts of at least 500 nucleated cells per slide and examination of the overall cellularity and morphology. The percentage of each cell type relative to the total nucleated cells and the group means, SDs, and myeloid-to-erythroid ratios (M/Es) were calculated. Megakaryocytes were evaluated for cellularity and morphology. Additionally, the percentage of degenerating cells was determined on smears from differential counts of at least 200 cells per slide.
Statistical Analysis
The data are presented as mean ± SD. Comparisons of differences in each organ's FDG uptake among all 5 study-day groups in either irradiated or sham-irradiated groups were performed by the Kruskal-Wallis test. Day-by-day comparisons of differences in the organ FDG uptake between each study-day group were performed by the Mann-Whitney U test (bone marrow, spleen, and lung). P < 0.05 was considered significant.
RESULTS
The thermoluminescence dosimetry examination revealed that the exposure dose on the contralateral left femur during the irradiation procedure to right femur bone was between 0.097 and 0.158 Gy, with the average of 0.114 ± 0.025 Gy. This is in contrast to the 10 Gy delivered to the irradiated side.
FDG Biodistribution
Table 1 shows the results of FDG biodistribution observed in the rats from the irradiated groups (calculated as %ID/g/kg) 1 h after intravenous injection. Two rats from groups 1 and 2 (one rat per group) were excluded because of apparently inappropriate fasting conditions (FDG uptake in heart, >1.0 %ID/g/kg). Higher FDG accumulation was observed in the spleen and bilateral femur bone marrow compared with that in other tissues. Bilateral femur bone, liver, blood, and kidney showed lower and relatively stable FDG accumulation throughout the study period. Table 2 shows the results of FDG biodistribution observed in the rats from the sham-irradiated groups. Comparisons of differences in each organ's FDG uptake across the 5 study days revealed significant differences in the FDG uptake time course of the nonirradiated groups in bilateral femur bones, bone marrow, heart, spleen, and lung compared with those of the irradiated groups.
FDG Biodistribution in Irradiated Groups
FDG Biodistribution in Sham-Irradiated Groups
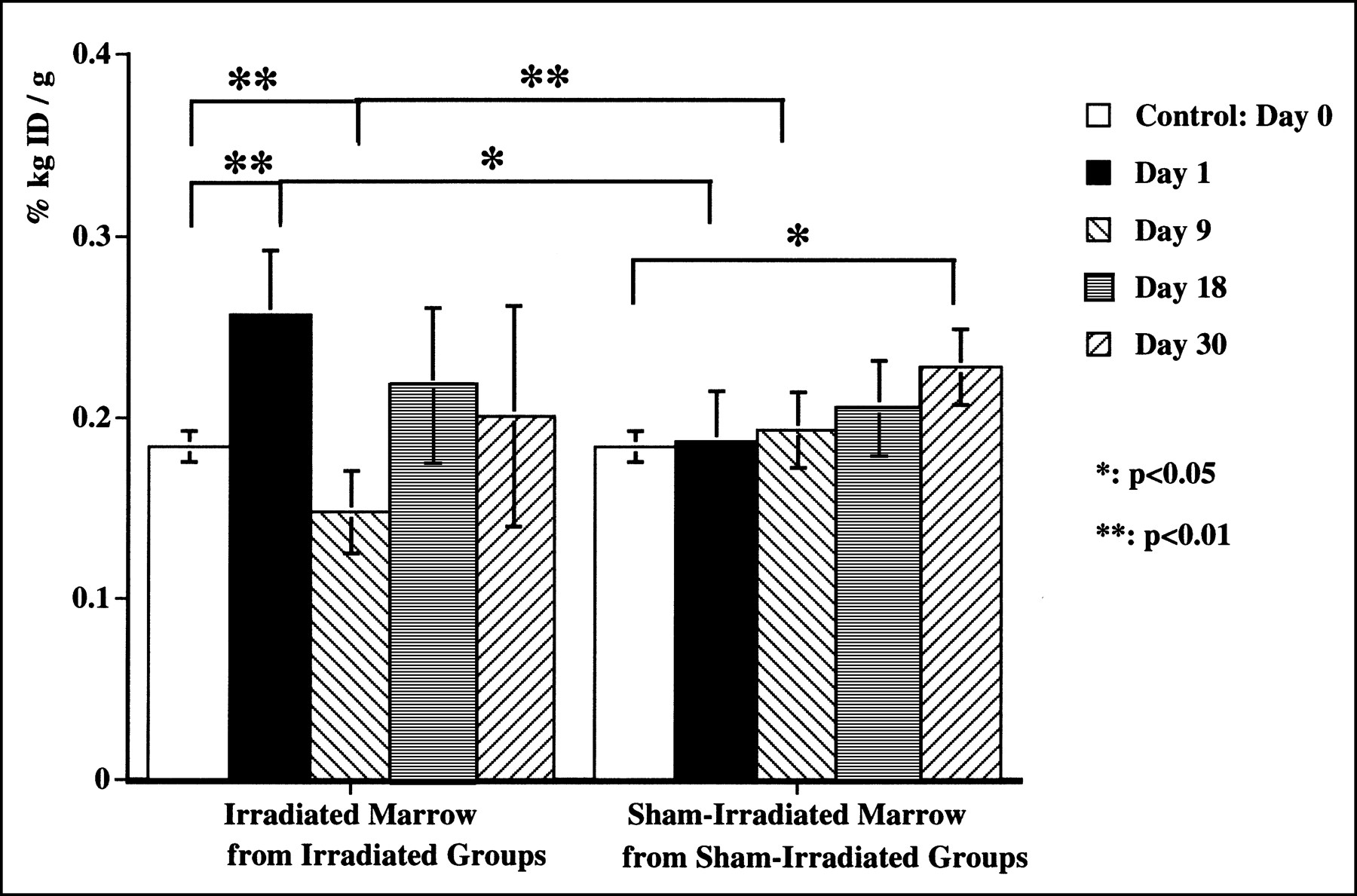
FDG uptake of the right side marrow (irradiated marrow from the irradiated groups and sham-irradiated bone marrow from the sham-irradiated groups) on each study day is shown in Figure 1. FDG uptake of the left side marrow (nonirradiated marrow from the irradiated groups and nonsham-irradiated bone marrow from the sham-irradiated groups) on each study day is shown in Figure 2. FDG uptake in bilateral femur bone marrow from the sham-irradiated groups had the same stable pattern but showed a slow increase over the time course (Fig. 1, right, and Fig. 2, right). FDG uptake of either right or left bone marrow from the sham-irradiated group on day 30 was significantly higher than that of the control group on day 0 (P < 0.05).
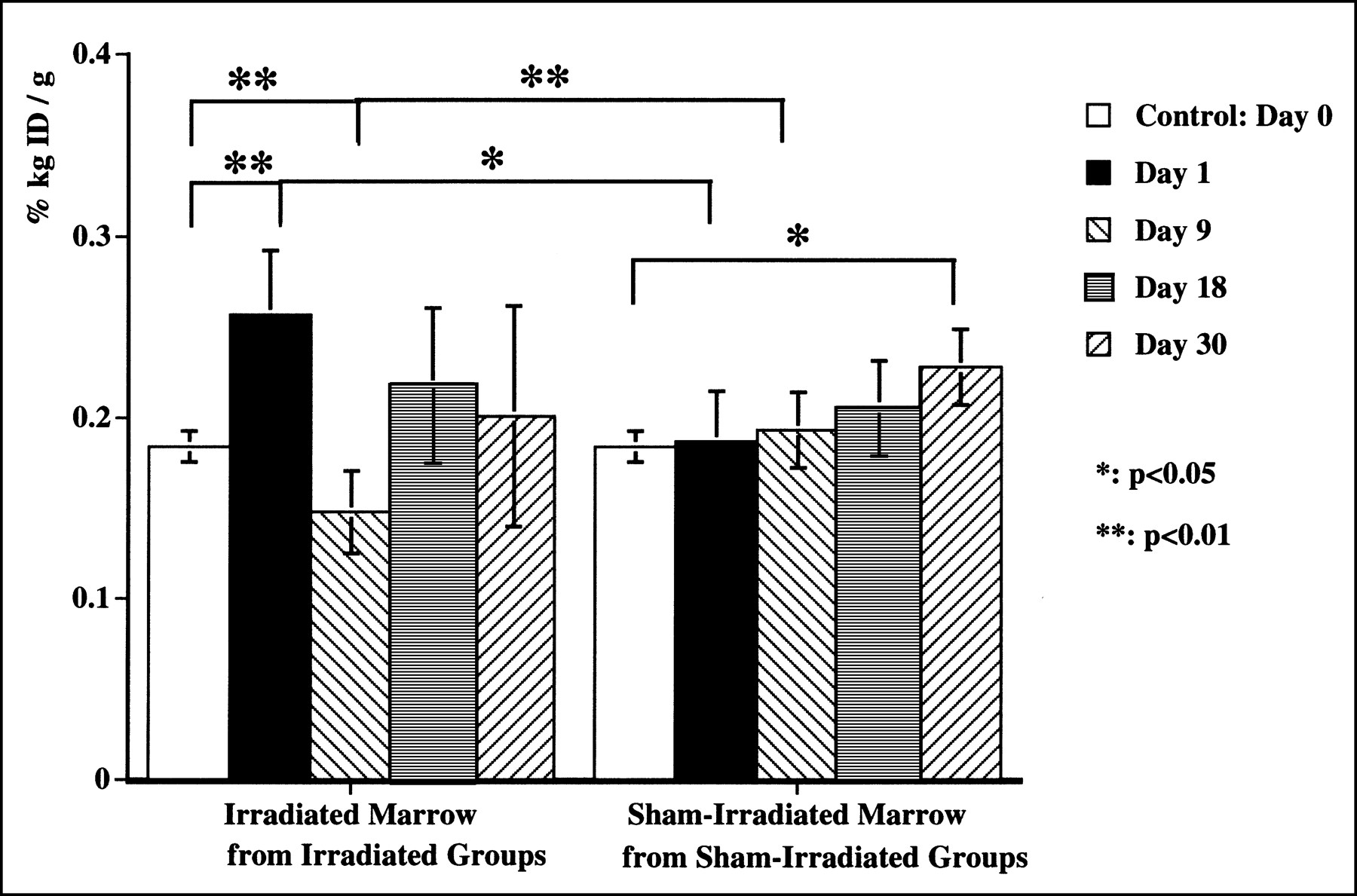
Time course of FDG uptake (%ID/g/kg) in right bone marrow: FDG biodistribution 1 h after injection in irradiated right bone marrow at different time intervals after irradiation compared with that of sham-irradiated marrow. Significant increase in FDG accumulation was observed in irradiated marrow on day 1, which was followed by considerable decrease to below control level on day 9. Uptake increased back to control level on days 18 and 30. Slight increase in FDG uptake over time was observed in sham-irradiated bone marrow.

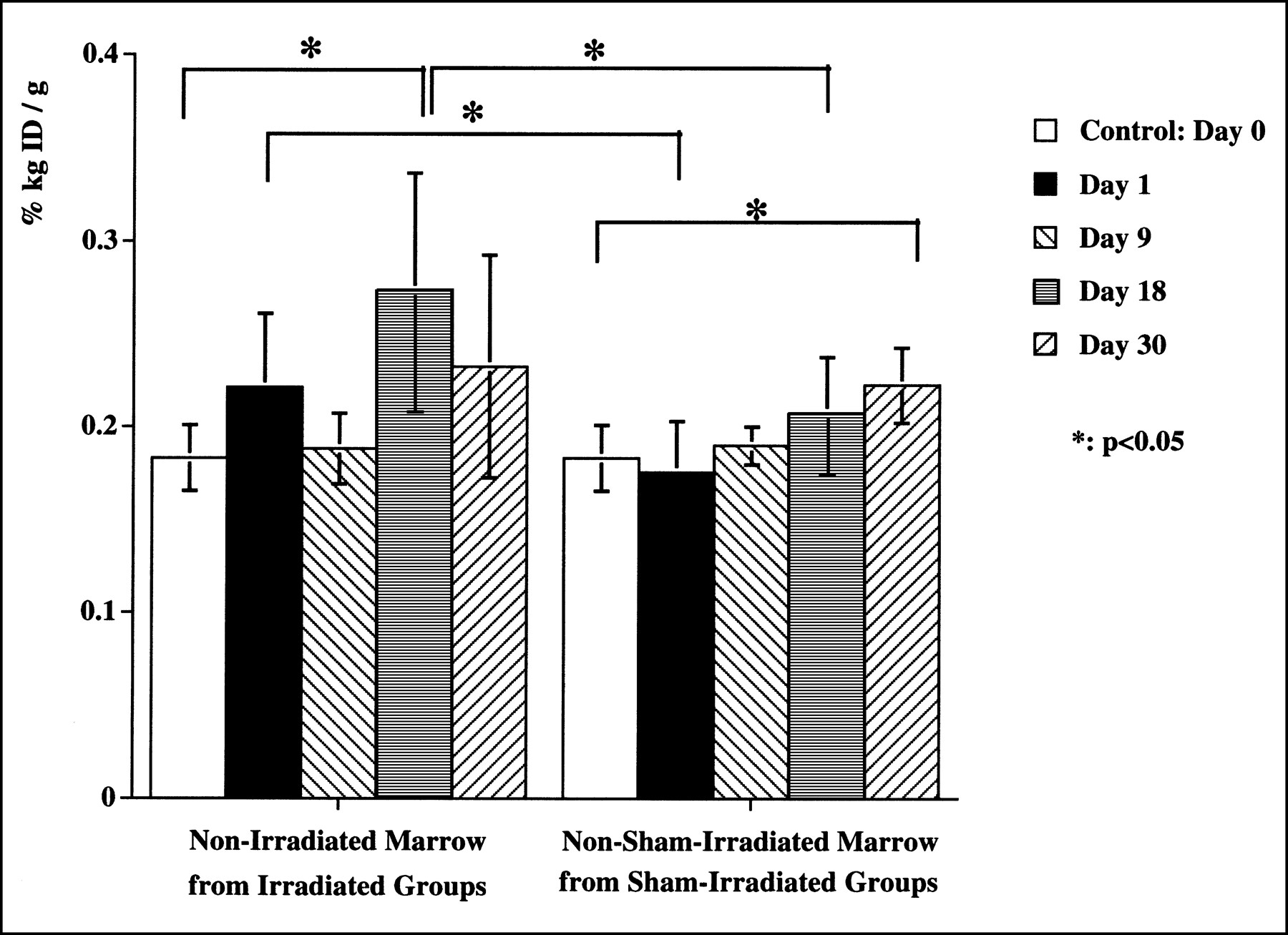
Time course of FDG uptake (%ID/g/kg) in left bone marrow: FDG biodistribution 1 h after injection in nonirradiated left bone marrow from irradiated groups at different time intervals after irradiation compared with that of left marrow from sham-irradiated groups. FDG uptake rose slightly higher than control level on day 1 and decreased on day 9. Then, on day 18, FDG uptake increased substantially above control level. Modest increase in uptake with time was also observed in left bone marrow from sham-irradiated groups.
The irradiated right marrow showed a considerable fluctuation of FDG uptake throughout the time course (Fig. 1, left). FDG uptake in irradiated marrow on day 1 after irradiation was significantly higher (0.257 ± 0.035 %ID/g/kg) than that on day 0 of the control group (0.184 ± 0.009 %ID/g/kg) (P < 0.01) and that on day 1 of the sham group (0.187 ± 0.028 %ID/g/kg) (P < 0.05). FDG uptake on day 9 was significantly lower (0.148 ± 0.023 %ID/g/kg) than that on day 0 of the control group (0.184 ± 0.009 %ID/g/kg) (P < 0.01) and that on day 9 of the sham group (0.193 ± 0.021 %ID/g/kg) (P < 0.01).
On the other hand, marrow of the nonirradiated left side from the irradiated groups showed a different fluctuation of FDG uptake compared with that of the irradiated right side (Fig. 2). FDG uptake of nonirradiated bone marrow from the irradiated group on day 18 increased significantly (0.274 ± 0.063 %ID/g/kg) compared with that on day 0 from the control group (0.183 ± 0.018 %ID/g/kg) (P < 0.05) or that on day 18 from the sham groups (0.208 ± 0.030 %ID/g/kg) (P < 0.05). FDG uptake of nonirradiated bone marrow from the irradiated group on day 1 (0.221 ± 0.040 %ID/g/kg) was significantly higher than that on day 1 from the sham group (0.176 ± 0.028 %ID/g/kg) (P < 0.05) but was not different from that on day 0 of the control group (0.183 ± 0.018 %ID/g/kg) (P = 0.07).
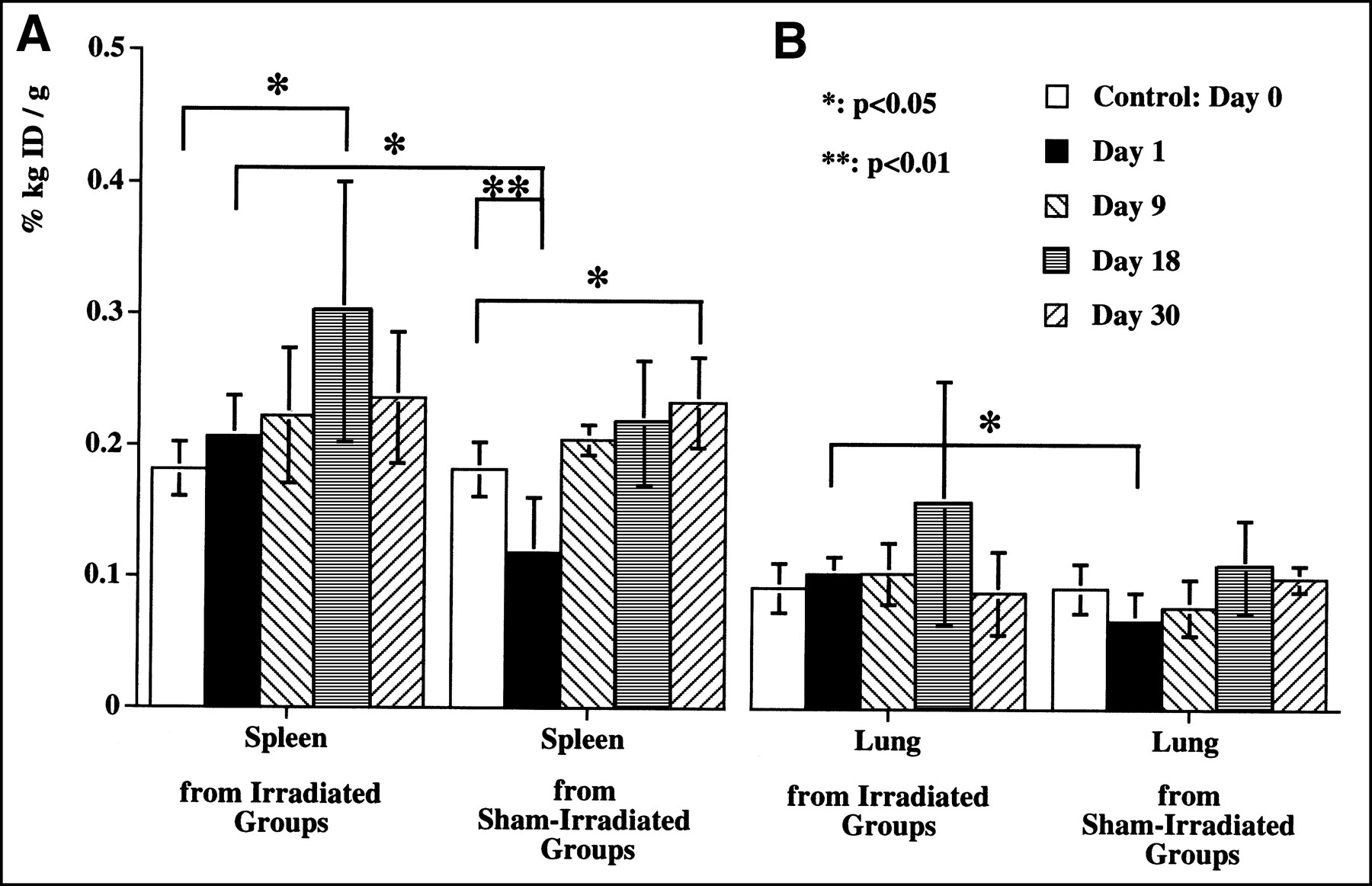
The results of FDG uptake of spleen and lung after local irradiation to the femur are shown in Figure 3. FDG uptake in spleen showed an increase on day 18 (0.303 ± 0.097 %ID/g/kg) compared with that on day 0 (0.181 ± 0.021 %ID/g/kg) (P < 0.05) and that on day 18 from the sham groups (0.218 ± 0.046 %ID/g/kg) (not significant). A similar increase of FDG uptake was found in the lung on day 18 (0.158 ± 0.092 %ID/g/kg) compared with that on day 0 (0.092 ± 0.019 %ID/g/kg) or that on day 18 from the sham groups (0.109 ± 0.035 %ID/g/kg), but the differences were not statistically significant. On day 1, there was a significant decrease of FDG uptake in spleen and lung in the sham group (P < 0.01).
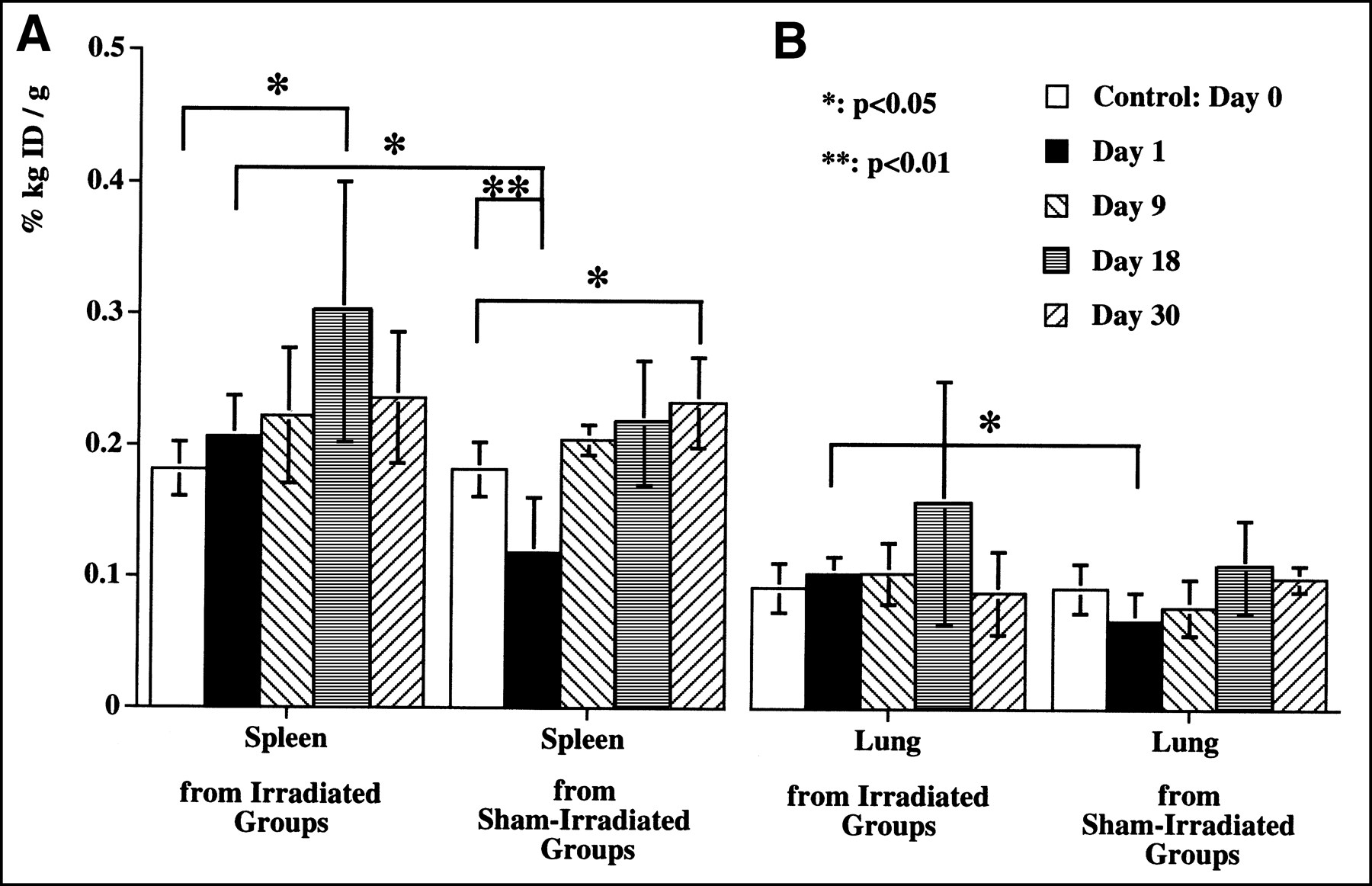
Time course of FDG uptake (%ID/g/kg) in spleen (A) and lung (B): FDG uptake of spleen (left) and lung (right) after local irradiation in irradiated groups compared with those of sham groups. Increased FDG uptake was observed in spleen and in lung on day 18.
Marrow Specimen Evaluation
The appearance of irradiated marrow of group 2 (on day 9) showed liquefaction and hemorrhagic changes at the time of killing. All specimens from the other groups appeared to have the same consistency as normal bone marrow. The cytologic results of the smear specimen from bilateral femur bone marrow from the irradiated groups are summarized in Tables 3 and 4. No cytologic findings were related to apoptosis in this study.
Results of Irradiated Bone Marrow Specimen from Irradiated Groups Compared with Sham-Irradiated Group
Results of Nonirradiated Bone Marrow Specimen from Irradiated Groups Compared with Sham-Irradiated Group
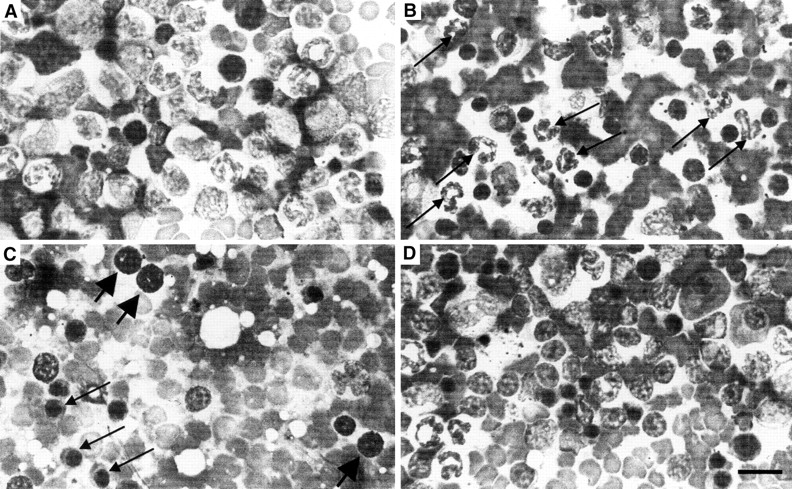
The smears of the irradiated right bone marrow were different from those of the sham group (Table 3 and Fig. 4). The overall marrow cellularity in the smear specimens of the irradiated marrows showed a moderate decrease on day 1 and a severe pancellular loss on day 9 compared with that of the sham group. The overall cellularity in the smear specimens of the irradiated marrow on day 18 was almost the same as that of the sham groups. On day 18, an increased number of adipose cells were observed on the irradiated side. Figure 4 reveals a severe cellular loss of nucleated cells and an increased number of red blood cells on specimens of day 9. The increased numbers in mature red blood cells observed on day 9 may be caused by hemodilution associated with the collapse of the irradiated sinusoids. The percentages of degenerative cells on day 9 increased to 57% in 200 cells counted, whereas those in the other groups were <20%.
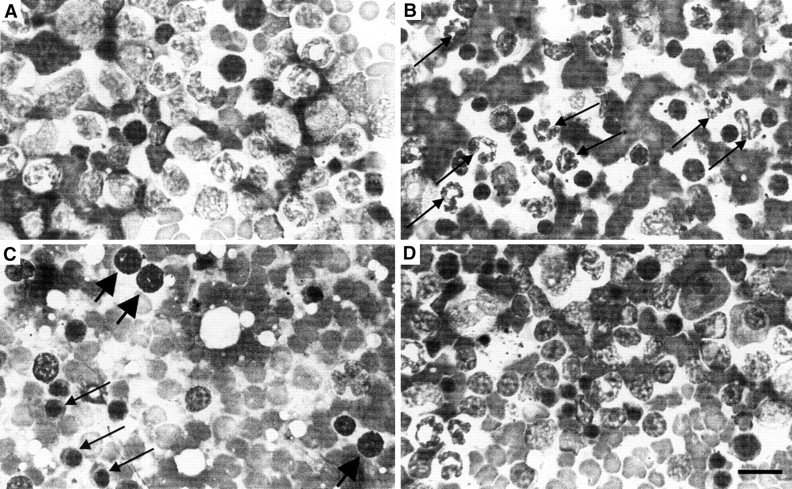
Smear specimens of irradiated and sham-irradiated bone marrow: smear specimens of irradiated right bone marrow on day 1 (B), day 9 (C), and day 18 (D) compared with sham-irradiated marrow on day 18 (A). Overall cellularity decreased moderately on day 1, showed severe cellular loss on day 9, and then increased back to control level on day 18. Fraction of mature neutrophils (long arrows) increased on day 1. On day 9, number of nucleated cells decreased and increased number of mature red blood cells was observed, which suggested collapse of irradiated sinusoids. Increased number of premature erythroid cells (rubricyte [long arrows] or prorubricyte [short arrows]) was also observed. Quick III Hematology Stain (MidAtlantic Biomedical, Inc., Paulsboro, NJ), ×400; bar = 20 μm.
The percentages of total granulocytic cells of the irradiated right bone marrow showed an increase on day 1 (55.6%) and then fell below the control level on days 9 and 18 (6.7% and 17.3%, respectively). The percentages of myeloid mitotic figures on day 1 were lower than that of the sham group and then slightly increased on days 9 and 18. The increased percentages of mature neutrophils (band and segmented) were observed on day 1 (45.4%), then decreased on day 9 (3.7%), and were still relatively low on day 18 (10.5%) compared with that of the sham group (21.8%). A decrease in megakaryocytes was also observed on days 9 and 18.
The percentages of total erythroid cells on the irradiated marrow were decreased on day 1 (4.0%), increased remarkably on day 9 (70.7%), and then returned to the sham group level. The percentages of erythroid mitotic figures also showed a similar fluctuation. The percentages of erythroid mitotic figures on day 9 were 4-fold higher than those of the sham group. The premature erythroid cells (rubriblast, prorubricyte, and rubricyte), except for metarubricyte, showed the highest percentages on day 9.
The smear results from nonirradiated left bone marrow from the irradiated rats did not show any significant changes compared with the sham group (Table 4). The M/E, percentages of degenerative cells, overall cellularity, and cellularity of megakaryocytes were stable from day 1 to day 18. On day 9, the percentages of total granulocytic cells and total erythrocytic cells increased slightly, but without any change in the M/E. The percentages of myeloid and erythroid mitotic figures were also the highest on day 9.
DISCUSSION
The preoperative assessment of patients considered for surgery of lung or breast cancer sometimes results in the detection of unresectable tumor with bone metastases (1). At the time of initial diagnosis, up to 45% of breast cancer patients with lymph node involvement exhibit microscopic bone marrow metastases (14). Bone scintigraphy is widely used for assessing the involvement of bone metastasis but has a poor specificity. FDG PET has been shown to be a useful modality in staging malignant tumors with high sensitivity and high specificity (4,5). PET has also been shown to be a promising tool in assessing treatment response to chemotherapy and radiotherapy (2,15). An increasing use of FDG PET in evaluation of the treatment effect of irradiation on bone metastases of tumors may be expected in the future.
Our results in this experimental system showed that localized irradiation of normal bone marrow with a single dose of 10 Gy caused considerable changes in FDG uptake in the early follow-up period of both irradiated and nonirradiated contralateral marrow. Irradiated marrow had a transient rise of FDG uptake, followed by a decline, and then normalization. Nonirradiated marrow from irradiated animals had a transient rise in FDG uptake. Knowledge of this phenomenon may be important for FDG PET diagnosis because this kind of radiation-induced fluctuation could make FDG PET diagnosis difficult or confusing (or both) in evaluation of the treatment effect if it were performed as an early follow-up after irradiation. FDG uptake of nonirradiated marrow should not be misinterpreted as bone marrow metastasis. In addition, the significant rise in FDG uptake observed in the nonirradiated marrow indicates that it may be inadequate to use an irradiated-to-nonirradiated marrow uptake ratio for the purpose of the evaluation of treatment effect on metastatic bone lesions. Although we have no evidence on how long the fluctuation of FDG uptake in bone marrow will last, evaluation of the treatment response of irradiated bone marrow metastases with FDG PET should be interpreted with caution within 30 d after irradiation. Ultimately, careful sequential FDG PET evaluation of human marrow at various time points after irradiation will be needed to determine the significance of these preclinical findings.
Our results are, on first inspection, seemingly at variance with a previous study that evaluated FDG uptake in irradiated bone marrow and other tissues in rodents (11). In that study, FDG uptake in bone and bone marrow did not show a significant change after several doses of irradiation. However, we believe that this variance results from a different experimental design, in which bone and bone marrow were examined together only at 6 d after irradiation compared with our multiple sequential assessment of bone and bone marrow after irradiation.
As for the irradiation effect on FDG uptake in tumor, multiple studies have shown that FDG accumulation in irradiated tumor cells or tumor tissue is determined as a result of the trade-off of several positive and negative factors. Some clinical and experimental studies have shown a reduction in FDG uptake in tumor tissue and cells after irradiation (11,16,17), whereas other in vivo and in vitro studies revealed transiently increased FDG uptake in the early phase after irradiation (18,19). Higashi et al. (18,20) reported a substantial increase in the overall tracer uptake with an increased uptake per cancer cell after irradiation, in spite of a decrease in viable cell number in vitro. Fujibayashi et al. (19) showed a transient increase in glucose transporter-1 messenger RNA expression and the enzymatic activity of hexokinase in cultured tumor cells within a few hours after exposure to ionizing radiation. In their study, a single radiation exposure with 10 Gy did not change the number of tumor cells until 4 d, although it increased the deoxyglucose uptake within a few hours. Furthermore, inflammatory reactions with high metabolic activity have also been reported to have some influence on the FDG accumulation in irradiated tumor tissue (21). Our findings suggest that similar phenomena can occur in normal bone marrow after irradiation.
Sequential histopathologic changes, acute and subacute, are typically observed in irradiated normal bone and bone marrow (22–24). This damage is summarized as follows: (a) decreased marrow cellularity, (b) extravasation of erythrocytes and increased blood pool, (c) dilatation or collapse of the marrow sinusoids, (d) increased bone marrow blood flow, (e) increased vascular permeability, (f) migration of premature progenitor cells from outside and their proliferation, and (g) infiltration of inflammatory cells. Aspects of a–c and f and g were clearly observed in this study. As for the relationship between FDG accumulation and the histologic changes, a decrease in marrow cellularity would be expected to result in decreased FDG accumulation (20), whereas infiltration of inflammatory cells would be expected to result in increased FDG accumulation (21).
Although total cell counting of the entire bone marrow was not performed in this study, the results of overall cellularity in our smear specimen indicate a severe total cell loss in the irradiated marrow by day 9. This finding is generally in agreement with the previous studies in rodents and humans, in which the cellularity of total bone marrow in irradiated marrow reached a nadir between 4 and 10 d after single local irradiation of various doses (25,26). The 10-Gy dose, which was used as a single irradiation in this study, is also known as a myeloablative dose in many species (27,28). From the cytology and the literature, we assume that most irradiated progenitor cells were still morphologically alive on day 1 but were on the course to cell death and that most of the irradiated cells were already dead on day 9. However, migration of progenitor cells from outside the irradiated field has been observed within 3 h and continues until around 3 wk after local irradiation (25,28). Therefore, the fluctuation of overall cellularity observed in the irradiated marrow in this study is believed to be the combined result of the decreasing number of irradiated cells and the increasing number of migrating progenitor cells and infiltrating inflammatory cells.
Second, infiltration of inflammatory cells should be considered. The changes in the percentages of neutrophils in this study are in agreement with the results of previous studies (29,30). These reports showed that infiltration of inflammatory cells was observed in irradiated regions within 8 h after irradiation and had disappeared from there within 2–10 d. An increased uptake of 111In-labeled leukocytes has also been observed in the irradiated bone marrow 1 d after irradiation (31). We believe that most neutrophils observed in the irradiated marrow were activated infiltrating cells from outside of the irradiation field. In this study, although the overall cellularity was moderately lower on day 1, the percentage of mature neutrophils observed in the irradiated marrow was 45% of total marrow cells on day 1, at least 2-fold higher than that of the sham group. In addition, the main energy production pathway in neutrophils is glycolysis (32). FDG is likely to accumulate in the region with increased glycolysis. Thus, we conclude that the overall FDG uptake of activated neutrophils in the irradiated bone marrow on day 1 was much higher than that of nonactivated neutrophils on day 0.
In this study, the proliferative activity of bone marrow cells after irradiation had little apparent relationship with FDG uptake observed in the irradiated marrow. The increased percentages in granulocytic cells on day 1 are caused by the profound loss of erythroid cells, not the proliferation of granulocytic cells. The increased percentages of the myeloid mitotic figures on day 18 suggest that the recovery of granulocytic cells was active around 18 d after irradiation. The evaluation of megakaryocytes also showed a change over time that was similar to that seen with the granulocytic cells. In contrast, the increased percentages in total erythroid cells on day 9 may be associated with both the profound loss of granulocytic cells and the increased proliferation of erythroid cells. The highest percentages of the mitotic figures and the premature cells observed on day 9 suggest that the proliferation and regeneration of erythroid cells had started between 1 and 9 d after irradiation. The timing is compatible with each of their transit times in bone marrow, as 1 wk for erythroid cells and 10–14 d for granulocytic and megakaryocytic cells (33). These findings indicate that the proliferation of bone marrow cells increased around day 9 through day 18; however, no increase in FDG uptake was observed in the irradiated marrow on day 9 and day 18. Our results are compatible with the findings of a previous in vitro study using cancer cells: FDG uptake does not strongly relate to the proliferative activity but is more closely related to the number of viable tumor cells (20).
Table 5 summarizes the relationship between FDG uptake and cytologic change in the irradiated and nonirradiated bone marrow. The increased FDG uptake observed on day 1 in the irradiated marrow may be explained by the trade-off between the infiltration of neutrophils and the relatively decreased cellularity. The decreased FDG uptake on day 9 is easily explained by the overall cellular loss. However, the increased FDG uptake observed on day 18 in the nonirradiated marrow cannot be explained by the results of the smear specimen.
Correlation Between FDG Uptake and Cytologic Change in Bilateral Bone Marrow from Irradiated Groups
Concerning the nonirradiated contralateral bone marrow, the smear specimen results in this study did not show any significant change compared with the sham group throughout the time course. However, subtle histologic changes, which could not be detected in our evaluation, are likely to be responsible for the mild changes in FDG uptake in the marrow over time. Our cytologic results are at variance with some of the previous studies, in which overall cellularity in shielded bone marrow also showed a smaller, but similar, fluctuation after irradiation to the irradiated marrow (26,34). This phenomenon is caused, in part, by the migration of hematopoietic cells from nonirradiated area to irradiated marrow (34). Therefore, the magnitude of this fluctuation of overall cellularity in nonirradiated bone marrow appears to depend on the irradiation dose and the irradiated area. In our experimental system, the change in overall cellularity in nonirradiated marrow appeared to be too subtle to be observed by visual examination of the smear specimen.
Figure 3 showed similar increased FDG uptake on day 18 in the spleen and lung in the irradiated groups, which may also help in understanding the mild changes in FDG uptake in the nonirradiated marrow from the irradiated rats. Both organs are monocyte/macrophage-rich tissues as is bone marrow itself. This phenomenon could be explained by systemic interactions between several cytokines, such as interleukin-1, interleukin-3, interleukin-6, tumor necrosis factor, granulocyte/macrophage colony-stimulating factor (GM-CSF), and granulocyte colony-stimulating factor (G-CSF). These interactions occur after irradiation and reportedly stimulate metabolism and cellularity of bone marrow and circulation or cycling of myeloid progenitor cells (35,36). In our previous study of normal rats and human breast cancer patients treated with chemotherapy, FDG uptake in bone marrow and spleen increased strikingly during G-CSF and GM-CSF therapy and then decreased to the control level after cessation of the therapy (10,37). Even if no significant cytologic change occurs, endogenous CSFs released by systemic interactions after irradiation stimulate the metabolism of each marrow cell, which may result in increased FDG uptake in the nonirradiated marrow. The increased uptake observed on day 18 in the spleen and lung may also be explained by the effect of CSF released either by the irradiated bone marrow or by each of the individual macrophage-rich tissues. Thus, local irradiation not only affects glucose metabolism of the irradiated bone marrow but also has systemic effects on the metabolism of the nonirradiated tissue, such as contralateral marrow, spleen, or lung.
It is likely, however, that the results of a trade-off may change net marrow uptake upward or downward depending on the dose and methods of irradiation. Fractionation or hyperfractionation methods of irradiation generally tend to spare normal tissues because of repair from irradiation damage between dose fractions. Further study is needed to determine the effects of fractionated radiation on normal marrow.
CONCLUSION
In this experimental rodent model, normal bone marrow FDG uptake transiently rises, then falls, and then returns to baseline after external beam irradiation. Knowledge of this early biphasic radiation effect on normal bone marrow FDG uptake may be important for accurately assessing the efficacy of radiation therapy on bone metastasis using FDG PET after irradiation. Sequential studies in patients soon after radiation therapy appear to be warranted to clinically verify these preclinical observations.
Acknowledgments
The authors thank Mary A. Davis (Radiation Oncology, University of Michigan, Ann Arbor, MI) for technical assistance with the rat irradiation procedure and Suzanne M. Carlson (University of Michigan) for her valuable editorial assistance. The authors also thank the members of Dr. Wahl's laboratory and the staff members of the PET center (University of Michigan). This study was supported by National Institutes of Health grants CA52880 and 2P30 CA46592.
Footnotes
Received Nov. 10, 1999; revision accepted Mar. 28, 2000.
For correspondence or reprints contact: Richard L. Wahl, MD, Division of Nuclear Medicine, University of Michigan Medical Center, 1500 E. Medical Center Dr., B1G 412, Box 0028, Ann Arbor, MI 48109-0028.
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Application of Intravenous Contrast in PET/CT: Does It Really Introduce Significant Attenuation Correction Error?
- Diagnosing Infection in the Failed Joint Replacement: A Comparison of Coincidence Detection 18F-FDG and 111In-Labeled Leukocyte/99mTc-Sulfur Colloid Marrow Imaging
- Local and Distant Effects of Radiotherapy on FDG Accumulation in Bone Marrow