Article Text

Abstract
Background: In primary cutaneous melanoma, the sentinel node (SN) biopsy is an accurate method for the staging of the lymph nodes. Positron emission tomography (PET) has been suggested as a useful alternative. However, the sensitivity of PET may be too low to detect SN metastases, which are often small.
Aim: To predict the value of PET for initial lymph node staging in melanoma based on morphometric analysis of SN metastatic load, without exposing patients to PET.
Material and methods: In 59 SN positive patients with melanoma, the sizes of tumour deposits in the SNs and subsequent dissection specimens were measured by morphometry and correlated with the detection limits of current and future PET scanners.
Results: The median tumour volume within the basin was 0.15 mm3 (range, 0.0001–118.86). Seventy per cent of these deposits were smaller than 1 mm3. State of the art PET scanners that have a resolution of about 5 mm would detect only 15–49% of positive basins. Logistic regression analysis revealed no pretest indicators identifying patients expected to have a positive PET. However, the SN tumour load was a significant and single predictor of the presence of PET detectable residual tumour.
Conclusion: Morphometric analysis of metastatic load predicts that PET scanning is unable to detect most metastatic deposits in sentinel lymph nodes of patients with melanoma because the metastases are often small. Therefore, the SN biopsy remains the preferred method for initial regional staging.
- positron emission tomography
- 18F-fluorodeoxyglucose
- melanoma
- staging
- lymph nodes
- sentinel node
- FDG, 18F-fluorodeoxyglucose
- H&E, haematoxylin and eosin
- LN, locoregional lymph node
- LND, lymph node dissection
- PET, positron emission tomography
- SN, sentinel node
Statistics from Altmetric.com
- FDG, 18F-fluorodeoxyglucose
- H&E, haematoxylin and eosin
- LN, locoregional lymph node
- LND, lymph node dissection
- PET, positron emission tomography
- SN, sentinel node
Determining the metastatic spread of tumour cells to the regional lymph nodes is essential in the assessment of prognosis and treatment options in patients with primary cutaneous melanoma. The sentinel node (SN) biopsy is currently the standard method for initial regional staging and has replaced the elective lymph node dissection.1 The SN is the first tumour draining lymph node that is surgically removed at the time of wide local excision of the primary melanoma. When the SN is tumour positive, a complete regional lymph node dissection (LND) is performed, but when the SN is negative, further regional lymph nodes should be negative in theory, and can therefore be left in situ.2–6
Positron emission tomography (PET) is a relatively new diagnostic imaging modality that allows the characterisation of disease based on altered metabolism rather than on the presence of structural abnormality. Accordingly, it differs fundamentally from most conventional imaging modalities, such as x ray films, computed tomography, and magnetic resonance imaging. In contrast, whole body PET can detect malignancy in normal sized lymph nodes and examines all organ systems in a single procedure.7–9 Images are obtained from positron emitting radioactive tracers that are administered intravenously. In oncology, 18F-fluorodeoxyglucose (FDG) is most frequently used because of the enhanced glucose consumption by tumours.10 The avidity of FDG for melanoma cells and the superior sensitivity of PET scanners led to the suggestion that FDG-PET might be used for initial non-invasive locoregional staging in breast cancer11 and cutaneous melanoma.12–15 One PET study claimed that micrometastases in SNs can be detected by PET before surgery.15 However, in breast cancer, this has already been questioned.16 Accurate assessment by PET of locoregional lymph nodes (LNs) would have great advantages: in LN positive patients, one could perform a primary lymph node dissection and avoid the SN procedure. The amount of (residual) tumour and the response to treatment are of importance when systemic treatment is considered. Such information would be very important because it could save unnecessary patient suffering and high costs, and could provide essential prognostic information for therapeutic decision making.
“Positron emission tomography is a relatively new diagnostic imaging modality that allows the characterisation of disease based on altered metabolism rather than on the presence of structural abnormality”
Even though it has convincingly been shown that PET detects tumour deposits smaller than the 1 cm limit of the computed tomography scan,17 the detectability rapidly decreases below the system resolution (typically 5 mm for a state of the art scanner). Therefore, we have analysed the size of metastatic lymph node deposits in histological sections by morphometry, and compared these with PET resolution. We also investigated whether future PET scanning machines will ever be able to detect micrometastases, given the detection limits that can be anticipated.
PATIENTS AND METHODS
Patients
Data were analysed from a cohort of 308 consecutive patients undergoing SN mapping in biopsy confirmed primary cutaneous melanoma between September 1993 and January 1999. The patient group consisted of 135 men and 173 women aged 18 to 85 years (mean, 48). SN mapping was performed by a triple technique, including lymphoscintigraphy followed by blue dye and γ probe guided surgery.18 In our hospital, a complete LND of the regional basin is performed in the case of a tumour positive SN. Patients were screened for distant metastases but none were found, so that LNDs were carried out in all but two SN positive patients who refused to agree to the procedure. Within one year after the initial investigations, recurrences were diagnosed by the finding of distant metastases in one patient within six months, and in another four patients in the remaining period.
Pathology
Lymph nodes were fixed in neutral buffered formaldehyde. SNs smaller than 0.5 cm were processed and paraffin wax embedded intact, those between 0.5 and 1 cm were halved, and SNs larger than 1 cm were lamellated into approximately 0.5 cm pieces.19,20 All SN blocks were step sectioned at five levels with 250 μm intervals. On each level, sections were stained with haematoxylin and eosin (H&E) and by immunohistochemistry (S100 and HMB-45 antibodies). Lymph nodes in LND specimens were analysed in a routine fashion, meaning that one H&E stained section was made for each block, so that depending on the size of the lymph node one to three sections were obtained from each non-SN.
The size of the metastases was determined using an interactive video overlay system (Q-PRODITR; Leica, Cambridge, UK). The surface areas of individual tumour deposits were measured and the total tumour area was calculated for each node. Because tumour deposits are usually spherical, surface areas were converted to diameter (mm) and volume (mm3), as follows: diameter (d) = 2/(tumour area/π) and volume = 4/3π(d/2)3. The total tumour volume for each nodal basin was calculated by summing up the volumes of tumour in all positive SN(s) and non-SN(s) in that basin.
It has been estimated that with a single central cross section and immunostaining, 69% of metastases are found, as opposed to 81% in the 10 step procedure used in SNs of 1 cm.21 In addition, with a limited number of slices, as used in non-SNs, the slice may not contain the maximum diameter: assuming that the section level is random, the average measured diameter in the case of a single section will be 8.7 mm (in the middle between the maximum and minimum diameter) in a spherical metastasis of 1 cm. In volume terms, this implies a potential average underestimation of 34%. Combined with the hit probability of 69%, this yields a mean potential underestimation of the real tumour volume by 50% (0.69* (1.0 − 0.34)) in non-SNs.
Statistical analysis
Logistic regression analysis was used to predict the usefulness of PET: (1) at initial regional staging and (2) after a tumour positive SN biopsy to identify patients with additionally involved regional lymph nodes. In the first situation, we studied whether the established prognostic variables—age, sex, Breslow thickness, and melanoma localisation—could predict the presence of a PET detectable amount of tumour. In the second situation, the feature “tumour volume in the SN” was added to this set of variables. In both situations, a range of PET detection limits was taken into account (2–10 mm). The significance of the correlations was evaluated by Pearson’s test. Tumour volumes in SNs and non-SNs were compared with the Wilcoxon signed ranks test. Significance was set at 0.05.
RESULTS
Of 308 patients, 59 (19%) had a tumour positive SN (table 1). SN positivity increased with Breslow thickness (table 1). In addition, the amount of tumour in the SN was significantly related to Breslow thickness (Pearson’s correlation coefficient = 0.397; p = 0.002). Thirteen SN positive patients had positive non-SNs, as shown by histological examination of 57 LND specimens and by (uneventful) follow up (at least two years) in two patients who refused LND. A weak positive correlation was found between the total amount of tumour in the regional basin and the Breslow thickness of the primary tumour (Pearson’s correlation coefficient = 0.286; p = 0.028). Table 1 shows that the average size of tumour deposits in SNs is extremely small, even in patients with Breslow thickness > 4.0 mm.
Tumour volumetry of regional lymph nodes in 59 patients with cutaneous melanoma in relation to Breslow thickness and sentinel node status
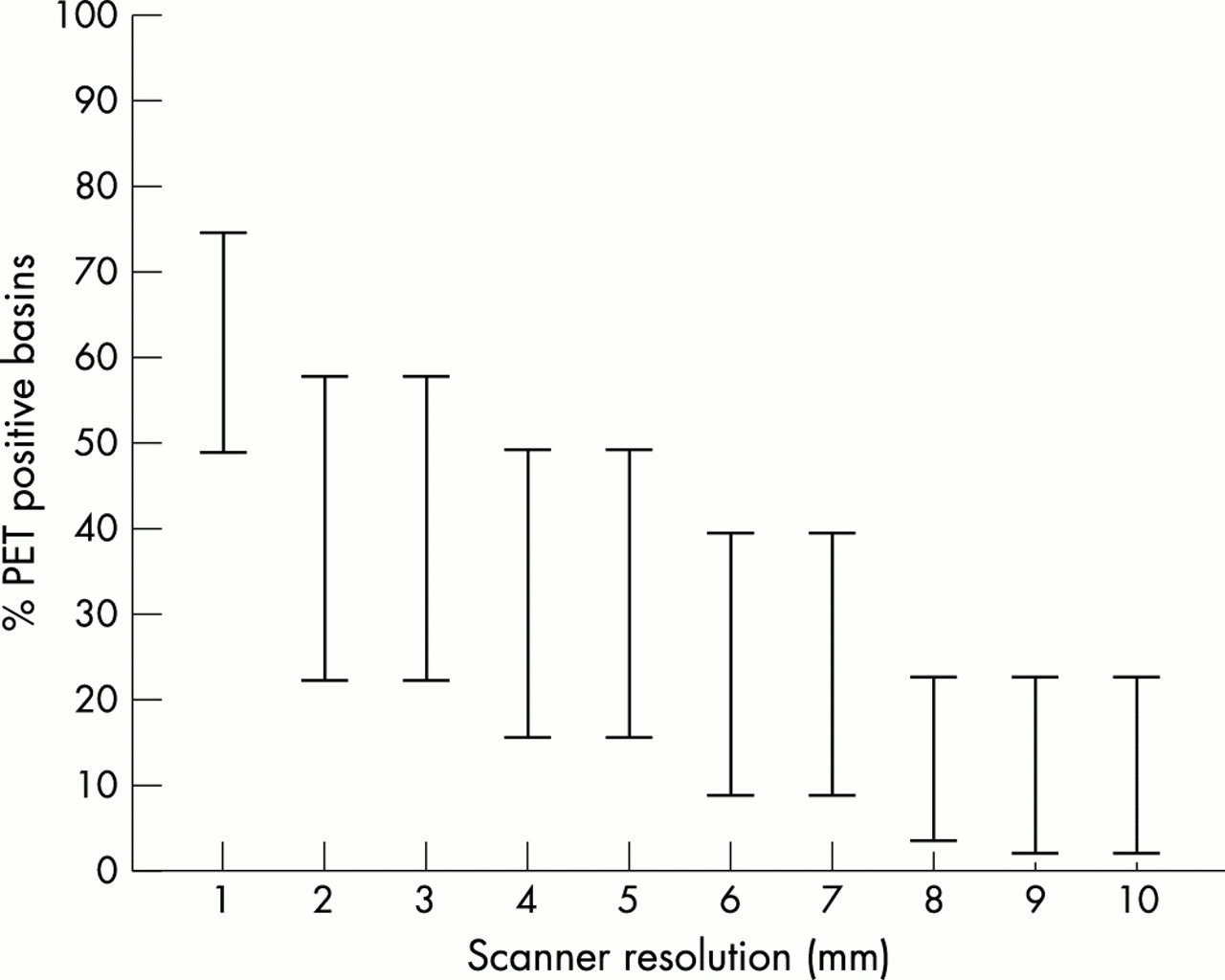
For a state of the art PET scanner the detection rate for metastases positive lymph nodes would be between 15% and 49% only. Figure 1 shows the predicted yield of scanners with alternative resolution parameters (see also appendix 1).
{kind=link}
The predicted yield of 18F-fluorodeoxyglucose positron emission tomography (PET) scanners with different resolutions (1–10 mm), using the histopathological data from 59 patients with cutaneous melanoma and lymph node involvement. For each resolution, the percentage of PET positive tumour basins is expressed as a detection range corresponding to published target to background ratios of 1.5–10 (appendix 1).12
With logistic regression analysis, we found that no established preoperative diagnostic indicator (age, sex, Breslow thickness, site of the primary melanoma) could predict PET positivity at any presumed detection limit. However, if the SN biopsy information (the tumour volume in the SN) was included, the amount of tumour in the SN was the only significant predictor for the presence of PET detectable tumour in non-SNs, but only at detection limits of < 65.4 mm3. It is predicted that at the 14.1 mm3 (3 mm) detection limit (p = 0.006), PET will miss more than 29% of the positive lymph nodes in patients with SN tumour volumes exceeding 19 mm3.
DISCUSSION
Our present morphometric study shows that the average total size of metastatic deposits in regional lymph node basins of patients with cutaneous melanoma is quite small. Within a broad range of detection limits for FDG-PET, most of these deposits remain undetectable. Earlier claims that PET would be of value12–15 have therefore been too optimistic.22 Large patient studies to validate this conclusion in the clinical setting would result in unnecessary costs. Such studies may only be useful in a specific subset of patients—for example, those with a large (> 19 mm3) tumour load in the SN.
This is the first study using histomorphometric data to predict the usefulness of a new imaging technique for a certain indication. Instead of performing a traditional accuracy study, we first assessed what could be expected from FDG-PET. Our method provides a clear answer to this question and makes further patient studies superfluous, which could save much unnecessary cost. In addition, this method is probably useful in other cancers with predictable lymphatic spread, such as breast cancer, where similar optimistic expectations of PET sensitivity have been postulated,11 but which have also been challenged.16
The use of a “cumulative tumour volume” in separate lymph nodes to represent the total tumour burden in the basin obviously leads to some overestimation of PET sensitivity. On the other hand, PET sensitivity may be underestimated because of tissue shrinkage during fixation leading to reduced volume measurements, and the fact that histopathology does not identify 100% of tumour deposits,23 as explained in the Methods section. However, we have tried to correct for this as much as possible. A further refinement could have been to use a sphere model approach instead of assuming that the metastases are round, but it is unlikely that this would have influenced the final results. Overall, we feel that our approach has resulted in realistic tumour volume assessments and resulting PET sensitivity estimations allowing a clear conclusion.
“The average total size of metastatic deposits in regional lymph node basins of patients with cutaneous melanoma is quite small”
Our prediction of the value of PET for initial regional staging (fig 1) is in agreement with in vivo data of four studies.24–27 The results of the study by Crippa et al,24 in which 23% of the nodal metastases < 5 mm were detected by PET, are comparable because in our database 95% of the tumour diameters were < 5 mm.
The SN status appears to be the most important prognostic factor for recurrence,28 and the best method to select patients with melanoma for adjuvant trials.29–31 Because FDG-PET is an established method to monitor the early response to systemic treatment, PET could then provide a tool to identify subclinical tumours and to monitor their response to treatment in this specific subset of SN positive patients. In our opinion, the next step should be to study this specific subset of SN positive patients and to perform LND regardless of the PET results.
Take home messages
-
The morphometric analysis of metastatic load predicts that positron emission tomography scanning cannot detect most metastatic deposits in the sentinel lymph nodes of patients with melanoma because the metastases are usually too small
-
The sentinel node biopsy is therefore still the preferred method for initial regional staging in melanoma
PET scanning is unable to detect small metastatic deposits in SNs of patients with primary melanoma. FDG-PET cannot replace the SN biopsy, which is still the preferred method for initial regional staging.
We conclude that morphometric analysis of metastatic load predicts that PET scanning is unable to detect most metastatic deposits in the sentinel and regional lymph nodes of patients with cutaneous melanoma because these metastases are often small. Therefore, the SN biopsy remains the preferred method for initial regional staging. Thus, PET studies where patients are scanned for this indication are superfluous.
APPENDIX 1 LESION DETECTABILITY IN EMISSION TOMOGRAPHY
Detectability is a function of resolution and contrast. According to standard principles, at a 5 mm system resolution (R), maximally 50% of the activity (emitted counts) from a lesion of 5 mm diameter (D) will be registered because recovery (the ratio between registered and emitted counts) is as follows: 1 − exp[−ln2*(D/R)2].32 For various target to background (T/B) ratios, the contrast resulting from this ratio and the resolution of the imaging system can be determined because contrast = 1 + (T/B − 1)* recovery. In our model, we used an empirically determined contrast of 1.1 as minimally required for detection. Using the morphometric data, the expected prevalence of FDG positive sites can then be predicted using the reported in vivo target to background ratios for extrathoracic and abdominal melanoma deposits (2–1012) and the 5 mm resolution typical of the present generation of PET scanners.