Diagnosis and management of peripheral arterial disease
BMJ 2012; 345 doi: https://doi.org/10.1136/bmj.e5208 (Published 14 August 2012) Cite this as: BMJ 2012;345:e5208
- G Peach, specialist registrar in vascular surgery,
- M Griffin, academic foundation year 2 trainee,
- K G Jones, consultant vascular surgeon,
- M M Thompson, professor of vascular surgery,
- R J Hinchliffe, Higher Education Funding Council for England clinical senior lecturer and consultant vascular surgeon
- Correspondence to: R J Hinchliffe rhinchli{at}sgul.ac.uk
- Accepted 26 July 2012
Summary points
-
Peripheral artery disease (PAD) is an important marker of overall cardiovascular disease
-
All patients with PAD should receive aggressive modification of cardiovascular risk factors
-
Most patients with intermittent claudication can be managed without revascularisation (angioplasty or bypass)
-
Less than 3% of patients with intermittent claudication require major amputation within five years
-
Patients with diabetes and smokers are at particularly high risk of developing critical limb ischaemia
-
Refer all patients with rest pain, ulceration, or gangrene for specialist assessment
Peripheral arterial disease (PAD) is an atherosclerotic process that causes stenosis and occlusion of non-cerebral and non-coronary arteries. It has an estimated worldwide prevalence of almost 10%, rising to 15-20% in people over 70 years of age,1 2 and it affects around 27 million people in Europe and North America alone.3 Critical limb ischaemia—the most severe manifestation of the disease—can lead to limb loss or even death if not treated promptly. Each year, 500-1000 new cases of critical limb ischaemia are diagnosed per million of the population, with an estimated annual cost to the NHS of more than £200m (€255m; $314m).4
Sources and selection criteria
We searched Medline, Embase, and the Cochrane Database for systematic reviews and meta-analyses related to the diagnosis and management of peripheral arterial disease. We also consulted relevant national and international guidelines published by the National Institute for Health and Clinical Excellence, the Trans-Atlantic Inter-Society Consensus for the Management of Peripheral Arterial Disease, and the International Working Group on the Diabetic Foot.
Increased awareness of the disease, enhanced medical treatment, and new endovascular interventions have dramatically improved the management of patients with PAD.5 6 With the publication of new National Institute for Health and Clinical Excellence (NICE) guidelines on the management of this disease, this review offers a timely summary of current evidence relating to PAD and provides up to date information on the diagnosis, referral, and management of this common condition.
Who is at risk?
The development of atherosclerotic PAD is a multifactorial process involving both modifiable and non-modifiable risk factors. About 65% of patients also have clinically relevant cerebral or coronary artery disease, and a large prospective cohort study showed that patients with PAD have a sixfold higher risk of death from cardiovascular disease than those without PAD.1 It is therefore extremely important to identify and treat risk factors for cardiovascular disease in these patients.
Age, sex, and ethnicity
The incidence and prevalence of PAD increase with age. Although some studies have found prevalence to be similar in both sexes, the male:female ratio is commonly reported as 2:1 for PAD and as high as 3:1 for critical limb ischaemia. Black ethnicity is also an independent risk factor for developing PAD, with an odds ratio of 2.83.7
Smoking
Smoking is the most important modifiable risk factor for developing PAD, and the causal link between the two may be even stronger than that between smoking and coronary artery disease.5 The Edinburgh Artery Study (1592 participants) found that smokers have a four times greater risk of developing intermittent claudication than non-smokers, and that patients with PAD who continue to smoke are more likely to need intervention or amputation than their non-smoking counterparts.8 9 Furthermore, a recent meta-analysis of 29 studies found that the failure rate of surgical bypass grafts is three times higher in those who continue to smoke, although this effect may be reversed by smoking cessation.10
Diabetes
Diabetes is a major risk factor for PAD and more generalised cardiovascular disease, and patients with diabetes are twice as likely as those without diabetes to develop the condition.5 PAD mainly affects the infrapopliteal arteries in these patients, and glycaemic control is of paramount importance: a meta-analysis of 13 studies found that a 1% increase in glycated haemoglobin (HbA1c) is associated with a 26% increase in the risk of developing PAD.11 PAD also progresses more rapidly in those with diabetes, and these patients are five to 10 times more likely to need major amputation (above ankle level) than patients without diabetes.12 13 People with both diabetes and end stage renal disease are at particularly high risk of limb loss.14
Ulceration in patients with diabetes usually has multiple causes, and although 50% of patients with diabetes and foot ulcers have PAD, neuropathy and infection often play a major role. Patients with diabetes and foot ulceration should therefore be seen by a multidisciplinary diabetic foot team at the earliest opportunity (ideally within 24 hours).15
Hypertension and hyperlipidaemia
Data from the Framingham Heart Study have shown that hypertension and hyperlipidaemia are independent risk factors for developing PAD.16 A blood pressure of greater than 160/95 mmHg increased the risk of developing intermittent claudication 2.5-fold in men and fourfold in women, and a fasting cholesterol concentration of greater than 7 mmol/L was associated with a twofold increase in the risk of claudication.16
Other factors
Chronic renal insufficiency, raised haematocrit, and high concentrations of homocysteine or plasma fibrinogen also seem to be linked to an increased risk of PAD, although it is unclear whether these links are causal.
How does PAD present?
Patients who develop symptoms of PAD usually present with intermittent claudication—an aching muscle pain that is brought on by exercise and rapidly relieved by rest. Symptoms are determined by the site of disease, and because PAD most commonly affects the superficial femoral artery (fig 1⇓), pain is usually felt in the calf, which is distal to the arterial stenosis or occlusion. Disease of the iliac arteries, common femoral artery, or tibioperoneal arteries may cause pain in the buttock, thigh, or foot, respectively. The presence of bilateral symptoms may indicate aortic disease, bilateral iliac disease, or a non-vascular cause.

{kind=link}
Claudication typically comes on after walking a pain-free distance (unlike the pain of osteoarthritis) and is worse when walking fast or uphill, when muscle oxygen requirements are at their highest. Although claudication distances can be inaccurate as a measure of absolute severity of disease, a change in perceived walking ability over time may be a useful indicator of clinical improvement or deterioration.
Symptoms generally develop over months or even years, with a gradual reduction in the pain-free walking distance. Rapid exacerbation of symptoms and sudden onset of claudication are important warning signs because they may indicate new arterial occlusion. This is usually caused by rupture of an atherosclerotic plaque or in situ arterial thrombosis (for example, a thrombosed popliteal aneurysm), but it may also be caused by emboli from the heart or more proximal arteries.
When patients with PAD experience acute arterial occlusion, they commonly present with deep duskiness and pain of the affected limb. This is in contrast to the classic picture of acute ischaemia (the “6Ps” of acute ischaemia: pain, pallor, pulselessness, perishing cold, paraesthesia, and paralysis) and results from the extensive network of collateral arteries that usually develops in people with pre-existing PAD. Such patients warrant urgent specialist referral.
Critical limb ischaemia is characterised by ulceration, gangrene, or rest pain consistently for more than two weeks. True rest pain usually affects the toes or foot of the affected limb (as opposed to benign night-time calf cramps), and patients often describe hanging the affected leg out of bed to ease symptoms.
What is the natural course of PAD?
Although many never experience symptoms, 7-15% of people with asymptomatic PAD will develop intermittent claudication within five years.8w1 Of those who do develop claudication, only 20-25% are likely to experience further clinical deterioration.5 Major amputation is rare (other than in patients with diabetes), and patients should be reassured accordingly—only 1-3% of patients with intermittent claudication will require major amputation in a five year period.5 17
Although some patients follow a gradual progression from asymptomatic PAD to intermittent claudication and then critical limb ischaemia, this is the exception rather than the rule, and more than half of patients undergoing major amputation for critical limb ischaemia may have had no symptoms of ischaemia as little as six months earlier.18 Furthermore, patients with PAD often have major comorbidity that limits physical activity and they may therefore develop critical limb ischaemia without preceding claudication.
For those with established critical limb ischaemia the prognosis is poor. About 12% of such patients require amputation within three months of presentation and 20-25% die within a year.5 The estimated five year survival rate for patients with critical limb ischaemia is 50-60% (worse than for many cancers),19 and these patients require urgent referral for specialist evaluation.
How to evaluate symptoms of PAD
Once a diagnosis of PAD is suspected from the history, a full cardiovascular examination is performed to identify other manifestations of cardiovascular disease. Limb temperature and capillary refill time are assessed and the feet are examined carefully for signs of tissue loss (ulceration or necrosis). It is also important to look for more subtle signs of ischaemia, such as pallor on limb elevation and hyperaemia when the leg is dependent (Buerger’s sign). These are caused by loss of capillary autoregulation in the ischaemic limb.
Palpation of the peripheral pulses helps to localise the site of the arterial stenosis or occlusion and identify other disease, such as popliteal aneurysms. If the presence of pulses is in doubt, the ankle brachial pressure index can be measured with the aid of a hand held Doppler machine (fig 2⇓). However, interpret the results with caution in patients with diabetes because heavy arterial calcification may give rise to artificially high ankle pressures.
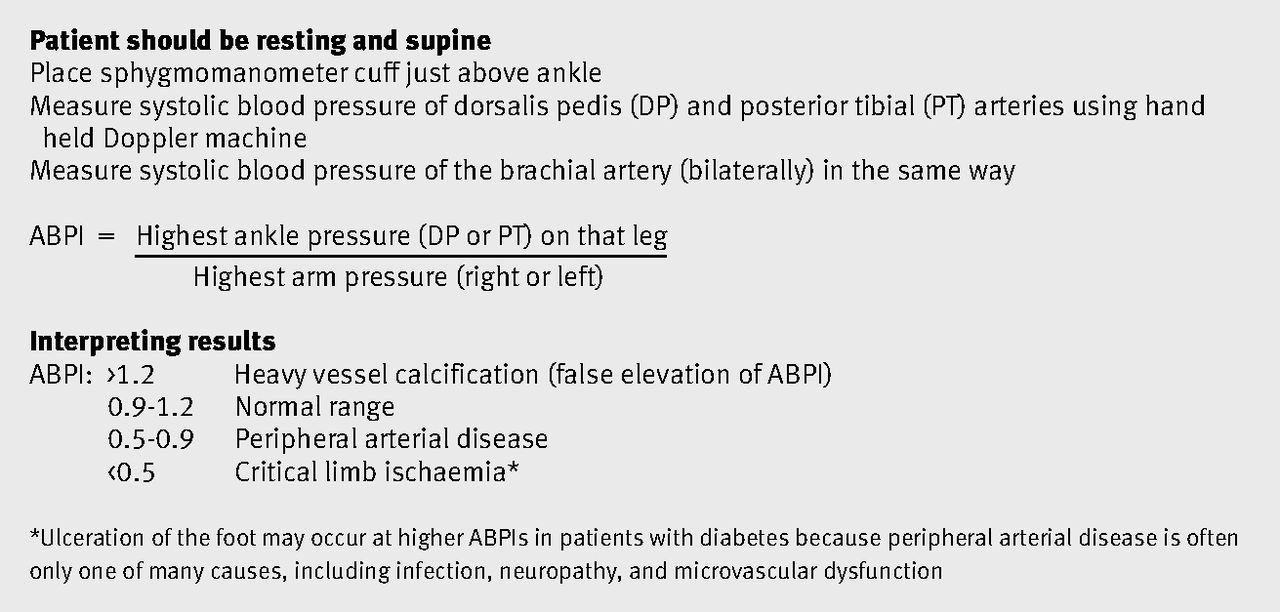
Fig 2 How to measure ankle brachial pressure index (ABPI)
{kind=link}
Several conditions can present with symptoms similar to those of PAD (box 1). Disease of the lumbar spine is perhaps the most common of these (causing spinal claudication) and can be distinguished from PAD by the presence of weakness as well as pain on walking. Straight leg raise may also reproduce symptoms in these patients.
Box 1 Differential diagnosis
Non-vascular: common conditions
Pain relieved by lumbar flexion (sitting)
-
Degenerative lumbar spine disease
-
Spinal canal stenosis (often associated with leg weakness)
-
Lumbar nerve root irritation (may be exacerbated by straight leg raise)
Pain elicited on joint examination
-
Osteoarthritis of hip or knee
Vascular (non-atherosclerotic): rare conditions
-
Athletic patients: popliteal artery entrapment; iliac artery endofibrosis
-
Male heavy smokers: Buerger’s disease (thromboangiitis obliterans)
-
Young patients with no other risk factors: cystic adventitial disease
-
Painful or pulsatile mass in buttock(s): persistent sciatic artery
Which patients should be referred to a vascular surgeon?
Consider routine referral for all patients with intermittent claudication, particularly if the diagnosis is uncertain. Although most patients will be managed without revascularisation, expert assessment can identify those who may benefit from intervention.
Refer patients with signs of tissue loss or sudden onset or deterioration of symptoms for urgent evaluation. NICE guidance recommends that patients with diabetes who present with foot ulceration of new onset should be seen in a multidisciplinary diabetic foot clinic within 24 hours of presentation, because such ulcers can rapidly progress to severe infection and amputation.15
The only patients for whom referral may be unnecessary are those with suspected PAD but only mild claudication that does not affect their quality of life (because such patients would not warrant revascularisation).
How are patients assessed further?
Specialist centres may supplement measurement of the resting ankle brachial pressure index with measurement of the toe-brachial pressure index, transcutaneous oxygen assessment, or exercise testing. Many patients will not require formal imaging once the diagnosis is established, because detailed characterisation of stenosis or occlusion is of little benefit unless revascularisation is planned. When imaging is necessary, duplex ultrasound is the first line modality, because it is non-invasive, readily available, and has a sensitivity of 84-87% and a specificity of 92-98% compared with angiography.20
Digital subtraction angiography was traditionally considered the “gold standard” for detailed evaluation of the arteries in PAD. However, it has largely been superseded by computed tomography angiography (fig 3⇓) and magnetic resonance angiography because of their high sensitivity and specificity and non-invasive nature. The role of digital subtraction angiography is now mainly in endovascular intervention.

Fig 3 Digital subtraction angiography images taken (A) before and (B) after angioplasty of the left superficial femoral and popliteal arteries. Note the extensive collateral network typically seen in peripheral arterial disease
{kind=link}
How can PAD be managed in primary care?
All patients with suspected PAD should be screened for cardiovascular risk factors (box 2).
Box 2 Recommended blood tests
All patients
-
Random serum glucose (to exclude occult diabetes)
-
Glycated haemoglobin (to assess glycaemic control in patients with diabetes)
-
Full blood count (to exclude polycythaemia, anaemia, and thrombocythaemia)
-
Serum urea and creatinine (to exclude renal dysfunction)
-
Serum cholesterol
Patients under 50 years of age
-
Thrombophilia screen
-
Serum homocysteine
Risk factor modification
Risk factors must be modified to reduce the risk of life threatening cardiovascular events and prevent progression of PAD.5 Targets for managing these risk factors are now included in the UK Quality and Outcomes Framework and NICE guidelines.21 22
Smoking cessation is extremely important and hypercholesterolaemia and hypertension should be treated aggressively according to national guidelines.21 22 Patients with a body mass index greater than 25 should also be encouraged to lose weight and take regular exercise. Subgroup analysis of the large Heart Outcomes Prevention Evaluation study suggested that angiotensin converting enzyme inhibitors may significantly reduce the risk of cardiovascular events in patients with PAD, and these are generally recommended as first line treatment for hypertension.23 However, they should be carefully monitored because more than 25% of patients with PAD have coexistent renal artery stenosis.5 A meta-analysis of 11 randomised controlled trials has shown that β blockers are not only safe for use in patients with PAD, but may also reduce perioperative cardiovascular events in those who need surgery.5 24
Patients should receive an antiplatelet agent to prevent progression of PAD and reduce overall cardiovascular risk. A subgroup analysis from the CAPRIE study (a large randomised controlled trial of 19 185 patients with all forms of cardiovascular disease) found clopidogrel to be more effective than aspirin, with a relative risk reduction of 8.7% for myocardial infarction, stroke, and vascular death.25 Because it has a preferable safety profile to aspirin and is now of comparable cost in the United Kingdom, clopidogrel is recommended by NICE as first line antiplatelet agent for patients with PAD.21 26
Concurrent use of more than one antiplatelet agent is generally not recommended for patients with simple PAD, but it may be useful for those who have had prosthetic bypass grafts.27 The use of warfarin is not routinely advised for patients with PAD unless they have a separate indication for its use.28
Management of claudication symptoms
Exercise
A Cochrane review of 22 studies of 1200 patients concluded that exercise regimens with at least two sessions of exercise a week can improve walking distance by 50-200% in patients with claudication.29 A separate Cochrane meta-analysis confirmed that carefully structured exercise programmes confer greatest benefit, with those in supervised programmes showing 30-35% greater improvement in walking distance after three months.w2 NICE therefore recommends that all patients with intermittent claudication are offered a supervised exercise programme.21
Vasoactive drugs
Two drugs are currently available in the UK for the treatment of intermittent claudication: cilostazol and naftidrofuryl oxalate. A meta-analysis of 26 studies assessing the efficacy of these drugs found that both offer modest improvement in walking distance with minimal adverse effects. However, there is little follow-up data beyond six months and cost effectiveness remains questionable.w3 As a result, the new NICE guidelines recommend only naftidrofuryl for use in patients with PAD and suggest that it be reserved for those who have failed to improve with structured exercise programmes and do not wish to be referred for angioplasty or surgery. Treatment with naftidrofuryl can be started in primary care, but its use should be reviewed after three to six months and discontinued if symptoms have not improved.21
Although antiplatelet agents and vasodilators (such as nifedipine) may be useful for reducing overall cardiovascular risk, there is little evidence that these drugs offer any benefit in treating the symptoms of claudication.
What are the principles of further management?
Intervention should be considered when conservative measures have failed and PAD is severely affecting a patient’s lifestyle or becoming limb threatening. Intervention may be endovascular (angioplasty or stenting) or surgical. Although endovascular treatment was originally reserved for short focal stenoses, advances in equipment and technique mean that an increasing proportion of lesions can be treated in this way.
Intervention for intermittent claudication
In patients with intermittent claudication, disease is often limited to a single arterial segment that may be suitable for angioplasty or stenting (fig 4⇓). Patients with focal iliac disease are more likely to be offered endovascular treatment than those with femoral disease, because intervention at the iliac level offers more durable results. Meta-analysis has shown that five year patency is 79% after iliac angioplasty and 55% after femoral angioplasty.30 31 However, there is some evidence that structured exercise programmes may improve walking distance as effectively as angioplasty.32w4
Surgical bypass is generally reserved for patients with debilitating claudication and a pattern of disease that is not amenable to angioplasty.

Fig 4 Computed tomography angiograms showing (A) normal lower limb vasculature and (B) heavily diseased arteries with previous left femoral anterior tibial bypass
{kind=link}
Intervention for critical limb ischaemia
Patients with critical limb ischaemia typically have multilevel disease and surgical bypass is often more appropriate, although endovascular techniques are increasingly being used as adjuncts to improve flow in the vessels proximal or distal to the bypass. Furthermore, emerging technologies such as drug eluting balloons and stents may improve the efficacy of endovascular techniques.
Trans-Atlantic Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II) guidelines currently recommend that patients with diffuse aortoiliac disease be treated with surgical bypass (unless other factors such as comorbidity prevent this), and five year patency of aortobifemoral bypass grafts is greater than 85% in those with critical limb ischaemia.5 33
Although few studies have directly compared angioplasty and surgical bypass, the large UK Bypass versus Angioplasty in Severe Ischaemia of the Leg trial compared outcomes in 452 patients with femoropopliteal disease and severe limb ischaemia.34 This study found no difference between angioplasty and bypass in terms of amputation-free survival, all cause mortality, or quality of life at two years, although the angioplasty group had significantly higher rates of reintervention (28% v 17%; 11% difference, 95% confidence interval 4% to 19%) and many ultimately needed surgery. Further subgroup analysis suggested that surgery may be preferable for fit patients. Vein tissue is used for bypass surgery whenever possible, because primary patency rates at five years are far higher than with prosthetic grafts (70% v 20% for femorodistal bypass).5
There is now some evidence that angioplasty alone may be beneficial for patients with critical limb ischaemia and infrainguinal disease who are unfit for surgical bypass. Although long term patency results are poor, short term improvements in distal perfusion may be sufficient to allow ulcer healing.w5
When revascularisation is unlikely to be successful or if patients have comorbidities that might prevent them making use of a salvageable limb, primary amputation may offer the best quality of life.w5 The knee joint is preserved whenever possible for the sake of mobility, although this must be balanced with the need to ensure wound healing.
What are the non-surgical treatment options for critical limb ischaemia?
Non-surgical treatments such as prostanoids (for example, iloprost), spinal cord stimulation, and lumbar sympathectomy are generally thought to have little long term benefit, so management of symptoms and amputation as appropriate are recommended for patients who are unsuitable for revascularisation.
Tips for non-specialists
-
Disease of the lumbar spine may cause symptoms that are similar to those of peripheral arterial disease
-
Always refer young patients with claudication to a specialist because they may have non-atherosclerotic vascular disease (for example, popliteal entrapment syndrome or iliac endofibrosis)
-
Some patients with claudication who fail to improve with conservative measures may benefit from angioplasty
-
Most patients with critical limb ischaemia are treated with surgical bypass, but the use of angioplasty is increasing
-
Foot ulceration has multiple causes in patients with diabetes and these patients should be seen by a multidisciplinary diabetic foot team within 24 hours
-
Ankle brachial pressure index <0.9 is associated with a threefold to sixfold increase in death from cardiovascular disease
Ongoing research and future directions
-
Drug eluting balloons and stents may prove to be superior to bare metal stents in the treatment of peripheral arterial disease, particularly in the infrapopliteal vessels, where restenosis rates are high.w6 However, these devices are expensive and with little evidence of clinical advantage to date, further trials are needed
-
Several very small studies have shown that injecting angiogenic growth factors into the gastrocnemius muscle may stimulate angiogenesis, inducing the growth of new blood vessels and reducing claudication and tissue loss.w7 However, much work is needed before such treatments become available for routine clinical use
Additional educational resources
Resources for healthcare professionals
-
National Institute for Health and Clinical Excellence. Lower limb peripheral artery disease: guideline. 2012. www.nice.org.uk/guidance/index.jsp?action=download&o=58408
-
Inter-Society Consensus for the Management of Peripheral Arterial Disease. www.tasc-2-pad.org/Client/EN/index.aspx?Composant=SSRubrique&IDBase=571&Methode=ClientFDetail&Ref=Downloadfulltextguidelines. Full detailed guidelines on the management of peripheral arterial disease and critical limb ischaemia
-
Schaper NC, Andros G, Apelqvist J, Bakker K, Lammer J, Lepäntalo M, et al. Specific guidelines for the diagnosis and treatment of peripheral arterial disease in a patient with diabetes and ulceration of the foot 2011. Diabetes Metab Res Rev 2012;28:236-7
-
International Working Group on the Diabetic Foot (www.iwgdf.org/)—Information on the care of patients with diabetes related foot disease
Resources for patients
-
Circulation Foundation (www.circulationfoundation.org.uk/help-advice/peripheral-arterial/)—Provides a summary of symptoms, investigations, and management of peripheral arterial disease
-
NHS Choice (www.nhs.uk/conditions/peripheralarterialdisease/Pages/Introduction.aspx)—Information and video explanation of peripheral arterial disease
Notes
Cite this as: BMJ 2012;345:e5208
Related links
bmj.com/archive
Previous articles in this series
Footnotes
-
Contributors: Contributors: GP and MG reviewed the literature and wrote the initial draft. KGJ, MMT, and RJH edited the manuscript. RJH is guarantor.
-
Funding: No special funding received.
-
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
-
Provenance and peer review: Not commissioned; externally peer reviewed.