Article Text

Statistics from Altmetric.com
The aorta represents a complex organ system which begins in the aortic ring adjacent to the aortic root with the origin of the two major coronary arteries, and ends at the iliac bifurcation. The subdivision into seven segments seems to be clinically important—the aortic root, the ascending aorta, the ascending aortic arch, the vessel bearing arch, the aortic isthmus, and the thoracic descending and abdominal aorta. The aorta as an organ can be regarded as a biological “windkessel”, storing kinetic energy during systole which is delivered during diastole in order to maintain a relative constant mean aortic pressure. In particular, a high diastolic blood pressure is important for the coronary perfusion.
The size of the aorta decreases with distance from the aortic valve in a tapering fashion. The normal diameter of the ascending aorta has been defined as <2.1 cm/m2 and of the descending aorta as <1.6 cm/m2.1 The normal diameter of the abdominal aorta is regarded to be less than 3.0 cm. The normal range has to be corrected for age and sex, as well as daily workload.
The aortic wall consists of three layers: intima, media, and adventitia. The intima is thin, the media contains the elastic fibres and smooth muscle cells forming a spiral layer of tissue providing the strength of the aortic wall, and the adventitia provides the nutrition with the arterial and venous vasa vasorum. An inner vasa vasorum from the aortic lumen also seems to be present.2 A wall thickness of < 4 mm is regarded as normal.
AGEING
During life the size of the aorta increases. The normal expansion rate is about 1–2 mm/year. It involves all segments which, during childhood and in young adulthood, result in an increase of the luminal diameter of the entire aorta (figs 1 and 2).3 In adulthood the aortic size is related to exercise and workload. The ageing of the aorta is accompanied by a loss of compliance, and an increase of wall stiffness caused by structural changes including an increase in the collagen content and formation of intimal atherosclerosis with calcium deposits.1,4,5 As a result pulse pressure is enhanced and pulse wave velocity raised, decreasing the resulting organ perfusion, particularly the predominant diastolic myocardial perfusion.
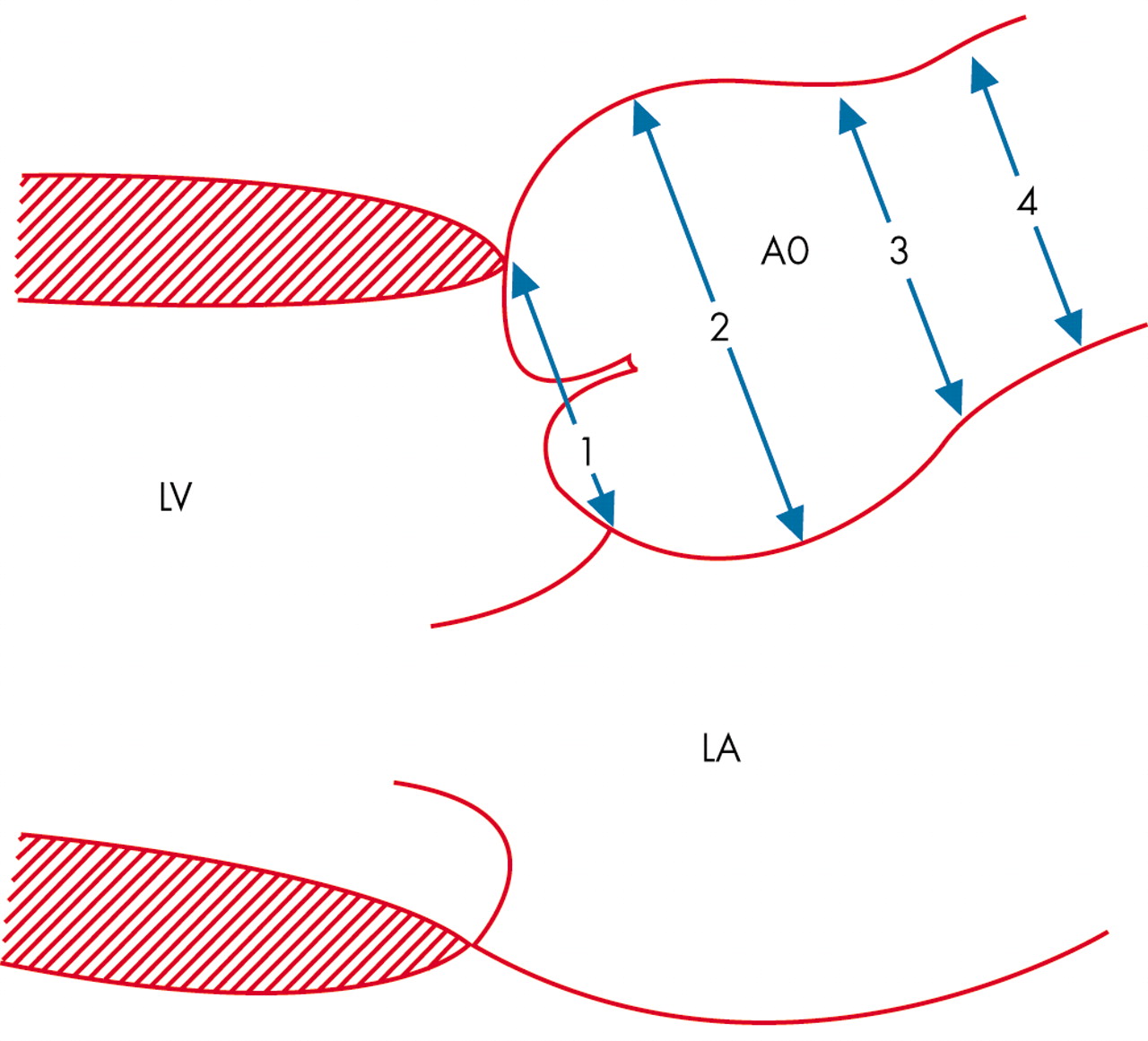
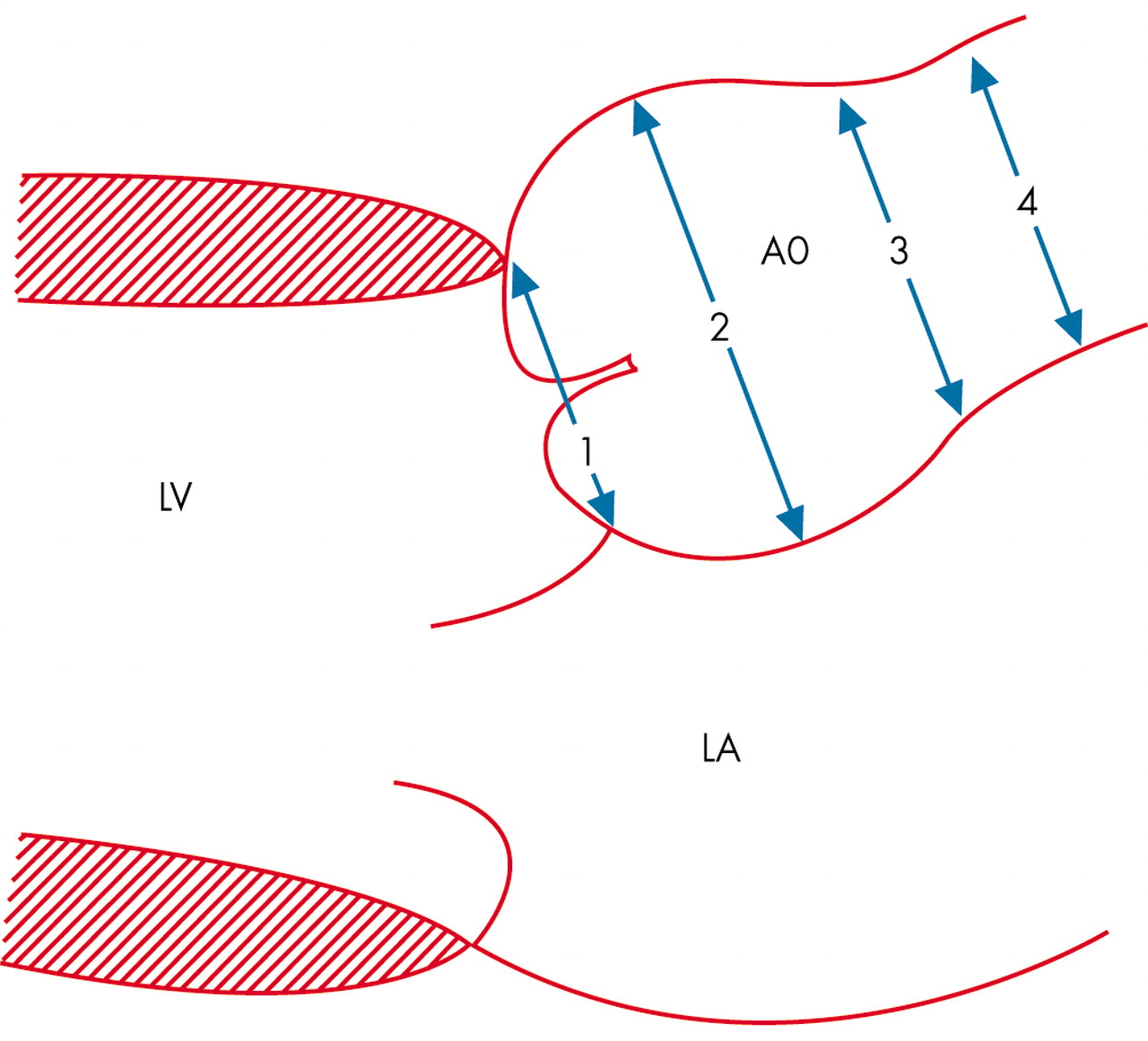
Schematic presentation of the longitudinal parasternal view with four regions where aortic diameters are measured for follow up analysis in Marfan’s syndrome. LA, left atrium; LV, left ventricle; 1, valve annulus; 2, aortic sinuses; 3, sinotubular junction; 4, proximal ascending aorta. Reproduced from Roman et al,3 with permission from Exerpta Medica Inc.

Aortic diameter changes related to body surface area (BSA) for the four different regions illustrated in fig 1. Useful for follow up studies and detection of abnormal enlargement of the aorta in Marfan’s syndrome. Reproduced from Roman et al,3 with permission from Exerpta Medica Inc.
Aortic sclerosis is subdivided into four stages:
-
intimal thickening
-
atheroma formation
-
protruding plaques
-
intimal flap and/or thrombus formation.
Aortic sclerosis risk factors are hypertension, hyperlipidaemia, diabetes mellitus, and smoking. A thickness up to 7 mm is regarded as the upper normal tolerance limit.1
The incidence of ruptured thoracic aneurysms in individuals aged 60–69 years is about 100 cases per 10 000, in those aged 70–79 years it is about 300/10 000, and in those aged 80–89 years the incidence is 550/10 000.6
DEFINITIONS
An enlargement of the aortic diameter exceeding at least 50% of the normal range represents an ectasia, which results in aneurysm formation when the ectasia exceeds tolerance limits.5
There are different forms of aneurysms:
-
true aneurysm means enlargement of the inner lumen caused by vessel wall expansion
-
false aneurysm (also called pseudoaneurysm) means lumen enlargement caused by perforation (penetration) of all parts of the vessel wall forming an outer sack in communication with the inner lumen of the aorta
-
circumscript (localised) aneurysm means that only segments of the entire aorta are involved
-
diffuse aneurysm includes an enlargement of the ascending aorta, the aortic arch, the descending thoracic (thoracic aortic aneurysms) or abdominal aorta (abdominal aortic aneurysm) or even the whole aorta
-
the term dissecting aneurysm should not be used.
ANEURYSM FORMATION
Three major inherited disorders are known to cause aortic diseases such as Marfan’s syndrome, Ehler-Danlos syndrome, and other familial forms of connective tissue diseases. For Marfan’s syndrome more than 100 mutations have been identified at one locus on the fibrillin gene.7 The prevalence is about 1/5000.8 It accounts for 6–9% of all dissections.9 Complications are aortic aneurysms, aortic regurgitation caused by aortic ring dilatation, and aortic dissection. Other familial clusters of thoracic aortic aneurysms have also been identified in about 20% of 1600 patients.10 It has been suggested that this number may be even higher, when new imaging techniques are used for screening. Ehler-Danlos syndrome belongs to the group of connective tissue syndromes.
The isolated aneurysm formation of the ascending aorta has been regarded as a “forme fruste” of Marfan’s syndrome, but represents a specific genetically determined disease. The aortic arch is usually not involved.11 In these patients an association with the bicuspid aortic valve (BAV) is found (table 1) with a prevalence 1%.12 In a review of 21 417 cases with 161 patients suffering from aortic dissection, the prevalence of BAV was 10-fold that of controls13 and it was found in 6–10% of all dissections.14 Patients with BAV have a ninefold higher risk of dissection than those with tricuspid aortic valves.11 A high incidence of BAV is also found in cases with aortic coarctation. In patients with BAV enlarged aortic diameters are reported.14
Comparison of Marfan’s syndrome versus bicuspid aortic valve in aetiology of aortic dissection.10
Annuloaortic ectasia affects 5–10% of patients undergoing valve replacement and has been described with a familial sex linked aggregation with a probable existence of genetic heterogeneity.15,16 Five mutations have been identified.11
Abdominal aortic aneurysm formation is uncommon before the sixth decade. The process is often combined with more proximal disease.17 The prevalence in men over the age of 50 years is 5%.18,19 A familial aggregation is suggested predominantly affecting women, whereas men who are affected tend to be younger.20 A genetic mutation has been described.21
A weakening of the aortic wall can also be induced by inflammation. This can be the result of microbiological diseases or multisystem vasculitis disorders. The aortitis induced by syphilis is well known, but Staphylococcus aureus infection can also be a cause. The Kawasaki syndrome is characterised by more circumscript aneurysm formation, whereas syphilis can induce a diffuse wall thickening and aneurysm formation of the ascending aorta; penetrating ulcers can also be observed.
The risk of rupture increases with the diameter of the aorta, but also occurs in small aorta. Inflammatory cells and raised concentration of cytokines within the aneurysm wall have been observed.22 Cytokines may trigger an increased production of matrix metalloproteinase (MMP) by macrophages and smooth muscle cells.23 A strong relation between infiltration and MMP activation was found.22 Behçet disease, like other forms of vasculitis, leads more to local aneurysm formation and perforation than dissection.24 The Kawasaki syndrome is a disease with an incidence of 135/100 000 children and 8–17 cases in 100 000 children < 5 years.25 Coronary aneurysm is the main sign, but also other arterial segments can be involved. In giant cell arteritis thoracic and abdominal aneurysms are feared complications.26
Toxic substances such as cocaine and amphetamines can also lead to aortic wall thinning and aneurysm formation.
In aortic stenosis a poststenotic aneurysm formation can occur, which may even be enhanced after aortic valve prosthesis implantation.27 Previous aortic valve surgery accounts for 2–4% of patients receiving aortic root surgery.27
An important cause of aneurysm formation is related to trauma, particularly high speed accidents involving the aortic isthmus.28 About 15–20% of deaths are related to aortic trauma in these patients.
PATHOPHYSIOLOGY
Pathological/anatomical studies demonstrate typical cystic degeneration of the aortic media, mucoid material, and loss of elastic fibres. The loss of elastic fibres, deposits of mucopolysaccharide-like material, and cystic anomalies are found in Marfan’s syndrome as well as anuloaortic ectasia.29 This leads to a weakening of the wall strength and consecutive vessel dilatation. The circumferential wall stress (W) can be calculated according to the La Place law for thin wall structures: W = P × r/2 h, where P = pressure, D = diameter, r = radius, and h = wall thickness.
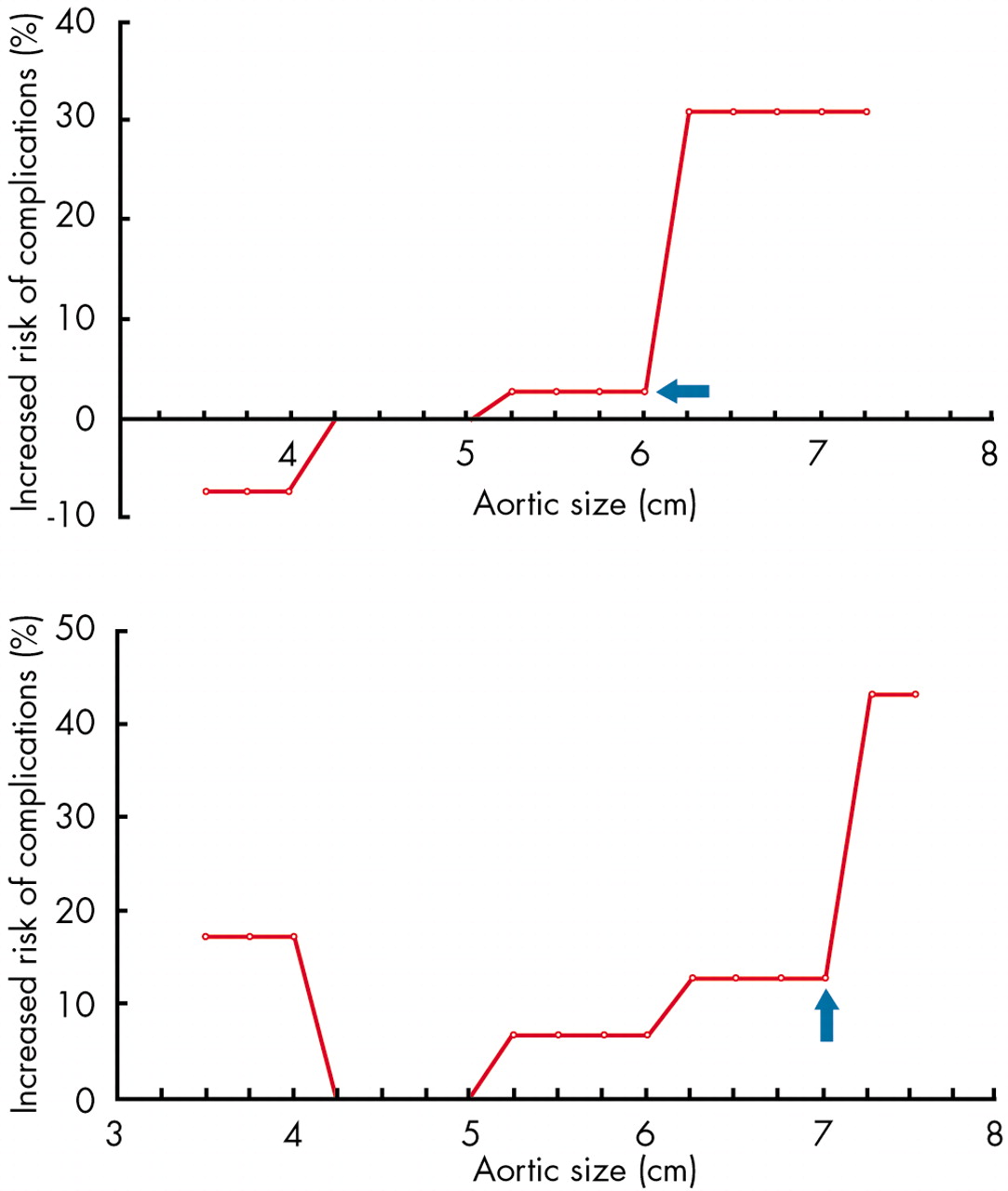
Hypertension, wall thinning, and aortic enlargement are the most important factors increasing wall stress and leading to aortic rupture or dissection.30,31 Aortic diameter is a marker of risk, but is not always enlarged. Whereas in connective tissue disease up to 40% of cases show an aortic enlargement greater than the normal range, in other forms this is found in only up to 10% of cases. The critical point of rupture (fig 3) is at 6 cm for the ascending aorta and 7 cm for the descending aorta.32 When this point is reached, up to 30% of cases with enlargement of the ascending aorta and 40% of cases with enlargement of the descending aorta have suffered rupture or dissection.32

{kind=link}
{kind=link}
{kind=link}
Influence of aortic size on cumulative, lifetime incidence of natural complications of aortic aneurysm. The incidence of natural complications (rupture or dissection) is plotted along the y axis, and the aortic size is plotted along the x axis. The plot for the ascending aorta is shown in the upper panel and for the descending aorta in the lower panel. Note the hinge point at 6 cm and 7 cm. Reproduced from Elefteriades,10 with permission from Elsevier Science Inc.
The yearly risk of complications can be calculated:
Ln λ = −21.055 + 0.0093 (age)
+0.841 (pain) + 1.282 (COPD)
+0.643 (descending aorta diameter) + 0.405 (abdominal aorta diameter).32 Probability of rupture within one year = 1−e−(365)
For both the thoracic and the abdominal aorta, aortic sclerosis was only a weak predictor of expansion.33,34 Patients with the most atherosclerotic burden had the slowest growth of the abdominal aorta.35 Smoking increased the growth rate by 15–20%, but this effect is too small to provide a guideline for screening smokers and non-smokers.34
CLINICAL FEATURES
Aortic aneurysms are silent as long as there are no complications, because no symptoms are produced by enlargement of the aortic diameter alone, except when rapid overexpansion occurs. Pain receptors are located in the adventitia so that as long as an intact structure is present, pain is not produced.
Aortic regurgitation is a typical consequence of ascending aortic aneurysm formation caused by an aortic ring dilatation with or without valve degeneration. Also circumscript pseudoaneurysm of the aortic root can lead to aortic regurgitation when the aortic ring is destroyed, which is seen more often in mycotic aneurysm, particularly when related to endocarditis involving the aortic–mitral connective triangle. The aortic regurgitation may even be the first sign of the aneurysm formation. It may be several years before patients become symptomatic.
Aortic dissection and rupture is related to aortic diameter and expansion rate in many situations (table 2). The mean (SD) expansion rate in the ascending aorta is 1.3 (1.2) mm/year, in the descending aorta it is 3.1 (3.2) mm/year, and in the abdominal aorta it is 2.6 mm/year (1 to 6.1 mm/year). The diameter accelerates as the aneurysm enlarges.34
Yearly complication rates as a function of aortic size10
The main risk factor is smoking. The aortic diameter is, however, similar in those with and without dissection, but the risk of complication accelerates beyond a diameter of 6 cm for the ascending aorta and 7 cm for the descending aorta.32 The risk of rupture, dissection, and death is in the range of 5–6.5% below 6 cm and more than 14% above 6 cm.32
SURGICAL AND ENDOVASCULAR MANAGEMENT
Aortic dissection and/or rupture are the most severe complications of aortic aneurysm formation leading in urgent or emergency situations to high operative risk (table 3).36–41 Operative mortality has been reported to be 1.5% for elective surgery, 2.6% for emergency, and 11.7% for urgent surgery.
Current risk of thoracic aortic surgery10
Thus, elective surgery has been recommended for aneurysms of the ascending aorta beyond 5.5 cm in patients with Marfan’s syndrome and 6.0 cm for those without connective tissue disease.1
Reoperation was necessary in 10–20% of the patients during a follow up of 10–20 years, with a trend for more reoperations in those with valve preserving aortic root reconstruction versus composite graft replacement (16% v 5%). A predictor for reoperation was found to be an annulus of > 2.5 cm.38 Other predictors were found to be Marfan’s syndrome, mitral valve prolapse, preoperative atrial fibrillation, aortic valve preserving operation, and concomitant procedures performed with a mean (SD) time to reoperation of 4.5 (5) years.39 Recurrent aortic aneurysm was found in 3.5%, mitral valve disease in 2%.
Long term problems can arise from anticoagulation. Thrombembolism is reported in up to 0.42/100 patient-years.36 Valve thrombosis was observed in 1% and life threatening haemorrhage in 2% of 203 patients with a mean period of 5.4 (4.9) years to the event. Endocarditis was found in 1% of cases only, but usually within one year after surgery. Main predictors of late death are female sex, increased age, non-treatment with β blockers, mitral regurgitation of +3–4 at presentation, mitral ring calcification, postoperative dysrhythmia, and postoperative use of inotropes. The overall 20 year survival rate reaches 50%.39
For the aortic arch, surgical intervention is most likely to be the method of choice, which is nowadays increasingly combined with graft stent implantation in order to seal the distal aortic arch to the descending aorta. Special systems have been designed, so that the implantation can be performed in an antegrade strategy.41,42
For the thoracic descending or thoracoabdominal aortic aneurysm, current surgical strategy has been developed during the last 15 years in order to prevent ischaemic complications. The technique for spinal cord protection can reduce the rate of paraplegia from about 15% to less than 5%. Also the rate of renal failure (serum creatinine elevation > 50% above baseline) could be reduced from about 60% to 20%.43
Aortic dimension and dissection: key points
-
Aortic dimensions increase with age and the wall thickens leading to aortic sclerosis, the most common aortic disease graded into four categories
-
The larger the diameter, the greater the expansion rate
-
Aneurysm formation is common in Marfan’s syndrome and accounts for 6–9% of dissections; familial clusters of thoracic aortic aneurysm account for 20%
-
Bicuspid aortic valve patients are at increased risk and account for 6–10% of all dissections
-
Inflammatory diseases have a potential risk for aortic aneurysm formation, such as Behçet’s disease, Kawasaki syndrome, and syphilis
-
Trauma, as well as aortic surgery of any kind, can lead to aneurysm formation and is responsible for 2–44% of patients undergoing aortic surgery
-
Critical points of rupture have been established—6 cm for the ascending aorta and 7 cm for the descending aorta
-
Surgery is recommended well before these levels are reached—in Marfan’s syndrome when the diameter exceeds 5.5 cm
-
Current management strategy includes surgery for type A dissection and medical treatment for type B dissection, with endovascular treatment on the horizon
In one report the five year survival rate of 1773 patients reached nearly 75%, compared to only 20% in another report.41,44 Over a 10 year period, the extent of the disease had no influence on patients’ prognosis, which was in the range of 50%.41
Nowadays, for circumscript, localised aneurysm formation, either true or false aneurysms, and for chronic or in some situations for acute aortic dissection, percutaneous stent graft implantation has become an alternative option.45–49 Despite the limited number of patients treated and the limited follow up time, this technique could even be used in emergency situations with high procedural and clinical success rates.50 The prerequisite is close cooperation of cardiologists, radiologists, anaesthetists, and cardiovascular surgeons, because the optimal strategy has to be chosen. The success rate today reaches 95%.50,51 The positioning of the 10 or 14 cm long stent graft—which for some types is not covered for the first part of the graft but covered with Teflon or Dacron for the distal segments—has been regarded as crucial. Positioning in the thoracic aorta can be supported using the transoesophageal approach, whereas for the abdominal aorta use of the intravascular ultrasound probe located in the inferior vena cava is suggested. Lowering the blood pressure by up to 50 mm Hg or the administration of adenosine to lower the heart rate is essential before deploying the stent graft, otherwise a sudden blood pressure rise or shifting of the stent graft can occur with dislodgement. The ratio of stent graft size to aortic diameter should be of the order of 1.1–1.15 with healthy areas before and after the aneurysm neck. Higher diameters have to be avoided in order to limit the vessel wall stretch which may result in antegrade or retrograde dissection or perforation. Angiography after implantation will reveal immediately wall apposition of the stent. If endoleaks are found, additional balloon inflations may be necessary to achieve good strut apposition to the wall. It may also be necessary to implant a second stent.
After stenting, patients can usually be extubated rapidly and after some days discharged. In some patients an inflammation is seen, described as graft disease, leading to some chest discomfort which responds well to corticosteroid treatment.
Hybrid techniques—the combination of stent graft placement and open visceral bypass grafting—have also been described.52–54 For the abdominal aorta even fenestrated grafts, additional visceral grafts, and directly anchoring the distal landing site have also been described.55–58
REFERENCES
Footnotes
-
Take the online multiple choice questions associated with this article (see page 130)
-
In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article
Linked Articles
- MULTIPLE CHOICE QUESTION