


Abstract
Langerhans' cell histiocytosis is a granulomatous disease that may involve multiple organs and the prognosis of which is highly variable. Because the prognosis depends particularly on the number of tissues involved, the accurate identification of the organs involved by granulomatous lesions is of critical importance. We hypothesized that 111In-pentetreotide scintigraphy would be useful for evaluation of patients with Langerhans' cells histiocytosis. Methods: Thirteen patients (38.3 ± 10.4 y) with Langerhans' cell histiocytosis (8 patients with unifocal lung disease, 5 with multifocal disease) received intravenous 111In-pentetreotide (111–222 MBq), and planar images were obtained at 24 h after injection. Pulmonary uptake was quantified using a lung-to-background ratio (L/B) and compared with a population of 10 normal scintigrams. For the other sites, uptake of radioactivity in disease-related areas was visually assessed. Results: Ten of 12 patients with lung involvement had increased lung uptake (L/B, 2.23 ± 0.49 versus 1.34 ± 0.07; P < 0.001). In the patients with multifocal disease, increased 111In-pentetreotide uptake was found in disease-related areas such as the salivary glands, the skin, the soft tissues, and the bones. However, somatostatin receptor imaging was insensitive for detecting central nervous system and liver involvement and most skin lesions. Conclusion: 111In-pentetreotide imaging may be useful in Langerhans' cell histiocytosis. Further study will indicate whether 111In-pentetreotide is a relevant tracer in the management of histiocytosis.
Langerhans' cell histiocytosis, also called histiocytosis X, denotes a group of rare diseases of unknown origin characterized by the presence of destructive granulomas containing large numbers of Langerhans' cells. The disease may involve multiple tissues or remain localized to a single organ, especially lung and bone (1,2). A wide spectrum of clinical manifestations may be encountered, and syndromes such as Hand-Schüller-Christian disease, Letterer-Siwe disease, and eosinophilic granuloma were classically included in this spectrum. However, distinction between these syndromes may be difficult, with each disease exhibiting its own clinical characteristics. Langerhans' cell histiocytosis is now categorized into unifocal disease (single organ involvement) and multifocal disease (3,4).
The prognosis of patients with Langerhans' cell histiocytosis may vary greatly, from patients healing spontaneously or after treatment to patients with disabling disease and fatal evolution. It is often difficult to predict at initial clinical presentation which patient will have a benign or poor course, but, because the prognosis depends particularly on the number of tissues involved, accurate identification of the organs involved by granulomatous lesions is of critical importance. Standard radiography and CT are used routinely for this purpose. However, these techniques do not assess the clinical course of the disease and some involved organs may not be detected, although involvement is clinically patent. In patients with bone involvement, bone scintigraphy has been shown to be complementary to conventional radiography (5,6).
Visualization of granuloma sites with 111In-pentetreotide (Octreoscan; Mallinckrodt, Petten, The Netherlands), a radiolabeled somatostatin analog, has been reported in patients with granulomatous disease, such as sarcoidosis, tuberculosis, and Wegener's granulomatosis (7,8). Recently, the presence of somatostatin was revealed in Langerhans' cells of the normal human epidermis (9). We hypothesized that somatostatin receptor scintigraphy could be useful for the visualization of lesions in patients with Langerhans' cell histiocytosis. We present the scintigraphic results of a preliminary study of 13 consecutive patients.
MATERIALS AND METHODS
Patients
Thirteen consecutive patients (8 men, 5 women; mean age, 38.3 ± 10.4 y; age range, 27–61 y) were prospectively studied after giving their informed consent. Eight patients presented with unifocal lung disease, and 5 patients had multifocal disease. The patients' clinical characteristics at the time of scintigraphy are given in Table 1.
Clinical Features of Patients with Langerhans' Cell Histiocytosis
Patients with Unifocal Lung Disease.
On the basis of CT results, 4 patients had cystic lesions only, whereas the other 4 had a combination of nodules and cysts. Histologic confirmation of Langerhans' cell histiocytosis was obtained in 6 patients, whereas in 2 others, the diagnosis was based on typical chest CT abnormalities (10). Three patients (patients 3, 8, and 11) were on a waiting list for lung transplantation.
Patients with Multifocal Disease.
All 5 patients had histologic confirmation of Langerhans' cell histiocytosis. The following organs were involved: lungs (4 patients, all with cystic lesions on CT); bones (2 patients with cystic lesions on radiography involving the proximal humerus [patient 1] and the distal femur [patient 13]); central nervous system (1 patient with clinically patent cerebellar involvement but with faint abnormalities on CT; 1 patient with clinically patent diabetes insipidus and brain-stem involvement, with moderate abnormalities in the brain stem on MRI; 2 patients with clinically patent diabetes insipidus but with no abnormality on CT or MRI); skin (2 patients [patients 3 and 10] with biopsy-proven lesions involving the same areas: head, axilla, and upper torso [patient 3 also had a biopsy-proven lesion on the left ear]); salivary glands (2 patients with clinically patent involvement but with no biopsy confirmation); and liver (1 patient with biopsy confirmation).
Patient 1 had stiffening of the soft tissues surrounding the shoulders, hips, and knees with diminution of mobility of the main joints. Biopsy of the soft tissues was not obtained.
Somatostatin Receptor Imaging
111In-pentetreotide (111–222 MBq) was injected intravenously. Planar images were acquired on a dual-head gamma camera (DST-XL; Sopha Medical Vision International, Buc, France) equipped with a medium-energy collimator. Static images were obtained 24 h after injection of 111In-pentetreotide. Preset counts were 300,000 for the head and neck and 500,000 for the other views. Chest tomographic imaging was performed on 7 patients, and brain tomographic imaging was performed on patient 10 (the other patients were unable to be held in 1 position for >30 min). Sixty-four projections were acquired for 60 s each over a 360° orbit, and the projection datasets were prefiltered with a Hanning filter. Images were interpreted by 2 observers who were unaware of the clinical presentation.
Lung uptake was visually assessed and quantified by the lung-to-background ratio (L/B). Briefly, regions of interest were manually drawn over the 2 lungs on the anterior planar image and on a normal region considered as the background (generally, the ipsilateral shoulder).
The average counts per pixel in each region of interest were computed, the L/B was generated for each lung, and the lung uptake was expressed as the mean L/B. This information was compared with that of a population of 10 control patients with neuroendocrine tumors without lung involvement.
For the other sites, tracer uptake in disease-related areas was graded on a 4-level scale: 0, no uptake; +, faint uptake; ++, moderate uptake; and +++, intense uptake.
Statistical Analysis
L/Bs are expressed as mean ± SD. The unpaired Student t test was used when the patients with increased lung uptake were compared with the control group. P < 0.05 is considered significant.
RESULTS
The patient data are reported in Table 2.
Results of 111In-Pentetreotide Scintigraphy in Patients with Langerhans' Cell Histiocytosis
Lungs
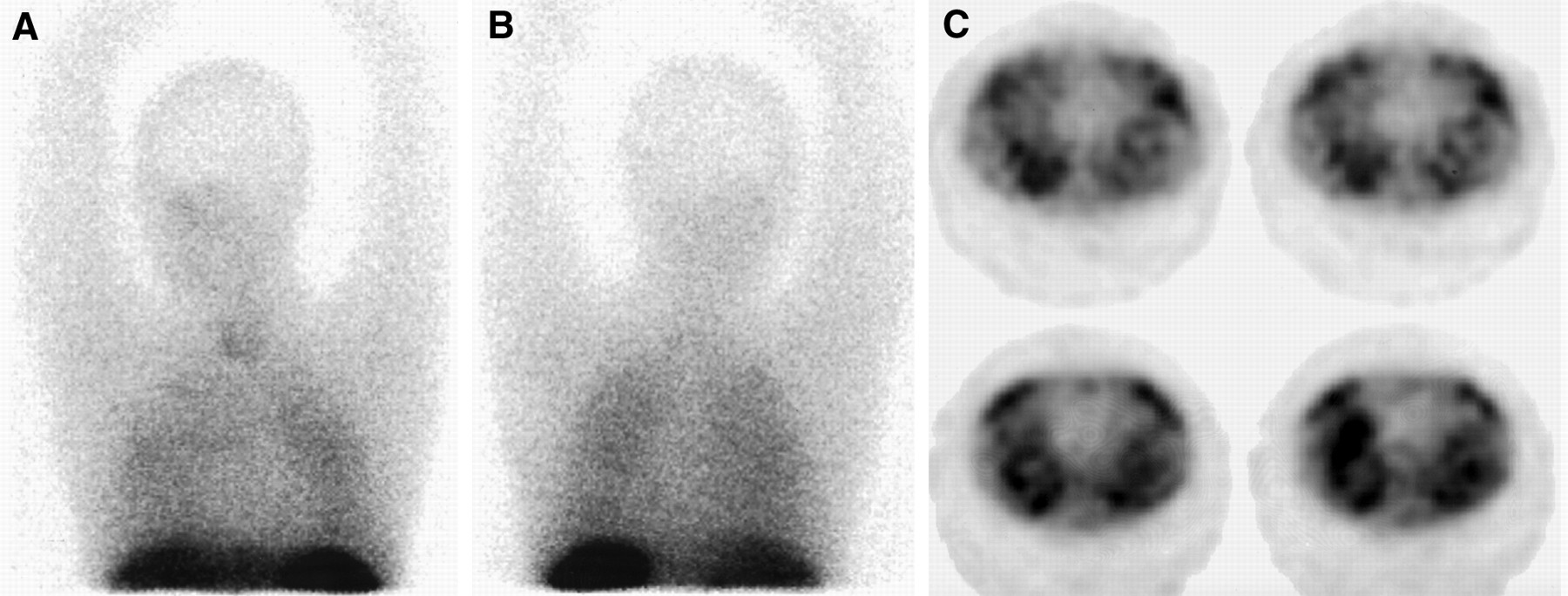
Lung uptake was increased bilaterally and diffusely (Fig. 1) in the 8 patients with unifocal lung disease and in 2 of 4 patients with multifocal disease and known lung involvement (L/B, 2.23 ± 0.49 in the 10 patients with increased uptake versus 1.34 ± 0.07 in 10 control patients; P < 0.001). Lung uptake was moderately increased (L/B, 1.61) in patient 13, who had multifocal disease but no lung involvement according to recent high-resolution CT of the lungs. In 7 patients in whom tomographic imaging was performed, a diffuse increased uptake was observed in the lungs.

111In-pentetreotide scintigraphy of patient 2. Planar anterior (A) and posterior (B) views of chest reveal bilateral increased lung uptake (lung-to-shoulder ratio, 2.90). (C) Transverse tomographic images reveal diffuse increased uptake.
Bones
Activity in the shoulders and proximal humerus of patient 1 was increased because of the presence of abnormal activity in soft tissues (Fig. 2). Associated known cystic lesions on the proximal humerus were not distinctly identified. Patient 13 exhibited intense 111In-pentetreotide uptake in the distal femur (Fig. 3).
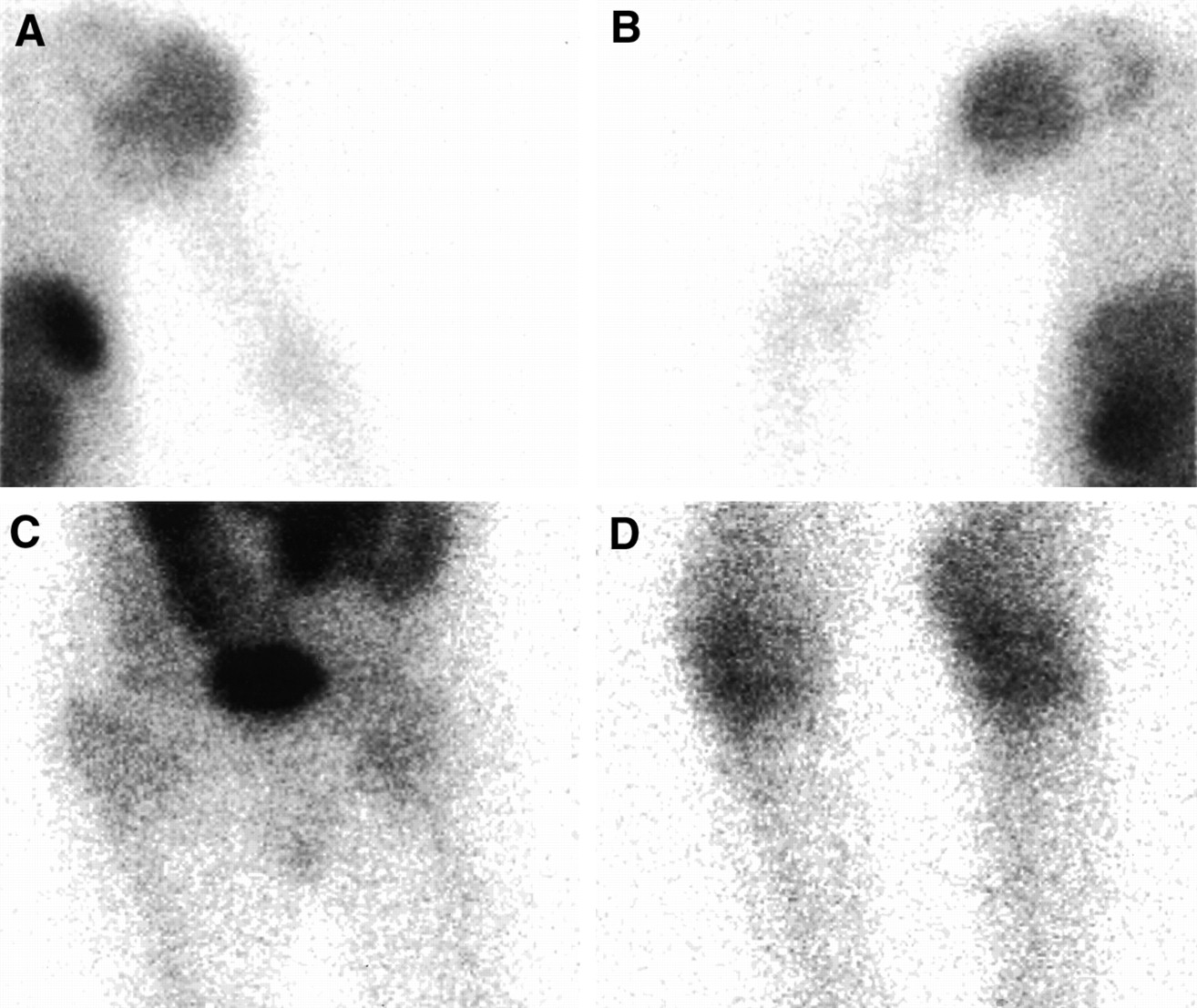
111In-pentetreotide scintigraphy of patient 1. Planar anterior views of left (A) and right (B) upper limbs, pelvis (C), and inferior limbs (D). Note increased uptake of 111In-pentetreotide in soft tissues around shoulders, hips, and knees.
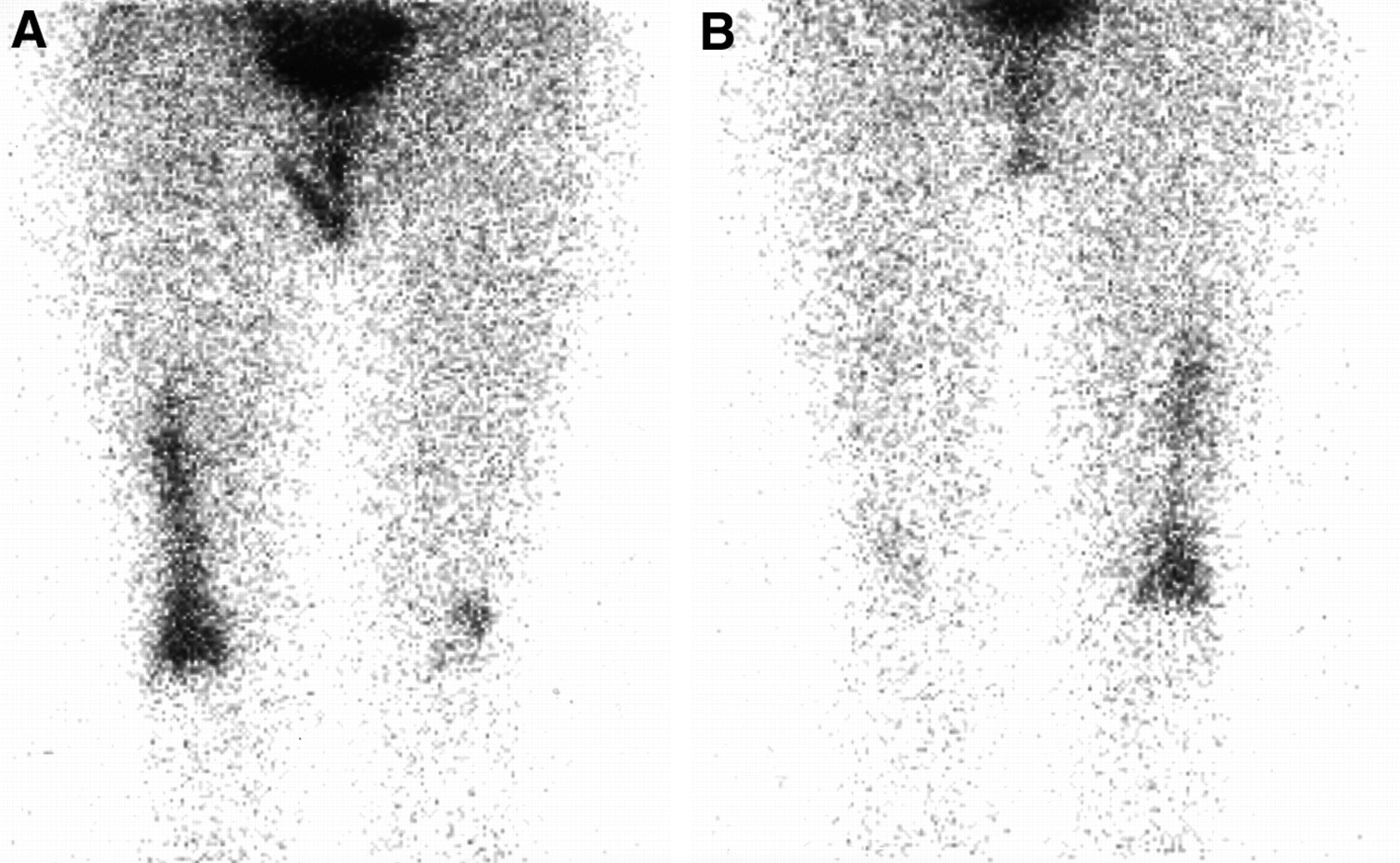
111In-pentetreotide scintigraphy of patient 13. Planar anterior (A) and posterior (B) views of inferior limbs. Note increased uptake of 111In-pentetreotide in right distal femur and knee and in left knee.
Central Nervous System
No significant uptake was observed in the cerebellum or brain stem of the 4 patients with central nervous system involvement. Among the 3 patients with diabetes insipidus, patient 10 exhibited a slightly increased uptake of 111In-pentetreotide in the pituitary gland region on planar images in comparison with the physiologic uptake by the pituitary gland. No increased uptake was found in the same region on planar images of the 2 other patients (patients 3 and 8).
Skin
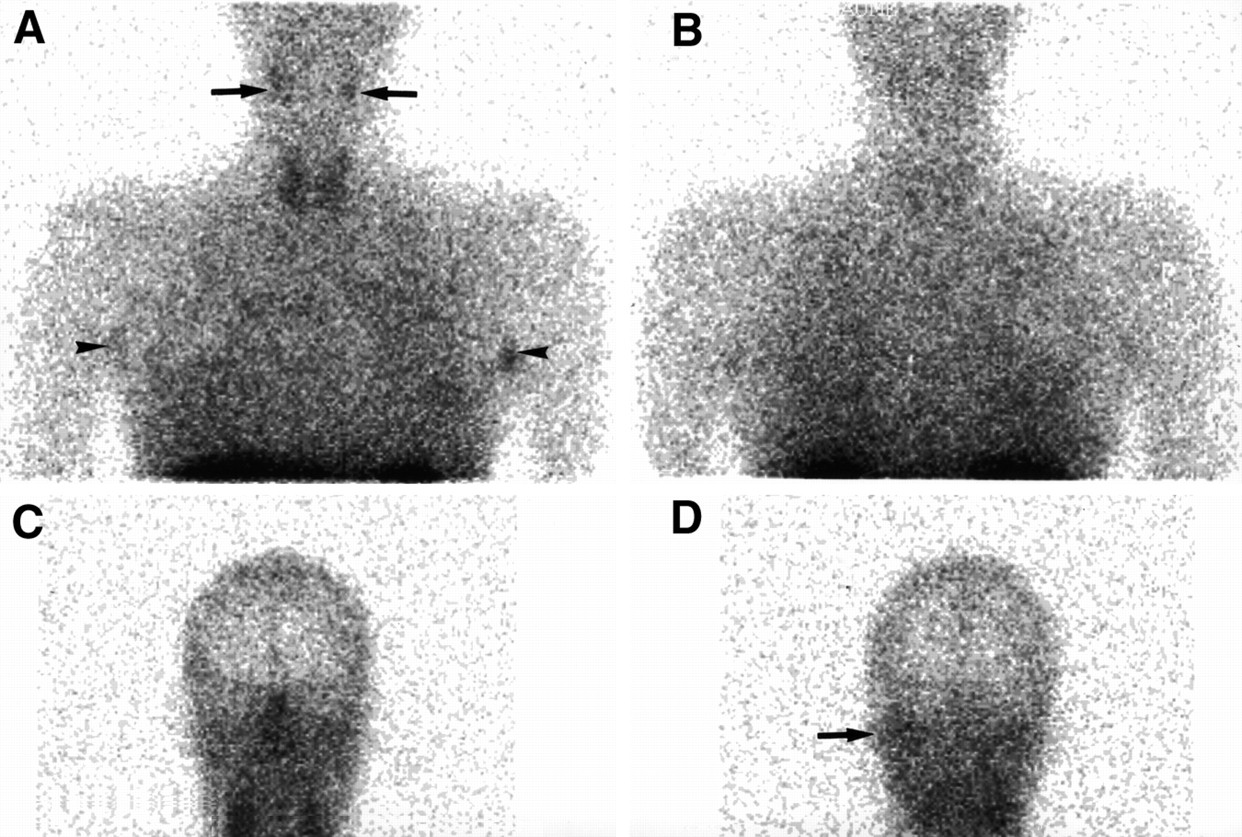
Patients 3 and 10 exhibited increased uptake of 111In-pentetreotide in the axillary region. Patient 3 also had increased uptake on the left ear (Fig. 4). However, other known lesions on the head and upper torso were not identified by 111In-pentetreotide scintigraphy. Therefore, somatostatin receptor imaging was insensitive in detecting most skin lesions.

111In-pentetreotide scintigraphy of patient 3. Planar anterior (A) and posterior (B) views of chest reveal bilateral increased lung uptake (lung-to-shoulder ratio, 2.59) and abnormal accumulation on salivary glands (A, arrows) and in axillary region (A, arrowheads). On posterior view of head (D), note increased uptake of 111In-pentetreotide of left ear region (arrow), which is faintly visible on anterior view (C).
Salivary Glands
Increased 111In-pentetreotide uptake was observed on salivary glands in patients 3 and 10, who had clinically patent involvement. Note that patients 3 and 10 had the same scintigraphic pattern with increased uptake of 111In-pentetreotide in the salivary glands and the axillary region.
Liver
No significant increased uptake was observed in comparison with the physiologic uptake by the liver.
DISCUSSION
Langerhans' cell histiocytosis is a rare disease. Diagnosis may be difficult in the early clinical stages, and identification of the involved sites and assessment of the clinical course are a challenge. Diagnostic tools that could improve assessment of the disease would be welcome.
Langerhans' cell histiocytosis is a granulomatous disease, and 111In-pentetreotide imaging has been shown to be relevant in this type of disease. Given the fact that somatostatin has been identified in Langerhans' cells, our purpose was to assess whether somatostatin receptor imaging could be useful for identifying the lesions in patients with Langerhans' cell histiocytosis. This pilot study depicts our scintigraphic findings.
In this study, we showed that most patients with lung involvement had increased lung uptake and that disease-related areas could exhibit increased uptake of 111In-pentetreotide in multifocal disease. In patients with lung involvement, somatostatin receptor imaging revealed diffuse bilateral increased uptake of 111In-pentetreotide in all but 2 patients. Because we do not know whether 111In-pentetreotide binds to Langerhans' cells, inflammatory cells, or both, the significance of increased uptake of 111In-pentetreotide by lung lesions in Langerhans' cell histiocytosis is currently unknown.
Two patients (patients 1 and 9) with destructive cystic lesions on CT had no increased 111In-pentetreotide lung uptake but had 1 of the longest time courses of evolution of the disease (diagnosis, 14 and 33 y earlier, respectively). Whether the intensity of 111In-pentetreotide uptake by lung lesions is representative of the activity of the disease remains to be evaluated.
In patients with multifocal disease, significant extrapulmonary uptake was observed in disease-related areas such as the bones, skin, salivary glands, and soft tissues. However, in patient 1, bone lesions on the proximal humerus were not seen but could have been hidden by the increased uptake of 111In-pentetreotide by the soft tissues. In patients with patent skin lesions (patients 3 and 9), somatostatin receptor imaging was insensitive for visualizing most lesions. Somatostatin receptor imaging was not relevant for visualizing lesions in 4 patients with central nervous system involvement (cerebellum, brain stem, and pituitary gland) and in 1 patient with liver involvement. However, when the central nervous system or the liver is involved, histopathologic findings reveal fibrous rather than granulomatous lesions (11,12). This also may explain our negative findings.
The limitations of this study include a small number of patients because Langerhans' cell histiocytosis is a rare disorder. Systematic brain tomographic imaging could have improved the performance of the scintigraphy, but some patients could not be held in 1 position for >30 min. On the basis of ethical considerations, lung biopsy was not performed in patients with diagnosis set on CT and could not be repeated in patients with already proven Langerhans' cell histiocytosis. The in vitro study of somatostatin receptors could not be performed at the present time.
CONCLUSION
Somatostatin receptor imaging is generally abnormal in patients with Langerhans' cell histiocytosis and lung involvement, revealing a diffuse increased uptake of 111In-pentetreotide in the lungs. In patients with multifocal disease, increased uptake of 111In-pentetreotide may be found in organs with Langerhans' cell infiltration. However, somatostatin receptor imaging was insensitive for visualizing the central nervous system, liver, and most skin lesions. 111In-pentetreotide scintigraphy may be complementary to other techniques such as CT and skeletal radiography, enabling visualization of numerous involved sites in a single examination. Further study should determine whether somatostatin receptor imaging is useful in the management of Langerhans' cell histiocytosis.
Footnotes
Received Nov. 8, 1999; revision accepted Mar. 28, 2000.
For correspondence or reprints contact: Pierre Weinmann, MD, PhD, Service de Médecine Nucléaire, Hôpital Avicenne, 125 Rue de Stalingrad, Bobigny Cedex, 93009 France.




{kind=link}
{kind=link}
{kind=link}
{kind=link}