Article Text

Statistics from Altmetric.com
Positron emission tomography (PET) studies of the heart focus on evaluation of myocardial blood flow and metabolism.1 These measurements must frequently be correlated with changes in left ventricular (LV) contraction to delineate myocardial viability fully.2 Usually, this requires assessment of myocardial contraction using a different imaging modality; however, this information may be obtained at a different time and in different planes from the PET studies. In segments displaying impaired contraction, the preservation of glucose metabolism is a marker of jeopardised but viable myocardium in patients with coronary artery disease.
We describe a pilot study using ECG gated PET with18F-flourodeoxyglucose (FDG) to detect segments with reduced wall thickening. Wall thickening is compared to ECG gated cine-magnetic resonance imaging (MRI). MRI is well validated for the assessment of myocardial motion and thickening in patients with normal and impaired LV contraction.3
The study population comprised nine patients (all men) with ischaemic heart disease and LV impairment, from angiography. Their mean age was 62 years (range 42–75 years).
Cine-MR images were obtained in the short axis, positioned using the end systolic long axis view as the frame of reference. Acquisitions were synchronised to the ECG, using the R wave as a trigger. Seven cardiac phases were obtained with a frame separation of 80 ms. Four non-contiguous slices were imaged to cover the length of the left ventricle.
PET imaging was performed using a Siemens ECAT 31 PET scanner within one week of MR imaging. Attenuation correction was achieved by performing a transmission scan before the emission scan.18F-FDG (4–5 mCi) was injected intravenously one hour after a 50 g dose of oral glucose. The 18F-FDG emission scan, acquired 60 minutes postinjection, was gathered in ECG gated mode using the R wave. Multiple phase FDG images were produced by reforming the axial views of the left ventricle into four short axis sections using visual comparison of the long axis views of both imaging techniques, with a reconstructed and reorientated resolution of 8 mm.
Four short axis planes from MR and PET were alternatively reviewed in separate random orders in a continuous loop cine format by two observers, independently and without knowledge of the clinical data. Each of the short axis slices was divided into four segments (anterior, lateral, inferior, and septal, according to conventional anatomic landmarks). Wall thickening was graded using a three point scale (0 = absent or severely impaired wall thickening; 1 = segments with better thickening, 2 = cannot be judged). PET scoring was based on the changes in regional counts and endocardial wall position through the cardiac cycle.
For interobserver variation, scores by the two observers were compared. For intraobserver variation, the MR and PET images were assessed on a second occasion by one of the observer.
The sensitivity and specificity of gated FDG, compared to the gold standard of gated MRI, to determine myocardial wall thickening was determined using standard formulae. Intraobserver and interobserver variability were evaluated by Cohen's κ statistic.
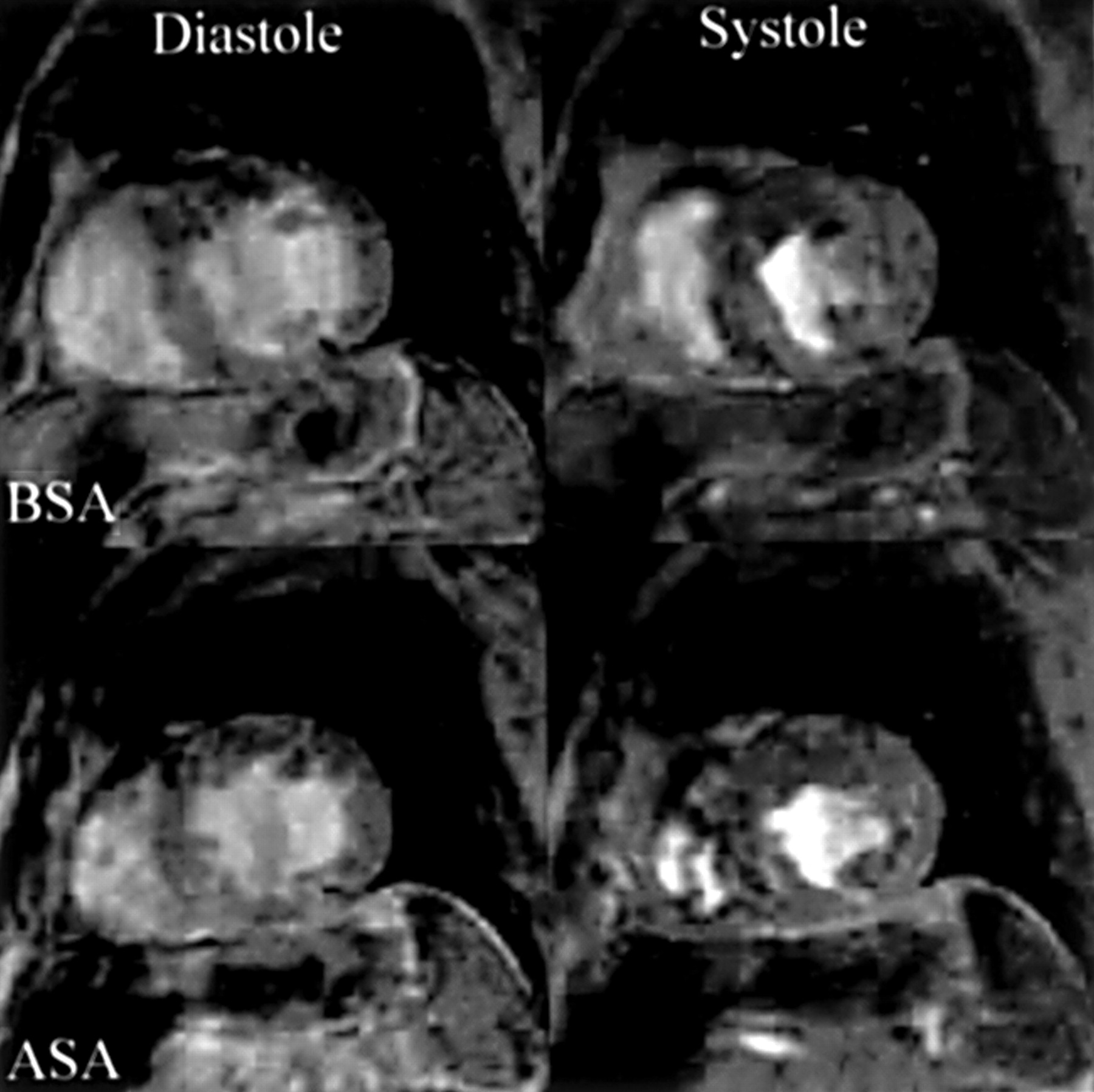
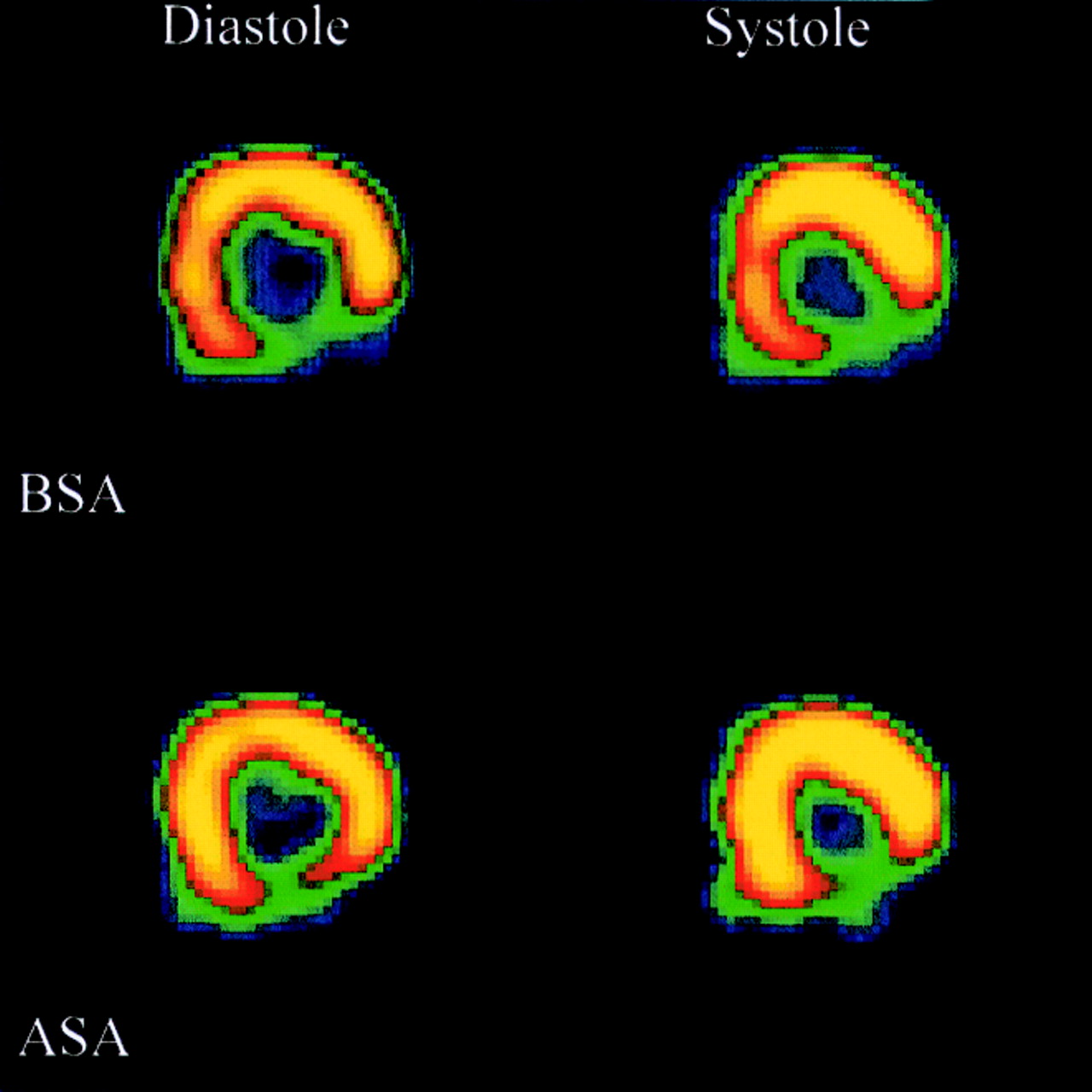
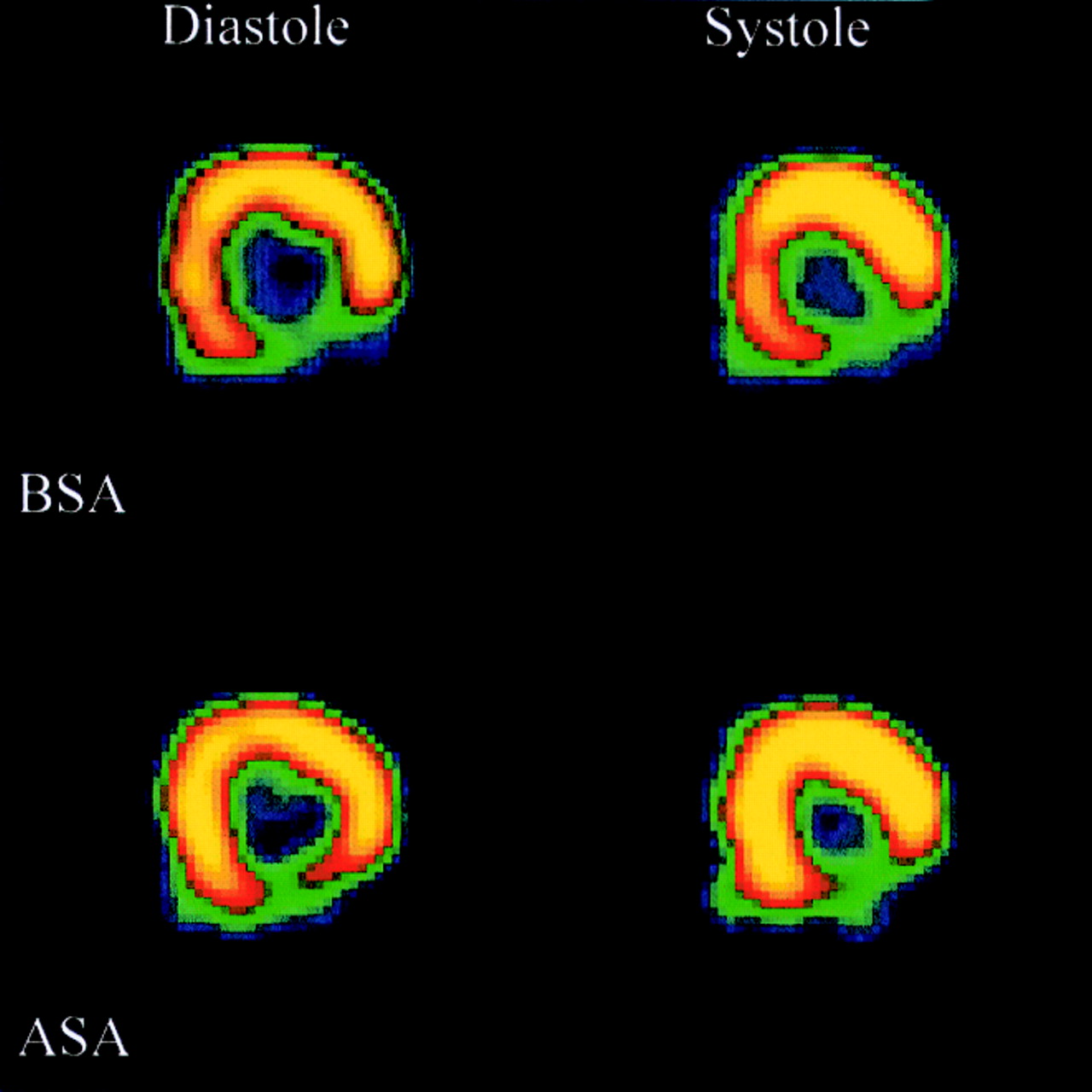
All patients underwent both studies without complication and eight had good quality images that were judged to be evaluable by the observers (fig 1). One PET examination resulted in data that were uninterpretable, and that patient was therefore removed from the study.
{kind=link}
{kind=link}
(Top) Representative diastolic and systolic frames from a cine-MRI sequence with (below) the corresponding ECG gated18F-FDG tomograms. BSA, basal short axis; ASA, atypical short axis.
Abnormal wall thickening was present in all patients, with 49 abnormal segments, 75 normal segments, and four that could not be scored. Intraobserver and interobserver reproducibility of the MR studies was 85% (κ = 0.67) and 83% (κ = 0.65), respectively.
Abnormal wall thickening was present in all patients, with 48 abnormal segments, 71 normal segments, and nine that could not be scored. Intraobserver and interobserver reproducibility of the PET studies was 95% (κ = 0.88) and 70% (κ = 0.37), respectively. Of the nine segments that could not be scored because of reduced tracer uptake, seven (78%) were found to have abnormal wall thickening and two (22%) normal wall thickening from MRI.
Of 128 segments, 13 (10%) were deemed uninterpretable because of either inadequate tracer uptake in PET or inadequate blood myocardium contrast in MR. Thus 115 segments were available for comparison (table1). Gated 18F-FDG PET and MRI showed a correlation in 93/115 (81%) segments. Taking MRI as the gold standard for the assessment of wall thickening gated 18F-FDG PET was found to have a sensitivity of 79% and a specificity of 82% for the detection of segments with severely reduced or absent wall thickening.
Comparison of determination of reduced wall thickening by MRI and ECG gate 18F-FDG
Intraobserver agreement for both modalities was 219/252 segments (87%, κ = 0.73). Interobserver agreement was 207/270 segments (77%, κ = 0.53).
PET is a highly developed tool for the study of myocardial perfusion and metabolism. In contrast to the research with flow and metabolism, little effort has been devoted to the assessment of myocardial contraction by PET. Measurement of myocardial contractility has usually been performed by echocardiography, radionuclide ventriculography or MRI. The use of different imaging modalities increases the complexity of the studies and may be affected by time differences while also requiring the accurate registration of anatomic segments from images acquired in different planes. We have validated gated18F-FDG PET for visual assessment of regional LV function at rest, against the accepted gold standard of cardiac MRI which is known to provide reliable estimates of both endocardial motion and myocardial wall thickening. PET wall thickening was judged from changes in regional counts and changes in endocardial wall position through the cardiac cycle. The combination of an increase in regional counts and change in apparent endocardial wall position has been shown to provide a method of estimating wall thickening that compensates for the partial volume effects.4 There was good overall agreement between the two methods, allowing accurate assessment of myocardial contraction in regions that are spatially equivalent to studies of metabolism.
We have assessed regional ventricular function at rest using ECG-gated18F-FDG PET. Two observers easily interpreted most of the images and there was good intra- and interobserver agreement. Patients investigated with coronary artery disease showed there was good overall agreement with MRI for segmental wall thickening. This will facilitate the integration of the assessment of myocardial metabolism and mechanical function by PET.
Acknowledgments
The authors would like to thank the Dr James Alexander Mearns Trust and the British Heart Foundation for their financial support during this study.