


Abstract
We evaluated the clinical usefulness of 99mTc-pertechnetate per-rectal portal scintigraphy (PPS) in the assessment of portal circulation in children with chronic cholestasis. Methods: PPS percentage shunt index (%SI) (the amount of radionuclide that shunts the liver and reaches the systemic blood after injection in the rectum) was measured in 22 children (mean age, 7.2 ± 4.9 y) and compared with established clinical, laboratory, and endoscopic and imaging parameters of portal hypertension (PH). Fourteen children had surgically treated biliary atresia, and 8 had chronic intrahepatic cholestasis. Six clinically well children served as control subjects. Results: The %SI was 14.3 ± 3.1 and 34.7 ± 18.8 in controls and in patients, respectively (P < 0.01). A cutoff of 19% correctly allocated 100% of controls and 86% of patients. Mean %SI values were significantly higher in patients with biliary atresia, a high risk of pretransplantation death, esophageal varices (EV) at endoscopy, and an abnormal value for the ratio of lesser omentum thickness to abdominal aorta diameter (LO/Ao) at ultrasonography. Correlations between %SI values and several ultrasonographic continuous variables were statistically significant only for LO/Ao ratios (r = 0.51; P = 0.005) and spleen longitudinal diameters (r = 0.53; P = 0.01). The presence of EV could correctly be predicted only when values of %SI were greater than 30% (100% specificity; 56% sensitivity). Endoscopic and PPS findings agreed for a diagnosis of PH with EV in 3 of 7 patients with normal or borderline ultrasonographic LO/Ao ratios. PPS patterns and %SI values became normal in 3 children who underwent liver transplantation. Conclusion: In children with chronic cholestasis, PPS may be an advantageous, minimally invasive tool complementary to ultrasonography and endoscopy for better assessment and follow-up of PH before and after liver transplantation.
Portal hypertension (PH) complicating liver cirrhosis represents significant morbidity and mortality both in adults and in children (1,2). Correct diagnosis of these conditions is therefore important because of the consequences on patients’ prognosis and type of care and monitoring. Early stages of cirrhosis can be detected only by histologic and laparoscopic criteria (3,4). A precise diagnosis of early PH may require measurement of portal pressure by direct and indirect methods (5,6), which, however, suffer from complexity or high invasiveness. Several clinical criteria (e.g., the presence of splenomegaly, cutaneous collateral circulation or ascites, or hepatopulmonary syndrome) and laboratory criteria (e.g., the presence of hypersplenism or of serum levels of extracellular matrix proteins) have been taken into consideration as surrogate markers of PH or cirrhosis, but most may be poorly specific, late, or misleading (4,7–9). Ultrasonography (10–16) and upper endoscopy (10,17) are more informative, but both have several shortcomings, including isolated or combined false-positive or false-negative results, technical failures, operator dependency, and age dependency.
Per-rectal portal scintigraphy (PPS) with 99mTc-pertechnetate is a technique that explores quite specifically the collateral flow that develops in PH from the portal system to the systemic circulation through the rectal venous bed (18–20). PPS has been proposed in adults with chronic hepatitis as a sensitive and minimally invasive method for early detection of portosystemic shunts secondary to cirrhosis (20). Apart from a few cases investigated for congenital portosystemic shunt (21–23), little information on its potential use in PH staging is available in the pediatric literature (24).
The aim of the present study was to assess the role of PPS—as compared with other clinical, laboratory, sonographic, and endoscopic parameters of PH or cirrhosis—in the diagnosis and monitoring of PH in children. Because cirrhosis and PH develop in most children with biliary atresia (BA) despite an early and successful Kasai intervention (1,25,26), we chose BA as the model of pediatric liver disease most frequently accompanied by these complications, and we compared BA with chronic intrahepatic cholestasis and with absence of disease.
MATERIALS AND METHODS
Twenty-two children (15 male and 7 female; mean age ± SD, 7.2 ± 4.9 y; age range, 1–18 y) having chronic cholestasis were evaluated. Two additional patients who had been enrolled were excluded because of technical difficulty with obtaining a complete ultrasonographic study. Fourteen children had BA, and 8 had chronic intrahepatic cholestasis (3 with Alagille syndrome, 1 with biliary hypoplasia, 2 with progressive familial intrahepatic cholestasis [Byler’s disease], and 2 with sclerosing cholangitis).
All 14 children with BA had undergone surgery within 2 (n = 10) or 3 (n = 4) months after birth. At laparotomy, the liver was already cirrhotic in most (9/14). Surgical intervention had partially restored biliary flow in 11 of 14 children, who were clinically jaundice free or had moderate jaundice when enrolled in the study. Because of the persistence of residual liver disease and clinical signs of PH, however, these 11 patients were considered potential candidates for orthotopic liver transplantation (OLT). The remaining 3 patients had jaundice, and because of the high risk of death from progressive liver disease, their names were entered on the liver transplant waiting list.
All 14 children had at least 1 presumptive clinical sign of PH (e.g., splenomegaly, cutaneous collateral circulation, or ascites). Five had undergone iterative sclerosis of esophageal varices (EV) because of previous bleeding. Four (2 with an endoscopic diagnosis of high-risk EV and 2 with a previous bleeding episode) were taking oral propranolol, a synthetic agent that blocks the β-adrenergic receptor and is commonly used to reduce PH as a prophylaxis for EV bleeding.
Five of the 8 children with chronic intrahepatic cholestasis had jaundice despite ongoing treatment with choleretic drugs (e.g., ursodeoxycholic acid, phenobarbital, cholestyramine, or rifampin) when enrolled in the study. Four of 8 had histologic signs of liver cirrhosis and at least 1 clinical sign of putative PH; none had previously bled or was taking propranolol. The name of 1 with severe liver disease had been entered on the liver transplant waiting list.
Six other clinically well children (mean age, 6.6 ± 2.5 y; age range, 4.3–11.4 y) served as putative control subjects. They had a previous diagnosis of hypoxia-related benign, transient neonatal cholestasis (27); a normal liver and spleen size; and persistently normal liver function tests, including serum levels of bilirubin, bile acids, and hepatobiliary enzymes. As neonates, 4 had undergone percutaneous liver biopsy, which showed cholestasis without significant fibrotic changes.
In patients and in controls, PPS was performed according to the protocol of D’Arienzo et al. (20), with slight modifications. In brief, according to the protocol, potassium perchlorate (10–50 mg) was given orally before the test to block thyroid uptake. After the rectum had been emptied, a radiopaque polyethylene tube (2.2 mm in internal diameter) was inserted approximately 10 cm to avoid physiologic absorption toward the systemic circulation in the lower rectum. After a fluoroscopic check, a dose of 2 MBq of 99mTc-pertechnetate (specific activity, 2 MBq/0.5 mL) per kilogram of body weight was given through the tube. Each patient was placed under a large-field-of-view γ-camera (Starport; General Electric Medical Systems) equipped with a low-energy general-purpose collimator linked to an imaging computer (Microdelta; Siemens) to evaluate the liver, mesenteric portal veins, lower right lung (background), and cardiac area. Dynamic data acquisition began soon after the radionuclide had been released into the rectal lumen. A generally fairly clear image of the flux of the absorbed dose through the lower mesenteric vein was obtained. In patients with PH, the radionuclide injected in the rectum shunts the liver and appears rapidly in the heart (abnormal pattern), as opposed to the normal pattern (radioactivity first appearing in the liver). The shunt index was quantified by generating time–activity curves for a region of interest selected over the liver, including the right lobe and a portion of the left lobe, and over the right ventricle. The shunt index, which was determined by the ratio of the integral value of the heart and liver curves between time 0 and time 30 s, was therefore defined as the ratio (expressed as a percentage [%SI]) of heart radioactivity to the sum of heart and liver radioactivity (heart/heart + liver) in the first 30 s of observation. Globally, the procedure takes a few minutes, including a 4-min dynamic recording.
PPS was correlated with putative clinical or laboratory data indicating hypersplenism (WBC < 5,000/mm3 and platelet count < 100,000/mm3 (28)) and PH (e.g., collateral venous circulation and splenomegaly).
PH was investigated within the same week by esophagogastroduodenoscopy and ultrasonography also. Esophagogastroduodenoscopy was performed with a pediatric fiberoptic instrument (GIFP3 gastroscope; Olympus) without general anesthesia. Endoscopically evident EV were graded to be at a high or a low risk of bleeding according to the presence or absence of the red-spot sign or a large size (29). The presence of hypertensive gastropathy and gastric ulcers was also recorded. Ultrasonography was used to determine the ratio of lesser omentum thickness to abdominal aorta diameter (LO/Ao), which is an effective tool for detecting the presence of EV in children (12). In fact, EV are formed by portosystemic shunting via the left gastric vein through the lesser omentum into the azygous-vein tributary system in the lower esophagus. As a result, if significant EV exist, substantial blood flow must pass through the lesser omentum. The thickness of the lesser omentum was measured on left paramedian sagittal sonograms between the abdominal aorta at the origin of the celiac axis and the posterior margin of the left lobe of the liver (12). Portal vein flow, portal vein diameter per square meter of body surface area, the longitudinal diameters of the liver and spleen per square meter of body surface area, and subclinical evidence of ascites were recorded as well. Procedures were performed using real-time ultrasonography coupled with color-flow pulsed-Doppler sonography on convex equipment (Logiq 500 MD; General Electric Medical Systems) with a 3.5- or 5-MHz transducer.
PPS finally was correlated with demographic data and with clinical and laboratory variables prognostically significant for a risk of dying before transplantation (namely, serum levels of cholesterol and unconjugated bilirubin, and length of activated partial thromboplastin time) according to the score of Malatack et al. (30).
Three stable children were studied twice over a period of 6 mo. Two and 3 other patients were prospectively studied before and after prescription of propranolol and OLT, respectively. Written informed consent was obtained from each patient’s parents or legal guardian. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the local institutional Review Committee.
The results of statistical analysis are expressed as mean ± SD. The significance of differences between means was evaluated by the Student t test. The significance of differences in contingency tables was evaluated by the Fisher exact test. Correlation between continuous variables was analyzed by Spearman rank correlation. The quality of ultrasonographic Lo/AO ratio and PPS as diagnostic tests at different cutoffs was investigated in terms of sensitivity (the probability that the test is positive, given that the person has the disease), specificity (the probability that the test is negative, given that the person does not have the disease), positive predictive value (the fraction of those with positive test results who actually had the condition), and negative predictive value (the fraction of those with negative test results who actually did not have the condition), taking into account the presence of EV at esophagogastroduodenoscopy as the gold standard of PH. A 2-sided P value less than 0.05 was considered to indicate statistical significance. The statistical analysis was performed using the Statistical Package for Social Sciences (release 11.5.2.1; SPSS Inc.) for Windows (Microsoft) and StatsDirect statistical software (release 2.3.7).
RESULTS
Endoscopic Studies
Endoscopy showed EV in 16 of 22 patients (73%): 12 of 14 (86%) with BA (including also all those with previous sclerosis) and 4 of 8 (50%) with chronic intrahepatic cholestasis (P = 0.14). Two of 16 patients (13%) had large EV occupying more than one third of the lumen; 2 patients (1 with large EV) had the red-spot sign (high-risk EV). A significant gastric lesion (portal hypertensive gastropathy) was recorded only in 2 patients with BA. None of the 6 controls had endoscopic evidence of EV or gastric lesion.
Ultrasonographic Studies
LO/Ao Ratios.
The studies of 4 children had to be repeated because of difficulties in determining lesser omentum thickness. For 2, the thickness of the lesser omentum could not be calculated on repeated examinations either, and therefore they were not included among the 22 patients compared in this study. Patients had LO/Ao ratios significantly higher than those of controls (1.62 ± 0.31 [range, 1.0–2.20] and 1.10 ± 0.19 [range, 1.0–1.2], respectively [P = 0.0007]).
As shown in Figure 1, an ultrasonographic LO/Ao ratio threshold of 1.6 yielded 13 of 16 (81%) true positives and 4 of 6 (67%) true negatives for the detection of EV: sensitivity = 81.25% (95% confidence interval [CI], 54.35%–95.95%); specificity = 66.67% (95% CI, 22.28%–95.67%); predictive value of positive test = 86.67% (95% CI, 59.54%–98.34%); predictive value of negative test = 57.14% (95% CI, 18.41%–90.10%). By lowering the threshold for EV to 1.3 as described by De Giacomo et al. (13), 16 of 16 (100%) true positives and 4 of 6 (67%) true negatives for the detection of EV are found: sensitivity = 100% (95% CI, 79.41%–100%); specificity = 66.67% (95% CI, 22.28%–95.67%); predictive value of positive test = 88.89% (95% CI, 65.29%–8.62%); predictive value of negative test = 100% (95% CI, 39.76%–100%).
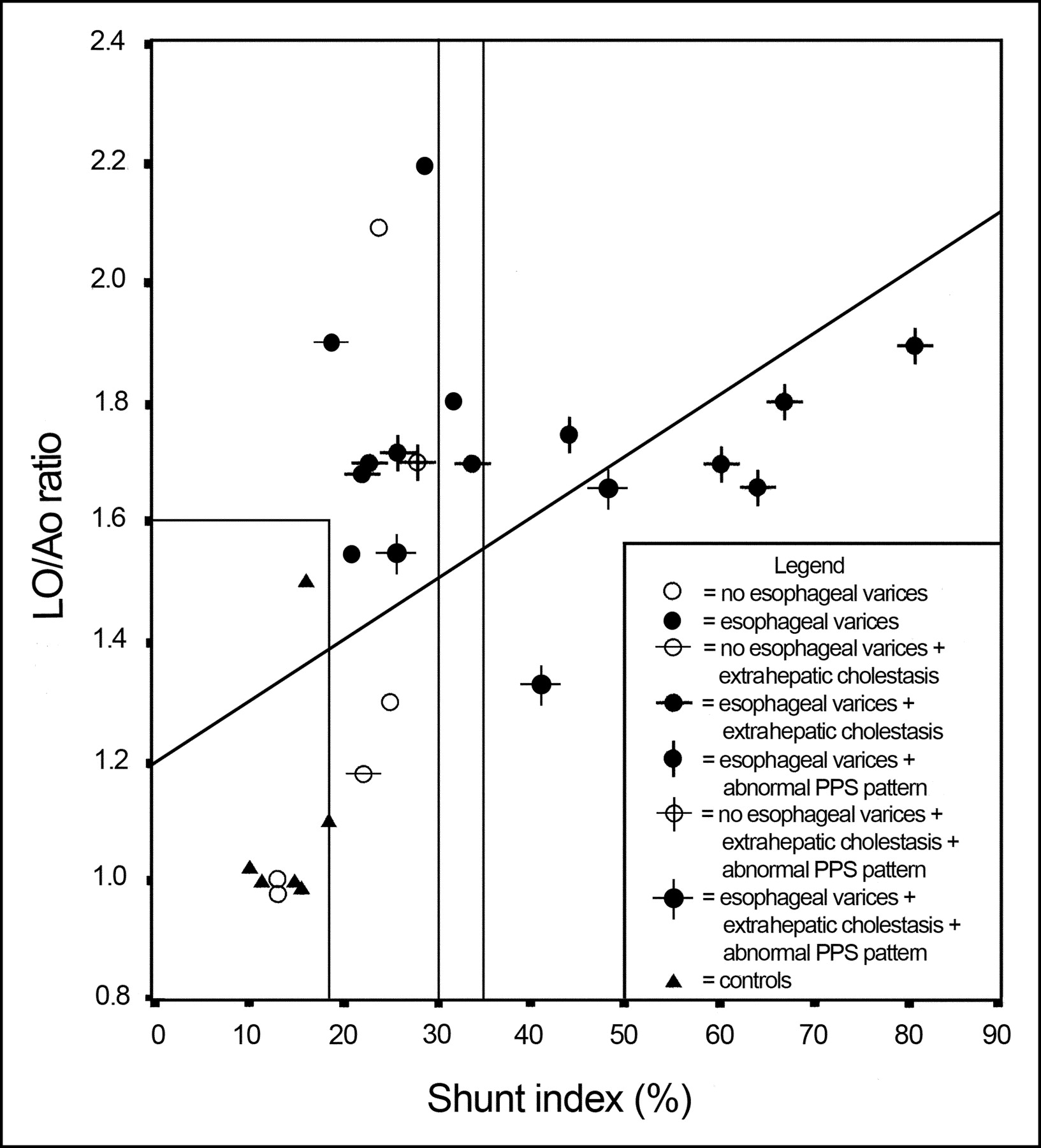
Correlation (r = 0.51; P = 0.005) between scintigraphic %SI and ultrasonographic LO/Ao ratio in controls and in patients with and without EV. Rectangle in left corner shows upper normal limits of LO/Ao ratio and of %SI. The 30 %SI limit increased specificity for the presence of EV to 100%. The 35 %SI limit individuates most cases with abnormalities of both PPS pattern and %SI.
However, mean LO/Ao ratios were not significantly different between patients with EV and those without (1.65 ± 0.06 vs. 1.59 ± 0.20), between patients with high-bleeding-risk EV and those without (1.66 ± 0.08 vs. 1.64 ± 0.07), between patients with hypersplenism and those without (1.69 ± 0.07 vs. 1.64 ± 0.07), or between patients with a high risk of death before transplantation and those without (1.67 ± 0.16 vs. 1.63 ± 0.07), according to the score of Malatack et al. (30).
Other Ultrasonographic Parameters.
Portal veins were patent in all, and portal flow and diameters did not disclose statistically significant differences between patients and controls (20.2 ± 0.8 vs. 23.7 ± 0.63 cm/s and 10.3 ± 0.7 vs. 9.9 ± 0.5 mm, respectively) or between EV-positive and EV-negative subjects (20.0 ± 1.1 vs. 20.7 ± 1.0 cm/s and 10.4 ± 0.8 vs. 10.3 ± 1.2 mm, respectively). The direction of portal vein flow was hepatopetal in all controls and patients, excepting 2 patients with BA. Normalized by body surface area, ultrasonographic spleen size was significantly larger in patients than in controls (15.7 ± 5.6 vs. 9.1 ± 1.40, P = 0.01) and in EV-positive than in EV-negative patients (19.4 ± 2.5 vs. 14.9 ± 4.5, P = 0.02). Ultrasonographic liver sizes were not different among groups.
PPS Studies and Correlation with Clinical, Laboratory, and Instrumental Data
PPS was performed in all 22 patients and in all 6 controls. No technical failure was observed, and the procedure was well tolerated by all. Reproducibility was within 10% in 3 stable patients studied twice within 6 mo.
PPS Patterns and %SI
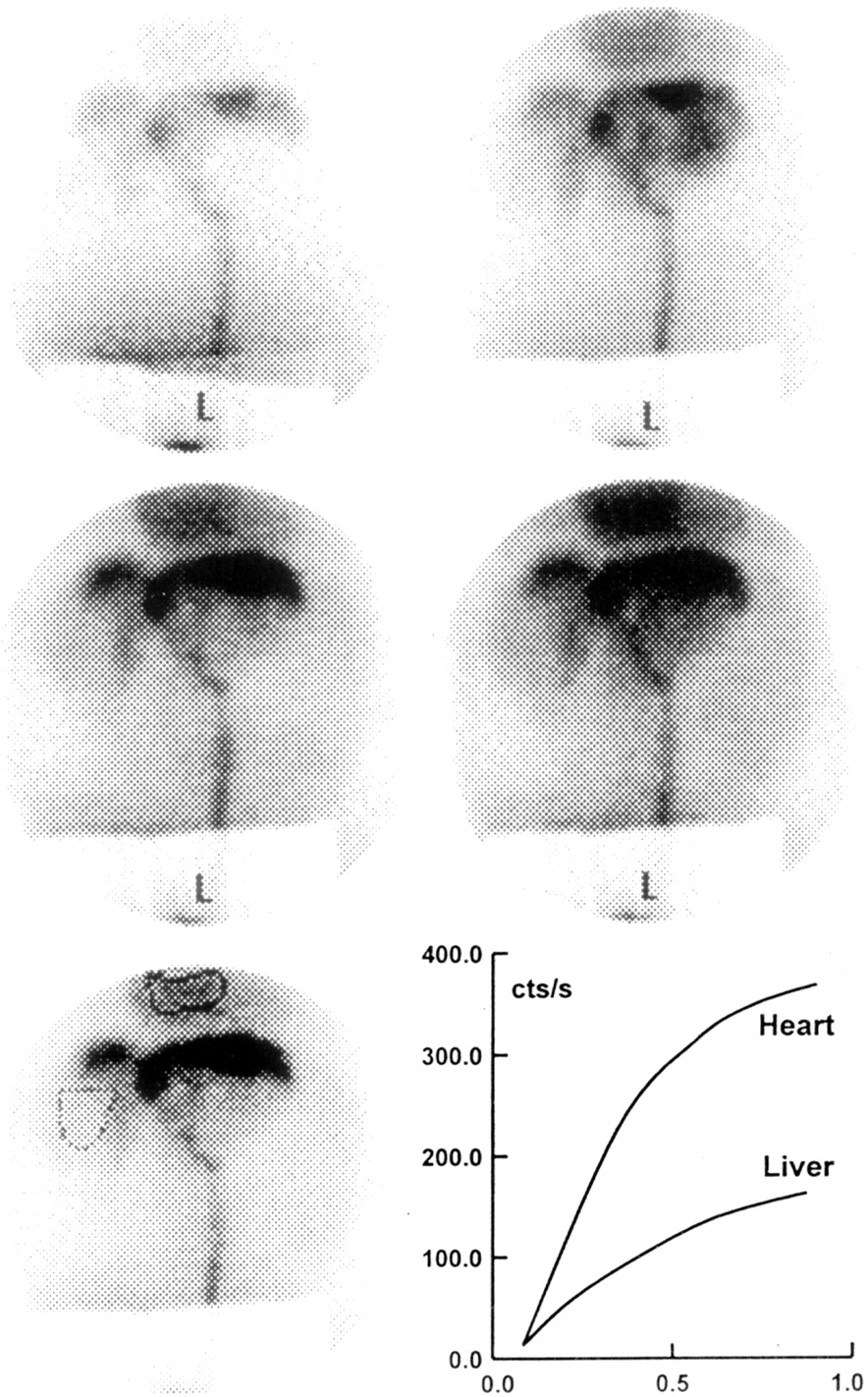
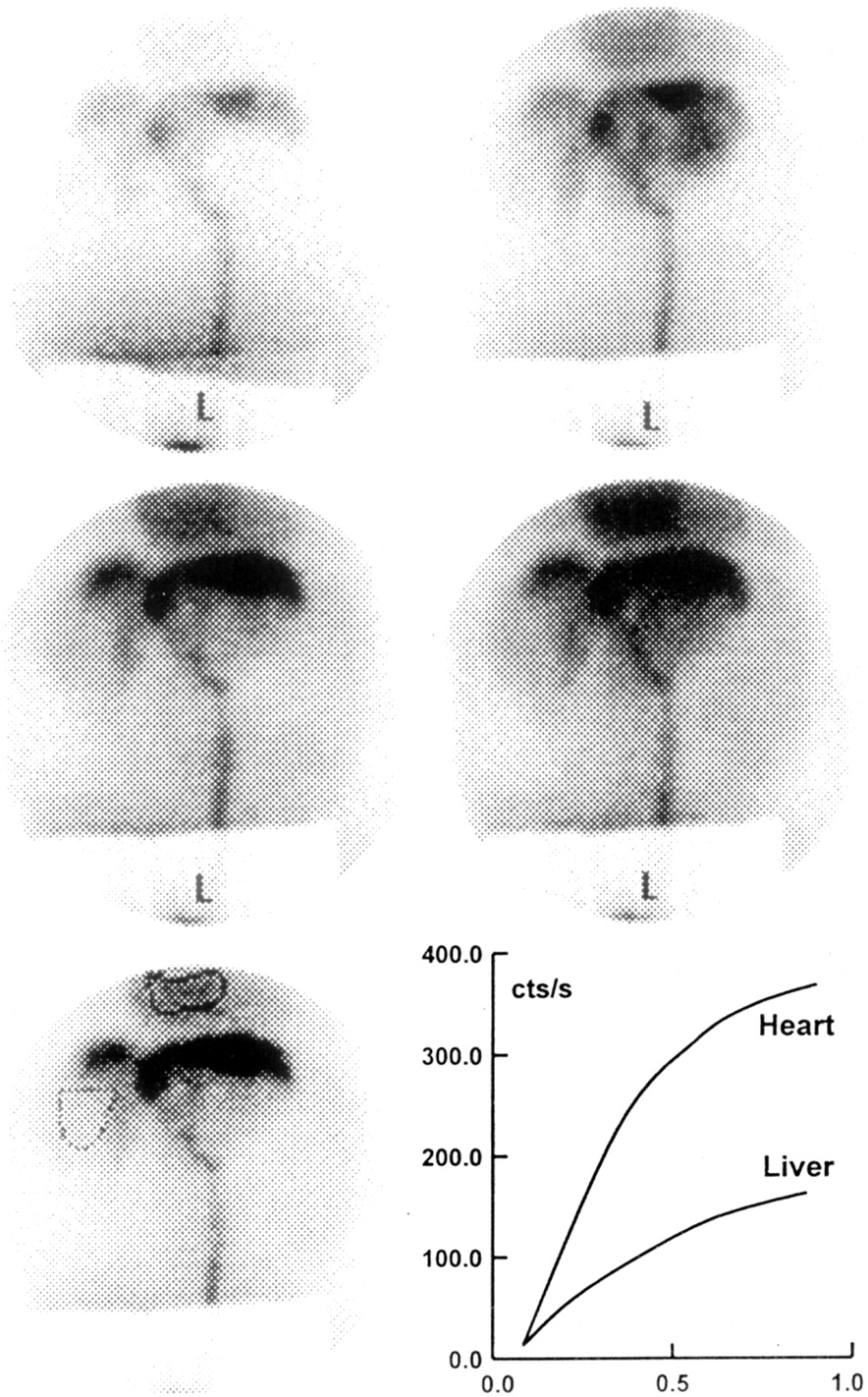
Figure 2 shows an example of a normal PPS pattern and rates of radionuclide uptake by liver and heart over time in a control subject. Figure 3 is a scintigraphic image of abnormal blood flow and the time–activity curves in a patient with PH.

99mTc-Pertechnetate PPS of a healthy subject. Images show scintigraphic appearance of normal blood flow after release of radioactive bolus into upper part of rectum trough medium. Also visible are the superior hemorrhoidal plexus and the inferior mesenteric vein up to porta. In the so-called normal pattern, the liver perfusion precedes arrival of the radioactive bolus at the heart. The time–activity curves at lower right, generated from regions of interest that were well delineated over the liver and heart images, are characterized by an upsloping liver curve that stays over the heart curve.
99mTc-Pertechnetate PPS of a PH patient with esophageal and gastric varices and ascites. Images show abnormal blood flow in upper part of rectum, via flow from inferior cava vein into varices, and diffusion of pertechnetate in the subdiaphragmatic space. Liver image is markedly delayed with respect to heart image. The time–activity curves at lower right, generated from regions of interest that were well delineated over the liver and heart images, are characterized by inversion of the heart curve, which stays over the liver curve.
PPS patterns were normal in 6 controls (100%) and in 12 patients (55%) (P = 0.06). Patients with BA had an abnormal pattern more frequently than did patients with chronic intrahepatic cholestasis (64% vs. 13%, P = 0.03). Abnormalities of PPS patterns tended to be more frequent in subjects with EV (9/16, or 56%) than in those without EV (1/6, or 17%), but the difference was not statistically significant and was independent of propranolol treatment. PPS patterns were always normal when %SI was less than 25% and abnormal when %SI was greater than 35%.
Mean values of %SI were higher in patients than in controls (34.7 ± 18.8 vs. 14.3 ± 3.1, P = 0.01) and were higher in patients with EV than in those without EV (47.8 ± 19.8 vs. 27.4 ± 13.5, P = 0.009), irrespective of propranolol treatment. %SI values were also significantly higher in patients with BA and in those with a high risk of death, abnormal LO/Ao ratios, or abnormal PPS pattern (Table 1).
%SI Values in Patients vs. Control Subjects and in Patients Allocated to Different Subgroups
As shown in Figure 1, a %SI cutoff less than 19 allocated correctly all 6 controls and 19 of 22 patients (86%) (13/16 [93%] with BA and 6 of 8 [75%] with chronic intrahepatic cholestasis). Fifteen of 19 patients (79%) with a %SI greater than 19% and 1 of 3 patients (33%) with a %SI less than 19% had EV (P = 0.17): sensitivity = 93.75% (95% CI, 69.77%–99.84%); specificity = 33.33% (95% CI, 4.33%–77.72%); predictive value of positive test = 78.95% (95% CI, 54.43%–93.95%); predictive value of negative test = 66.67% (95% CI, 9.43%–99.16%).
As shown in Figure 1, a higher cutoff for %SI (namely >30) increased specificity for the presence of EV (from 33.33% to 100%) but lowered sensitivity (from 93.75% to 56.25%). Seven of 9 patients (78%) with a %SI greater than 30 and 3 of 13 (23%) with a %SI less than 30 had an abnormal PPS pattern (P = 0.03). The association between %SI values ranging from 19% to 30% and abnormal PPS pattern (i.e., radioactivity first appearing in the heart) was always consistent with ultrasonographic data of PH in individual patients but could not significantly increase either sensitivity or specificity for EV detection. As shown in Figure 1, an abnormal pattern was always present when %SI was greater than 35% (7/7 subjects had an abnormal pattern when %SI was greater than 35; 3/15 subjects had an abnormal pattern when %SI was <35; P = 0.001).
Correlation of %SI with ultrasonographic parameters was statistically significant only for spleen longitudinal diameter (r = 0.53, P = 0.01) and ultrasonographic LO/Ao ratio (r = 0.51; P = 0.005), not for portal vein flux, portal vein diameter, or liver longitudinal diameter. %SI did not correlate with age. Patients for whom %SI was greater than 19 and LO/Ao ratio was greater than 1.6 tended to have more chances of having EV than did patients with an LO/Ao ratio less than 1.6, but the difference was not statistically significant. Regardless of the result of ultrasonographic LoO/Ao ratio, combination of %SI with LoO/Ao ratio at several cutoffs shows that the presence of PH with EV is highly probable when %SI is greater than 30. In contrast, the presence of PH with EV is unlikely when %SI is 19 or less.
Among 7 patients (3 EV-positive and 4 EV-negative) with normal LO/Ao ratios, PPS detected 5 (including those 3 with EV) who had PH, as determined by a positive %SI (%SI > 19% in 5/5) or an abnormal PPS pattern (in 2/5) (Fig. 1).
Follow-up Studies
Repetition of the PPS test after 3–6 mo for 3 stable patients gave comparable results, thus showing a high reproducibility for the method. In 2 other (EV-positive) patients who underwent the test before and 6 mo after propranolol prescription, a statistically insignificant decrease of 20% and 22% from the initial %SI was observed. In 3 other patients with severe PH whose names had been entered on the waiting list, the course of the liver disease went downhill and OLT was necessary. Normalization of both PPS pattern and %SI were observed within 6–12 mo after OLT (%SI was 49, 48, and 41 before OLT and 22, 26, and 18 after OLT).
DISCUSSION
To our knowledge, this report is the first indicating that PPS is a safe and easy procedure for the evaluation of PH in children, and we have also established its complementarity to endoscopy and ultrasonography. The percentage of patients with PH, as inferred from the presence of EV at endoscopy (our gold standard), in the present series of children with BA is in keeping with data reported by other authors (1,17,31). On the other hand, probably because of the heterogeneity of etiologies, little information exists in the literature on the diagnosis and incidence of PH in children with chronic intrahepatic cholestasis (1). In our series, the incidence of PH in patients with intrahepatic chronic cholestasis evaluated by endoscopy, ultrasonography, and PPS was approximately half that in patients with BA, and this finding also agreed with “surrogate” clinical data. None of the controls had either sign or symptom of PH.
Because the presence of EV has been considered a reliable reference for underlying PH in most adult and pediatric studies of PH, we compared the ultrasonographic and scintigraphic findings with the presence of EV at endoscopy.
Ultrasonographic evaluation of the portal venous system and detection of enlarged splanchnic vessels had little or no value as predictors of EV in our pediatric study. A possible reason is the age dependence of the size of the portal vein (11,14), without statistically significant differences between children with PH and controls (11). Also, reversal of portal blood flow direction—an important aspect of adult PH (16,32)—was not informative and occurred in only a small percentage (9%) of our children, within the same order of magnitude as that previously described for pediatric PH (11). Ultrasonographic spleen size normalized by body surface area was significantly higher in patients than in controls but could not correctly differentiate patients with EV from those without, unlike findings in adults (33).
On the other hand, our study confirmed that a collateral flow from the portal system to the systemic circulation through lower omental vessels (increased thickness of lesser omentum) develops frequently in children with chronic cholestasis, especially those with BA. However, this parameter cannot be considered a gold standard, since ultrasonography-positive diagnoses of PH in patients with endoscopic signs of EV were not higher than 81% and negative diagnoses of PH in patients without endoscopic signs of EV were lower than 67%. In addition, individual values of LO/Ao ratios could not help to distinguish cases with from those without EV. These drawbacks of ultrasonography are not surprising and agree with previous studies (11–13) reporting that not all patients with PH have a greatly thickened lesser omentum: 30% of patients in the series of Brunelle et al. (11) had a lesser omentum–to–aorta ratio of 1 or 2 and 15% had a ratio less than 1. Similarly, Sokal et al. (10) found enlargement of the small omentum in only 70% of children in a series with EV mainly due to chronic cholestasis. De Giacomo et al. (13), using 1.7 as the upper limit of normal for LO/Ao ratio among 23 children with EV, found 4 false negatives (all with an LO/Ao ratio of 1.5) and, using a ratio of 1.8 among 11 children without EV, found 2 false positives. The same authors, when considering a lower limit of 1.3 for the LO/Ao ratio, could detect no false negatives and 3 false positives (91% predictive value for EV). Moreover, false-positive results (i.e., tick and echogenic lesser omentum) may be encountered in obese children with no liver disease and in patients treated with steroids (11). Finally, technical difficulties with measuring the lesser omentum thickness may be possible as well (12): In our hands, repetition of ultrasonography was necessary in almost one fifth of patients, leading to an inconclusive result in half.
All these data may therefore moderate the originally claimed value of this noninvasive ultrasonographic ratio for the detection of pediatric patients at risk of having PH with EV. In our series, the choice of a different upper limit of normal for the LO/Ao ratio, that is, 1.3 (13), might have correctly allocated all EV-positive cases, but it was not exempt from false-negative EV results. The latter phenomenon might in part be explained by the observation that hypertensive portal circulation in the EV district may peculiarly decrease in the follow-up of pediatric patients with chronic cholestasis. In fact, interestingly, despite the common occurrence of PH in BA and the reported severity of the EV bleeding outcome (34–38), in our series and those reported by Sokal et al. (10) and, more recently, Miga et al. (2) only a small number of patients presented a picture so severe as to necessitate surgery for this complication. The probable reason is spontaneous regression of EV and development of new portosystemic shunts in some patients (1,13,17,39). This phenomenon is thought to be peculiar to the liver in growing children (40), and accordingly we believe that—at least in children—absence of EV might not always mirror absence of PH (13,17,39,40).
Our study has shown that 93% of patients with BA have an abnormal %SI, a figure close to the 92% of Ikeda et al. (24). In most patients, formation of portosystemic collaterals in the inferior mesenteric vein district, as detected by PPS, does coexist with the formation of “large” EV in children with either intra- or extrahepatic chronic cholestasis. When viewed as a predictive tool for the presence of EV, PPS is seen to have several drawbacks. Abnormal PPS %SI values consistently indicated the presence of EV at endoscopy but, similar to LO/Ao ratio, the values were not closely related to the size of the varices and were not able to predict a high risk of bleeding in patients who had endoscopic signs of such a risk. However, elevated values of %SI were correct early predictors of bleeding in the 2 children who had high-risk EV and bled within the 6-mo clinical follow-up despite prophylactic propranolol and antacid therapy. This bleeding was probably due to the severity of PH in these patients.
Accordingly, a high value for %SI, but not a high value for the ultrasonographic LO/Ao ratio, suggested the possibility that a patient was at increased risk of dying before transplantation. PPS patterns were always normal in controls and were abnormal in only a subgroup of patients, especially when %SI was highly positive (>35%). An abnormal %SI was always consistent with ultrasonographic data of PH in individual patients.
In patients whose endoscopic test is negative for EV and with a negative ultrasonographic LO/Ao ratio but positive PPS results, the latter might have had a role in early detection of PH that either had not yet developed EV or had no ultrasonographic abnormalities suggestive of PH. Although a lower threshold (i.e., 1.3) might be considered more precise for diagnosis of EV at ultrasonography, the occurrence of several false-positive diagnoses of EV both at ultrasonography and at scintigraphy remains a problem. Again, as discussed earlier, these pitfalls might result from the development of collaterals other than those leading to EV (4). Our follow-up preliminary studies support this hypothesis.
CONCLUSION
Our data suggest that PPS is a safe and useful procedure in children with chronic cholestasis, especially those for whom detection of the LO/Ao ratio at ultrasonography is technically difficult or impossible. PPS may also be complementary to ultrasonography and to endoscopy in the evaluation of early PH. In particular, PPS helps to better allocate patients who have clinical evidence of PH but whose ultrasonographic LO/Ao ratios or endoscopic findings are either normal or equivocal. Further studies are warranted to evaluate whether the use of PPS alone or combined with ultrasonography may allow lengthening of the intervals between surveillance with endoscopy, a procedure that is often poorly accepted by children. According to our preliminary results, PPS also seems a promising, minimally invasive tool for monitoring PH in patients undergoing OLT or who start taking propranolol.
Acknowledgments
The authors thank Dr. Alfredo Iovine for help in managing the patient database and Prof. Philip Rosenthal for useful comments and help in revising the manuscript.
Footnotes
Received Feb. 12, 2004; revision accepted Apr. 29, 2004.
For correspondence or reprints contact: Pietro Vajro, MD, Dipartimento di Pediatria, Università di Napoli “Federico II,” Via S. Pansini 5, 80131 Napoli, Italy.
E-mail: vajro{at}unina.it
REFERENCES
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.