Article Text

Statistics from Altmetric.com
In recent years the development of non-invasive cardiac imaging has progressed rapidly. Cardiac multidetector computed tomography (CT) is rapidly becoming an integral part of clinical cardiology. On the other hand, the justification for coronary revascularisation must be based on ischaemia, not solely on anatomical narrowing of the coronary lumen.1 While several standard functional imaging techniques such as nuclear perfusion imaging, stress magnetic resonance imaging, and stress echocardiography have been well established for the detection of ischaemia, they do not provide any information about coronary anatomy.
Hybrid scanners combining positron emission tomography (PET) with high resolution multidetector CT are currently the standard for almost all commercially available systems. Hybrid scanners offer the ability to assess the anatomy of the heart and coronary arteries, and the functional evaluation either at stress (for assessment of induced ischaemia) or at rest (for viability), in association with the left ventricular systolic function. Therefore, combining functional information from PET with morphological data from CT is appealing.2
Why use PET in myocardial perfusion imaging?
Since myocardial perfusion imaging using conventional nuclear medicine techniques is well established, what could be the justification to use PET imaging instead? PET imaging offers a unique possibility to measure myocardial perfusion quantitatively in absolute terms.3,4,5,6 This is useful in patients with diffuse coronary artery disease (CAD) or balanced disease where relative assessment of myocardial perfusion cannot uncover a global reduction in perfusion (fig 1). Typically, in relative analysis of perfusion only, the regions supplied with the most severe stenosis are detected. In less severe cases multivessel disease is likely to be underestimated. Quantification of myocardial perfusion using dynamic PET provides a high performance level for the detection and localisation of CAD3 (fig 1). The incremental value of quantitative analysis was also recently studied and it was found that the accuracy of PET was further improved by quantitative analysis.4,5,6 It has also been documented that PET is more accurate in traditionally difficult patient populations such as obese and diabetic subjects.

Three dimensional cardiac hybrid positron emission tomography/computed tomography (PET/CT) image providing a panoramic view of stress perfusion and CT angiography. The images (A and B) are scaled to relative scale where the best perfused region is set to maximum and has the brightest colour (in rainbow scale lowest = blue and highest = red). The hybrid images of anterior (A) and posterior (B) views suggested no perfusion abnormalities. However, in the images scaled according to absolute scale (C and D) (0 ml/g/min = blue and 3.5 ml/g/min = red) uncovered global reduction of perfusion. The hybrid images of anterior (C) and posterior (D) views showed severely reduced stress perfusion in all myocardial regions. The finding of multivessel disease was also confirmed in invasive angiography.
For hybrid imaging there are also other clear advantages favouring the use of PET in such systems. The most important ones are listed here:
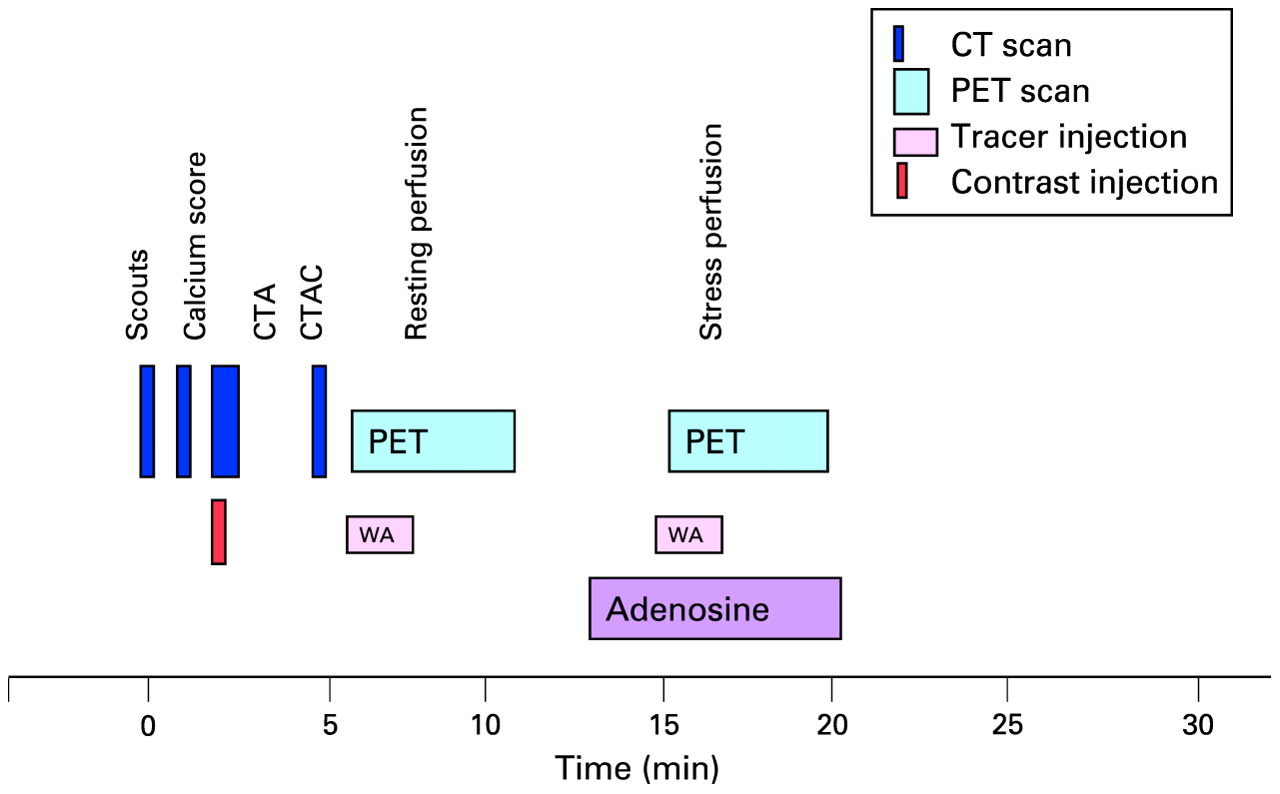
The efficiency of imaging is very good when PET/CT systems are used. The PET imaging protocols are short, allowing both CT angiography and perfusion imaging to be performed in a single session clearly below 30 min of total scan duration (fig 2).
The radiation dose for patients will be very small using the current PET/CT systems. The radiation dose from PET perfusion studies is very small—for example, radiation dose from a single PET perfusion study is 0.8 mSv for 15O-water and 1 mSv for 13N-ammonia. Recently, techniques that reduce patient dose in CT have been developed and the doses have been reduced to as low as 1–7 mSv.7 Therefore, although the use of hybrid imaging as such causes an increased radiation dose for the patient as compared to single imaging, currently comprehensive cardiac PET/CT imaging can be performed with a radiation dose below 10 mSv,8 which has been regarded as the maximum dose even for healthy volunteers.
There are other promising future applications that involve molecular imaging of cardiac targets and these may further enhance the clinical utility of hybrid imaging using PET/CT.

An example of cardiac hybrid imaging protocol using positron emission tomography/computed tomography (PET/CT) and 15O-water (WA). The calcium score imaging, CT angiography (CTA) and two perfusion imaging acquisitions can be done in 30 min. Due to the short half-life of the tracer, PET acquisitions can be performed without delay. If only stress imaging is used the protocol can be further shortened to about 15 min. O-15-water.
Why use hybrid imaging instead of image fusion?
Because imaging procedures are a significant financial burden to the overall cost of healthcare, it is important to carefully consider and justify the use of all imaging tests. The potential disadvantage of the fast development of new and tempting diagnostic techniques is that the patients may now be exposed to multiple and costly diagnostic tests and procedures, which may deliver, occasionally, contradicting results. Thus, it is rational to search for a non-invasive technique to assess CAD in which the detected perfusion abnormalities can be immediately and accurately associated with the individual’s coronary anatomy.
As previously mentioned, CT coronary angiography has proven to be valuable for the evaluation of many subgroups of patients with known or suspected CAD, but it only enables the assessment of coronary luminology, thus providing purely morphological information which has well known limitations.9,10 It has been shown that only about half of the lesions classified as significant in CT are linked with abnormal perfusion.9,10 The vasomotor tone and coronary collateral flow cannot be estimated since the per cent diameter stenosis is only a weak descriptor of coronary resistance.9,10 (fig 3).

The relationship between quantitation of luminal blockage via computer based border detection of coronary angiograms (horizontal axis) was performed in a large number of individual coronary stenoses, and their haemodynamic significance was contemplated using fractional flow reserve (FFR) (vertical axis). This measurement of the extent to which any coronary stenosis impedes flow during maximal hyperaemia is a surrogate for non-invasive functional testing, with a cut-off value of significance at 0.80, below which stress inducible ischaemia can be detected (range of normal values 0.90–1.00). Reproduced with permission from Wijns W, De Bruyne B, Vanhoenacker PK. J Nucl Cardiol 2007;14:366–70.
On the other hand, myocardial PET perfusion imaging provides a simple and accurate integrated measure of the effect of all the parameters on coronary resistance and tissue perfusion, thereby optimising selection of patients who may ultimately benefit from revascularisation. However, PET imaging does not provide morphological information. The perfusion imaging only provides information about the existence and severity of perfusion abnormalities, but not about the mechanism—for example, those patients with diffuse balanced coronary heart disease and those with microvascular dysfunction leading to globally compromised perfusion cannot be separated by perfusion imaging.
If combining image information is expected to be useful, why not simply use mental integration of the information from CT angiography and perfusion? The different orientation of image sets makes a subjective integration difficult. This may lead to inaccurate allocation of the coronary lesion to its subtended myocardial territory, particularly in patients with multivessel disease and intermediate severity lesions. In addition, standard distribution of myocardial territories corresponds with the real anatomic coronary tree in only 50–60% of cases, which may cause misleading interpretation.
Hardware based image co-registration permits the acquisition of fused anatomical and functional images using hybrid scanners with the capability to perform PET and CT image acquisition almost simultaneously, with the patient’s position fixed (fig 2). Inherently, image fusion is performed fully or semi-automatically by superposition of image datasets. An additional important benefit of fusing different imaging modalities is the ability of using the anatomical information acquired in situ to improve the scan efficiency and to use the CT images for attenuation correction of the PET scan. Last but not least, an important benefit for the patient is that a comprehensive study can be performed in a very short single session of scans.
In hybrid imaging two alternative approaches have been used. In one approach both CT and PET acquisitions are performed in all subjects; the order of the scan can be variable, although in most situations the perfusion study is performed first and CT angiography subsequently due to the need for pre-medication for CT. In another approach the CT angiography is performed first and the images briefly analysed, and PET perfusion is only then performed when abnormalities are found on the CT angiograms. The latter approach is apparently more effective but requires careful planning of logistics to enable efficient patient throughput.
Alternatively to hybrid imaging, image datasets can be acquired using stand alone scanners and fused manually using software based co-registration. Intuitively, the hardware based approach appears preferable since manual co-registration may be hampered by issues of accuracy and user interaction. However, when successful, this alternative offers advantages similar to hybrid imaging by merging functional information with anatomical data, but without the need for a hybrid device. This type of software based image co-registration may still remain a common form of hybrid imaging, since dedicated cardiac fusion software packages are now commercially available allowing hybrid imaging with an excellent interobserver reproducibility and short processing durations. In fact, such software is used irrespective of whether the images are acquired on a hybrid device or on two different stand alone scanners.
Limitations of hybrid approach
Although the hybrid PET/CT devices have been used routinely in cancer patients for a decade, there are specific challenges in fully automated hardware based image co-registration for cardiac applications.
The heart is a continuously moving organ that has beat-to-beat and respiratory variations in its position, despite fixation of the patient’s position and orientation.
The CT images are acquired using electrocardiographical gating and during breath hold. In contrast, PET perfusion images are usually acquired in non-gated and free breathing mode, resulting in a slight mismatch of ventricular size and position between the image sets.
Obviously, the small misalignment is not very critical for perfusion imaging since ischaemic lesions are typically in the centimetre rather than the millimetre range. However, for more advanced molecular imaging, such as plaque imaging, the correction of even small misalignments becomes very important. Even with perfusion imaging, if significant misalignment is not controlled, it can lead to diagnostic errors.11 Therefore, nowadays software realignment of cardiac image sets is performed even if the scans were acquired in a single session using a hybrid device.
Imaging protocols for hybrid imaging
The patient preparation for a hybrid study is practically the same as for the individual scans.12,13 Drinks containing caffeine need to be avoided during the preceding 12 h since pharmacological stressors are commonly used in hybrid imaging. Typically preparation of CT angiography requires the patient’s heart rate to be controlled with the use of β-blocking agents. Several protocols have been used for hybrid imaging, each of which have their inherent advantages and disadvantages.
In the most effective protocol the need for perfusion study is individually decided upon by the findings in CT angiography (fig 2). This protocol utilises the high negative predictive value of CT, and only that proportion of the patients who had suspicious findings on CT will continue with perfusion imaging. If the pretest likelihood of CAD is 30–70%, as it ideally should be, approximately half of the patients need sequential perfusion imaging. In this protocol CT is performed first with standard preparations. The potential limitation is that the premedication required for CT angiography may also affect the perfusion results, although this is likely to be less significant with pharmacological stressors such as adenosine and dipyridamole.
If the perfusion study is performed first, the above mentioned potential problem is avoided; however, currently the analysis of perfusion images is not fast enough for an immediate decision to be made as to whether to omit CT angiography in the case of a completely normal perfusion result. Thus, this protocol employs both PET perfusion and CT angiography in all patients.
The comfortable positioning of the patient on the scanner bed is critical to prevent any motion artefacts during and between the scans. It is strongly recommended that hands are supported upright and not within the field of view. The calcium score study can also be performed, although its clinical value is unclear in hybrid protocols. The detailed protocol of CT angiography depends on the system used. Low dose CT for attenuation correction scan is performed if needed (in some systems calcium score or CT angiography study can be used for this).
The perfusion imaging protocol depends on which tracer is used. In hybrid imaging the stress study is performed using pharmacologic stressors such as adenosine, dipyridamole or dobutamine. With PET tracers such as 82Rb and 15O-water studies (half-lives 76 s and 112 s), the stress study can be performed practically without delay after the rest study. With 13N-ammonia stress testing is delayed for about 30 min to allow tracer decay. If a method to correct patient motion between stress and rest studies is not available, a second low dose CT scan for attenuation correction is needed. In all studies a quality control process is needed to ensure optimal alignment of the CT attenuation and PET emission scans and, if necessary, misalignment needs to be corrected.
If the system is capable of list mode acquisition, the data can be collected in ECG gated mode that allows the simultaneous assessment of regional and global left ventricular wall motion from the same scan data. This is particularly practical when Rb-82 is used as tracer. The total time required for a whole study session depends on the tracer used. With 15O-water and 82Rb the whole session can be finished in 30 min, and with 13N-ammonia in 80 min. The protocols can be further shortened significantly since in hybrid approaches only single stress perfusion imaging may be needed, especially when using quantification,6 and then the protocol with all tracers can be as short as 15 min.
If hybrid imaging is used to assess myocardial viability the standard patient preparations and procedures are used as in stand alone imaging.
Image analysis and interpretation
The analysis of PET studies follows the standard procedures that have been explained in detail in published guidelines.12,13 In addition, the analysis of CT angiography includes the standard processes and techniques used in stand alone situations, such as visual assessment of original transaxial slices, multiplanar reconstructions, and utilisation of the quantitative tools available. To make use of the true power of hybrid imaging, the fused images and data should also be utilised. In fused images the individual coronary anatomy can be linked with perfusion information. The most advanced analysis also includes visualisation of perfusion in diagnostic quality multiplanar reconstructions of CT. The absolute stress flow values should also be included in the analysis (fig 4).

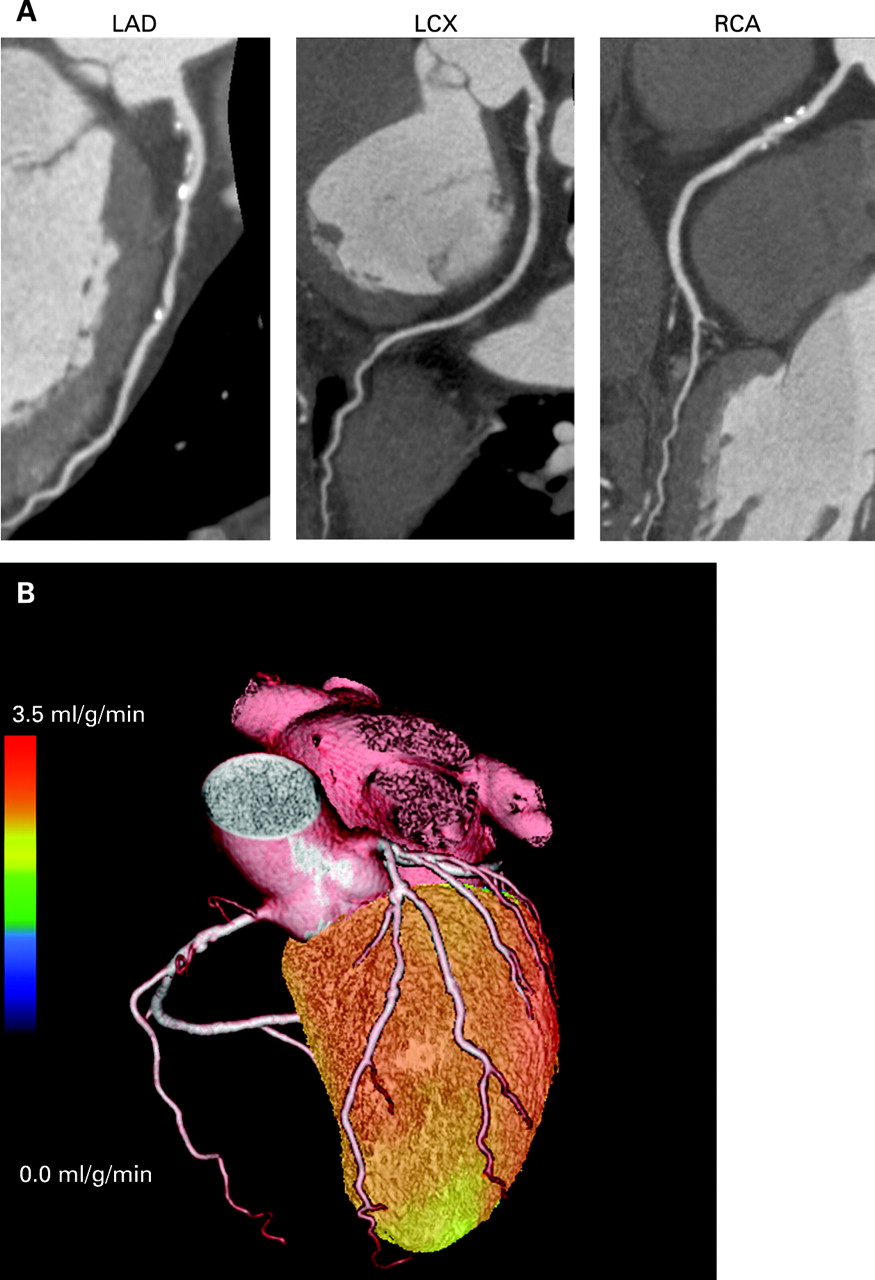
(A) Computed tomography (CT) coronary angiography images (curved multiplanar reconstructions) of a male patient with effort angina. The images of the right coronary (RCA), left anterior descending (LAD) and left circumflex (LCX) arteries show several calcified and non-calcified plaques, which suggest significant multivessel disease. (B) Three dimensional cardiac hybrid PET/CT images of the anterior view show normal stress perfusion patterns in all regions (red and yellow colour). In an invasive study no significant stenoses were identified.
Clinical impact of cardiac PET/CT
Hybrid images provide a comprehensive view of the myocardium, the regional myocardial perfusion, and the coronary artery tree, thus eliminating uncertainties in the relationship of perfusion defects, scar regions, and diseased coronary arteries (figs 1 and 4). This may be particularly helpful in patients with multiple perfusion abnormalities (fig 5). Combining anatomical information with perfusion also helps to identify and correctly register the subtle irregularities in myocardial perfusion (fig 6).

In situations of complex multivessel coronary artery disease, hybrid cardiac imaging provides accurate location of ischaemia as related to the individual’s coronary anatomy. Furthermore, quantitative analysis of perfusion gives added value in the assessment of the severity of ischaemia. In this symptomatic patient with mild effort angina, the relative hybrid images acquired during stress (anterior view A, posterior view B) showed clear findings of ischaemia in the anterior wall located in the left anterior descending artery (LAD) region. However, in the quantitative analysis (anterior view C, posterior view D) the ischaemic areas were much larger and linked also to the left circumflex artery (LCX) and also partially the right coronary artery (RCA), indicating haemodynamically significant multivessel disease.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
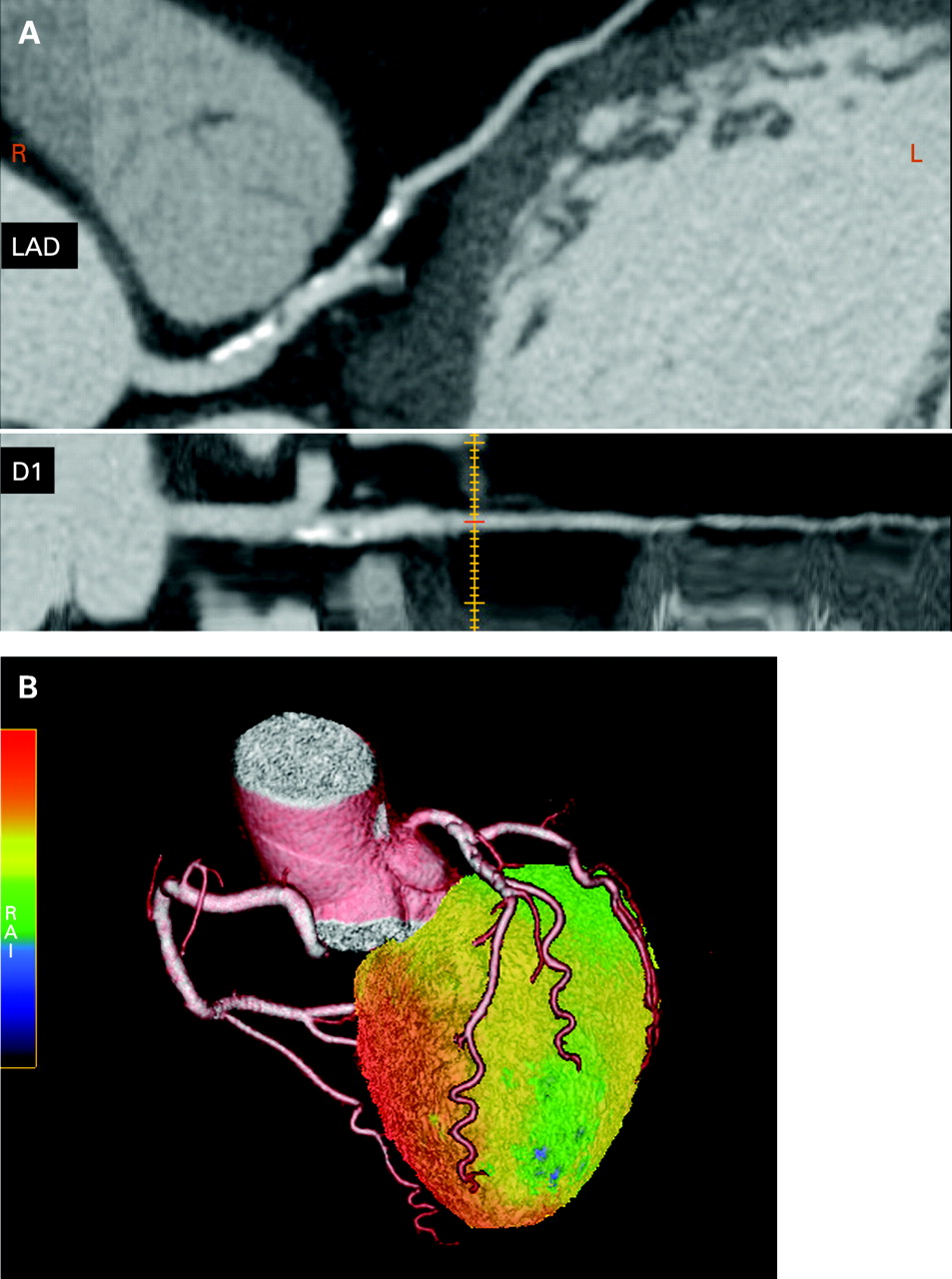
Example of symptomatic patient who had significant findings in the left anterior descending artery (LAD) and in the first diagonal branch (D1) in computed tomography (CT) angiography (A). Hybrid PET/CT imaging (B) revealed only a subtle reduction in territory supplied by D1, but perfusion was normal in the other regions.
It is well established that a comprehensive assessment of CAD requires not only morphologic information about the location and degree of coronary artery stenosis, but also functional information on the severity of the pathophysiologic lesion. In patients with suspected CAD hybrid imaging provided a sensitivity and specificity of 90% and 98%, respectively.14 Further studies are warranted to ensure the accuracy of hybrid PET/CT in different clinical populations. Furthermore, the incremental value of hybrid imaging over the stand alone individual scan needs to be defined.
Hybrid images may offer superior diagnostic information with regard to identification of the culprit vessel and therefore increase diagnostic confidence.6 The incremental value is likely to be pronounced for functionally relevant lesions in distal segments and diagonal branches, and in vessels with extensive CAD or substantial calcification on CT.15 Due to the variation in coronary anatomy and the complex disease pattern in these patients, the correct allocation of the perfusion defect and subtending coronary artery could only be achieved using the hybrid images. As hybrid images offered superior information with regard to identification of the culprit vessel, the diagnostic confidence for categorising intermediate lesions and equivocal perfusion defects was significantly improved. It is likely that the greatest added value appears to be the firm exclusion of haemodynamic significance of coronary abnormalities seen on CT coronary angiography, which likely leads to avoidance of unnecessary invasive procedures.
Another group of patients in whom hybrid imaging is likely to be clinically useful is those with multivessel CAD. Typically myocardial perfusion analysis is based on relative assessment of perfusion distribution. This technique, however, often uncovers only the coronary territory supplied by the most severe stenoses (fig 1). In multivessel disease coronary flow reserve may be abnormal in all territories, thereby reducing the heterogeneity of flow between “normal” and “abnormal” zones (fig 5). This is obviously limiting the ability of relative perfusion analysis to delineate the severity of multivessel CAD. This problem can be solved in several ways:
The response of left ventricular ejection fraction to stress can be measured from perfusion data when data are collected in gated mode.16
Myocardial perfusion is quantified in absolute terms (in ml/g/min) which is standard with 15O-water and 13N-ammonia PET and provides independent information about all myocardial territories.3,4,5,6
Anatomical information from CT is able to identify those patients with severe balanced multivessel disease, despite globally reduced but relatively homogenous myocardial perfusion.
Although assessment of myocardial viability using stand alone systems is well established, hybrid imaging may provide additional benefits. Comparable with perfusion hybrid imaging, the detected dysfunctional but viable or scar regions can be directly linked with the individual’s coronary anatomy and coronary stenoses. The limitation of a hybrid approach in this patient group may be that many patients may have other diseases that prevent the use of iodinated contrast agents.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit = men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal’s username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
Future perspectives of PET/CT
Clinical cardiac PET/CT hybrid imaging in patients with suspected CAD has attracted increasing interest recently. It appears that this approach may have the potential to become the central decision making element in the future diagnostic and therapeutic strategy for patients with CAD.9 However, more studies assessing the prognostic value and cost effectiveness of hybrid imaging are warranted. The current bottleneck which slows the increase of cardiac PET/CT is the limited access to tracers.
Currently, the best established applications of PET and PET/CT in patient care are based on perfusion and glucose metabolism imaging. However, PET allows for imaging and quantification of molecular interactions and pathways with very high sensitivity. Thus, the number of cellular processes can be studied—for example, receptor density, enzyme activity, inflammatory processes, and gene expression. Rupture of vulnerable coronary atherosclerotic lesions is the key incident in acute cardiac events. Non-invasive techniques such as multislice CT can characterise morphologic criteria associated with a high risk of atherosclerotic plaque rupture. On the other hand, PET may be used to target individual inflammatory activities in atherosclerotic plaques. This approach is possible only with hybrid imaging.
Conclusions
Cardiac PET/CT imaging is entering into routine clinical use. The combination of morphological imaging of coronary arteries using multidetector CT angiography and functional imaging of myocardial perfusion using PET is a non-invasive single imaging session technique that provides comprehensive information for diagnosis and decision making for treatment of CAD.2,9 Further data are warranted to demonstrate the cost effectiveness of this technique. In the near future, other molecular imaging applications will also enter into clinical cardiology by means of PET/CT imaging.
REFERENCES
- 1.↵
American clinical guidelines for cardiac radionuclide imaging.
- 2.↵
- 3.↵
This clinical study emphasises the absolute quantification of myocardial blood flow using 13N-ammonia.
- 4.↵
This clinical study emphasises the absolute quantification of myocardial blood flow using 15O-water.
- 5.↵
This clinical study emphasises the absolute quantification of myocardial blood flow using 82rubidium.
- 6.↵
This clinical study also emphasises the absolute quantification of myocardial blood flow using 15O-water.
- 7.↵
- 8.↵
- 9.↵
An excellent review about hybrid imaging in clinical cardiology.
- 10.↵
An important multicentre study on CT angiography.
- 11.↵
- 12.↵
European procedural guidelines.
- 13.↵
American procedural guidelines.
- 14.↵
- 15.↵
- 16.↵
Footnotes
Competing interests In compliance with EBAC/EACCME guidelines, all authors participating in Education in Heart have disclosed potential conflicts of interest that might cause a bias in the article. The author has held research contracts with GE Healthcare and St Jude Medical.