Article Text

Abstract
Objective To investigate the value of iodine-123 meta-iodobenzylguanidine (MIBG) myocardial imaging for defining high risk patients with idiopathic dilated cardiomyopathy from among candidates for β blocker treatment, and for predicting functional improvement of the left ventricle in the early stages of treatment.
Methods Echocardiographic indices, neurohormonal measurements, and myocardial MIBG distribution were assessed at baseline and after one month and three months of treatment in 27 patients with idiopathic dilated cardiomyopathy. Patients were classified into two groups, based on whether they reached a daily dose of > 20 mg of metoprolol without deterioration of heart failure at three months (group A, n = 20) or not (group B, n = 7).
Results There were no significant differences in the echocardiographic indices or neurohormonal activity at baseline between the two groups, but MIBG uptake was higher, and the washout rate lower, in group A than in group B. After one month, though there were no significant changes in echocardiographic and neurohormonal variables, the heart to mediastinal (H/M) ratio on the delayed image was increased in group A but not in group B. In group A, the degree of increase in the H/M ratio on the delayed image after one month was also correlated with the degree of reduction in plasma concentrations of noradrenaline after three months.
Conclusions MIBG myocardial imaging may be useful for predicting the outcome of β blocker treatment for heart failure patients with idiopathic dilated cardiomyopathy.
- dilated cardiomyopathy
- β blockers
- MIBG
Statistics from Altmetric.com
In 1975, Waagstein et al reported that a very low initial dose of the β adrenergic receptor blocker, metoprolol, which was then slowly increased, produced clinical improvement in patients with severe heart failure from idiopathic dilated cardiomyopathy.1 Following this first report, β blockers have been found to improve symptoms, cardiac function, and prognosis in a proportion of patients with heart failure from various causes.2-6 However, it is necessary to predict the likely effectiveness of the β blocker treatment before starting it, because β blockade has negative inotropic effects and is recognised to be a two edged sword for patients with heart failure. Although two recent studies have suggested that patients with a rapid heart rate at rest and at peak exercise will respond best to β blocker treatment,7 ,8 this criterion does not adequately distinguish high risk patients from candidates for the treatment. Thus it is still unclear what features can be used to predict the effectiveness of β blockade, either before treatment has been started or early in its course.
It has been reported that myocardial imaging with iodine-123 meta-iodobenzylguanidine (MIBG)—an analogue of noradrenaline—provides information on the severity of altered adrenergic innervation of the heart in patients with heart failure.9 Previous studies have shown the potential value of MIBG for assessing the pathophysiology of heart failure: increased clearance of MIBG from the heart is consistent with increased sympathetic nervous activity,9 and reduced MIBG uptake is related to poor prognosis.10 However, the clinical significance of myocardial MIBG imaging in relation to the treatment of heart failure has not been established.
In this study, we identified features of MIBG cardiac imaging that defined high risk patients from the candidates for β blocker treatment, and predicted improvement in echocardiographic and neurohormonal indices before treatment or early in its course, in a group of patients with idiopathic dilated cardiomyopathy.
Methods
PATIENT POPULATION
We studied 27 patients with dilated cardiomyopathy (mean age 52.2 years, range 23 to 73 years), who had experienced at least one episode of exacerbation of heart failure requiring short term hospital admission and who underwent baseline cross sectional echocardiography, left ventriculography, and coronary angiography between 1 October 1993 and 20 December 1996. All patients had a left ventricular ejection fraction of ⩽ 0.45 (mean 0.34, range 0.16 to 0.45), a systolic blood pressure > 90 mm Hg (mean 118, range 92 to 138), and a heart rate > 50 beats/min (mean 68, range 56 to 92) before study entry, and were in New York Heart Association (NYHA) functional class II to III; 21 were in class II and the remaining six were in class III. None of the patients had received β blocker treatment or β agonists within three months of study entry. No patient had significant coronary stenoses on coronary angiography (narrowing > 50% of the artery lumen). Patients who were on reserpine or tricyclic antidepressants, which are known to affect myocardial MIBG uptake, were excluded from the study. Otherwise drug treatment, which included oral digoxin, diuretics, or angiotensin converting enzyme (ACE) inhibitors, remained unchanged during the study period. Informed consent was obtained orally from all subjects.
CROSS SECTIONAL ECHOCARDIOGRAPHY
Cross sectional echocardiographic recordings of routine views were obtained with a Toshiba 160A or 270 machine using a 2.5 or 3.75 MHz transducer (Toshiba Co, Tokyo, Japan). The recordings were stored on a video recorder and analysed for evidence of organic valvar disease and left ventricular wall motion disturbances. The end diastolic and end systolic left ventricular dimensions and the calculated per cent fractional shortening (%FS) were determined according to the recommendations of the American Society of Echocardiography.11
NEUROHORMONAL MEASUREMENTS
Blood was drawn from the antecubital vein after the subject had been in a recumbent position for 30 minutes. The blood sample was placed in a prechilled tube containing sodium EDTA for the measurement of plasma noradrenaline and atrial natriuretic factor (ANF). The sample was centrifuged within one hour at 3000 ×gfor 12 minutes at 4°C. Plasma was stored at < −70°C. Plasma noradrenaline was measured by high performance liquid chromatography with electrochemical detection by a previously described method, with an interassay coefficient variability of 11%.12 The plasma concentration of ANF was measured using a specific radioimmunoassay for α-human ANF, as previously described.13
IMAGING PROTOCOL
MIBG cardiac imaging was performed at rest and in the fasting state, before, one month after, and three months after β blocker treatment was begun. A dose of 111 Mbq of commercially available MIBG (Daiichi Radioisotopes Laboratories, Tokyo, Japan) was given intravenously. Anterior planar images of the chest were acquired 15 minutes (initial imaging) and four hours (delayed imaging) after the tracer injection, using a large field gamma camera equipped with a low energy, all purpose, parallel hole collimator (Toshiba, GCA901A/HG). For comparing MIBG uptake by the heart between individuals, theheart to mediastinum (background) radioactivity ratio (H/M ratio) was determined by drawing regions of interest (ROI) around the left ventricular myocardium and in the upper mediastinum, and measuring the average count in each ROI ([H] and [M]) with an on-line minicomputer system (Toshiba GM5500).MIBG washout rate (WR; %) of the heart from the initial to delayed imaging was also calculated using the formula, {([H] − [M])initial − ([H] − [M])delayed} / {([H] − [M])initial}.
DRUG TITRATION
Metoprolol was initially given at a dose of 5 mg daily; the dose was then increased by 2.5 to 5 mg weekly up to a maximum of 40 mg/day. We measured left ventricular dimensions by echocardiography and assessed neurohormonal activity and MIBG myocardial distributions after one month (daily dose metoprolol 20 mg) and after three months of treatment.
STATISTICAL ANALYSIS
Results are given as mean (SD). Baseline variables were compared using Pearson’s χ2 test for discrete variables and the Mann–Whitney U test for continuous variables. Serial changes in the H/M ratio, neurohormonal factors, and echocardiographic variables in response to metoprolol treatment were compared by analysis of variance for repeated measures. As the distributions of the neurohormonal factors are certainly not normal, the data were logarithmically transformed before analysis. Linear regression analysis was used to determine the correlations between the H/M ratio and plasma noradrenaline. Probability (p) values less than 0.05 were considered significant.
Results
CLINICAL OUTCOME
All patients tolerated the initial 5 mg dose of metoprolol. However, one patient who was receiving 10 mg of metoprolol daily died of ventricular tachycardia, and six could not tolerate the drug at doses of ⩾ 20 mg/day. Patients were classified into two groups on the basis of whether they reached more than 20 mg of metoprolol without deterioration of heart failure at three months (group A, n = 20), or not (group B, n = 7). All patients in group A improved symptomatically at three months of treatment: those in NYHA class II (n= 17) improved to class I, and those in NYHA class III (n = 3) improved to class II. None of the patients in group B improved at three months; one in NYHA class III died (as mentioned above) and the remaining six (four in NYHA class II and two in class III), deteriorated on 15 to 20 mg of metoprolol. There were no significant differences between the groups in baseline characteristics, age, symptoms, or haemodynamic variables (table 1). There was no significant change in heart rate in either group during the study.
Patient characteristics at baseline
ECHOCARDIOGRAPHIC VARIABLES
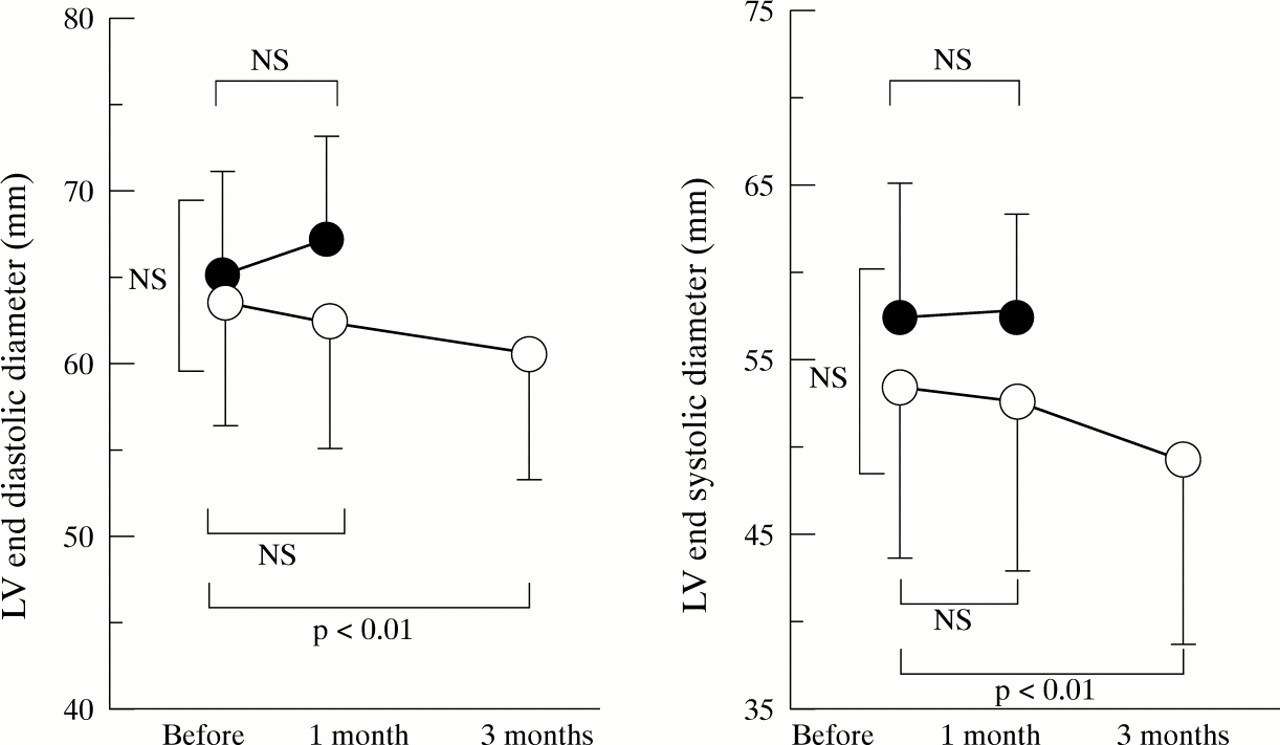
In group A, the left ventricular end diastolic dimension showed no significant change at one month (from 63.3 (7.8) to 62.5 (7.8) mm), but improved at three months, to 60.4 (7.4) mm (p < 0.01v baseline and the one month value; fig 1); left ventricular end systolic dimension showed no significant change at one month (from 52.2 (8.7) to 52.1 (9.1) mm) and improved at three months, to 47.4 (9.5) mm (p < 0.01 vbaseline and the one month value; fig 1). %FS showed no significant change at one month (from 17.2 (6.6) % to 18.6 (5.1) %), but again improved at three months, to 22.7 (6.4) % (p < 0.01v baseline and the one month value).

Echocardiographic findings in group A (empty circles) and group B (filled circles) before β blocker treatment and at one month and three months after starting treatment.
In group B, left ventricular end diastolic and end systolic dimensions and %FS showed no significant change during the course of the study.
NEUROHORMONAL DATA
In group A, plasma noradrenaline decreased at one month from 662 (463) to 492 (231) pg/ml (NS), and decreased significantly at three months, to 354 (151) pg/ml (p < 0.05 vbaseline; fig 2).
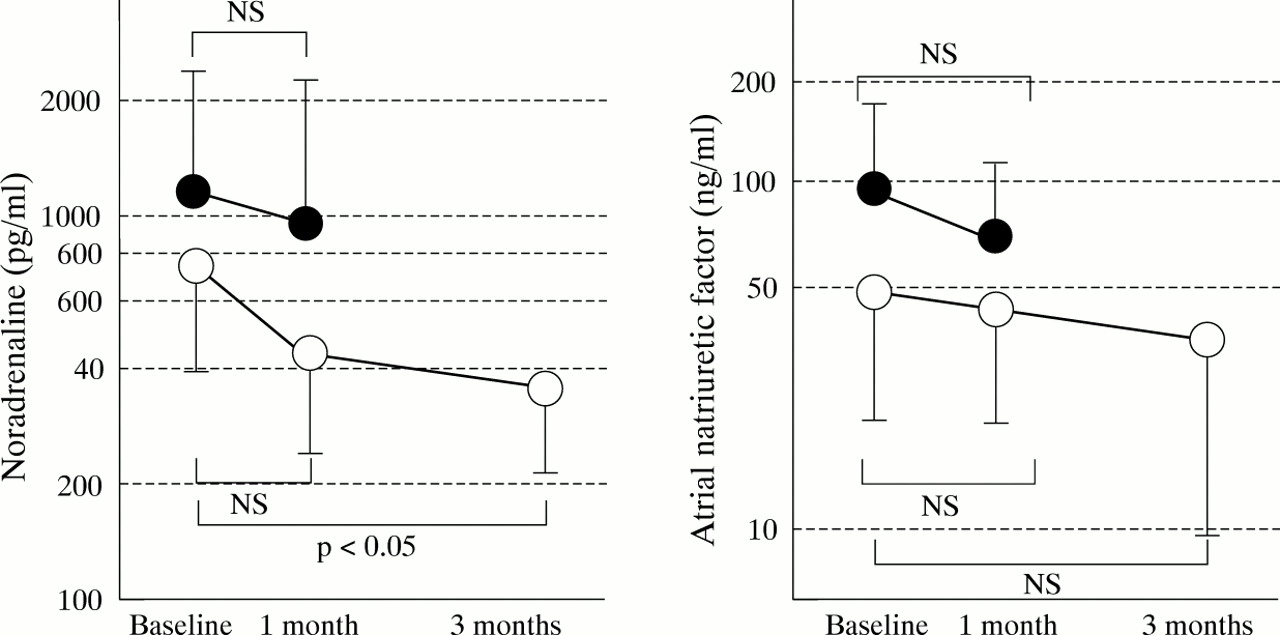
Neurohormonal factors of group A (empty circles) and group B (filled circles) before β blocker treatment and at one month and three months after starting treatment.
In group B, plasma noradrenaline at one month was the same as at baseline.
Plasma ANF tended to decrease at one month in both groups, but the decrease was not significant.
MYOCARDIAL MIBG CONCENTRATION
Baseline H/M ratios on the initial image (2.58 (0.38)v 1.85 (0.35), p < 0.01) and on the delayed image (2.33 (0.63) v 1.55 (0.34), p < 0.01) were higher, and the washout rate was lower (42.8 (11.5) % v 57.1 (14.3) %, p < 0.05) in group A than in group B (fig 3). No patients with baseline H/M ratios of < 2.0 on the initial image were observed in group A.
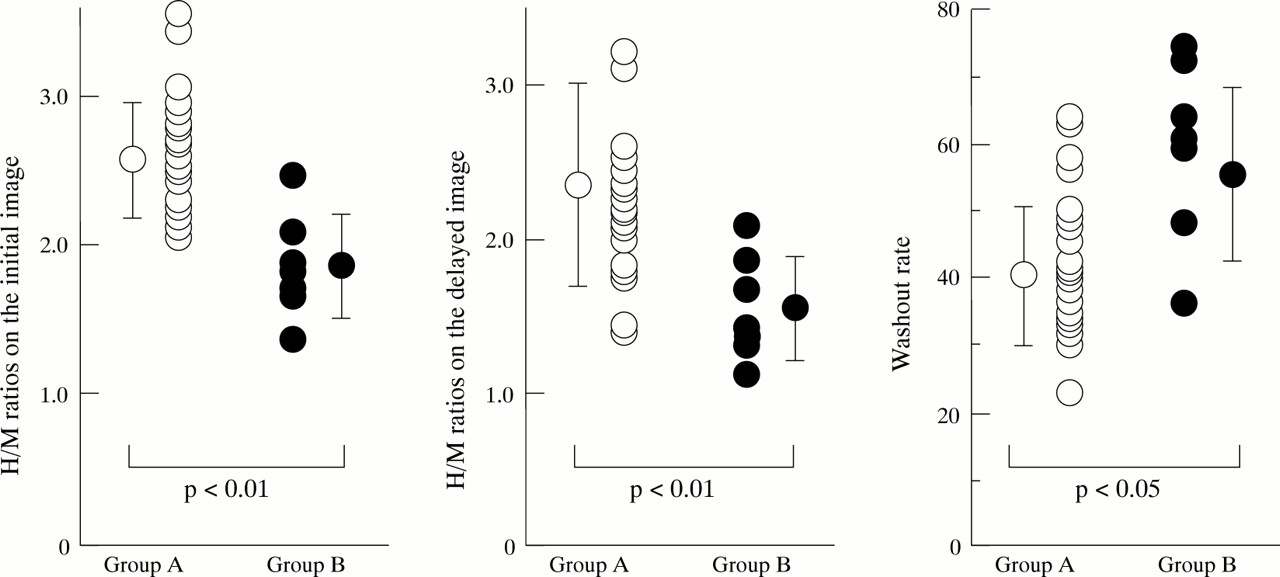
Baseline heart to mediastinal (H/M) ratios and washout rates in group A (empty circles) and group B (filled circles).
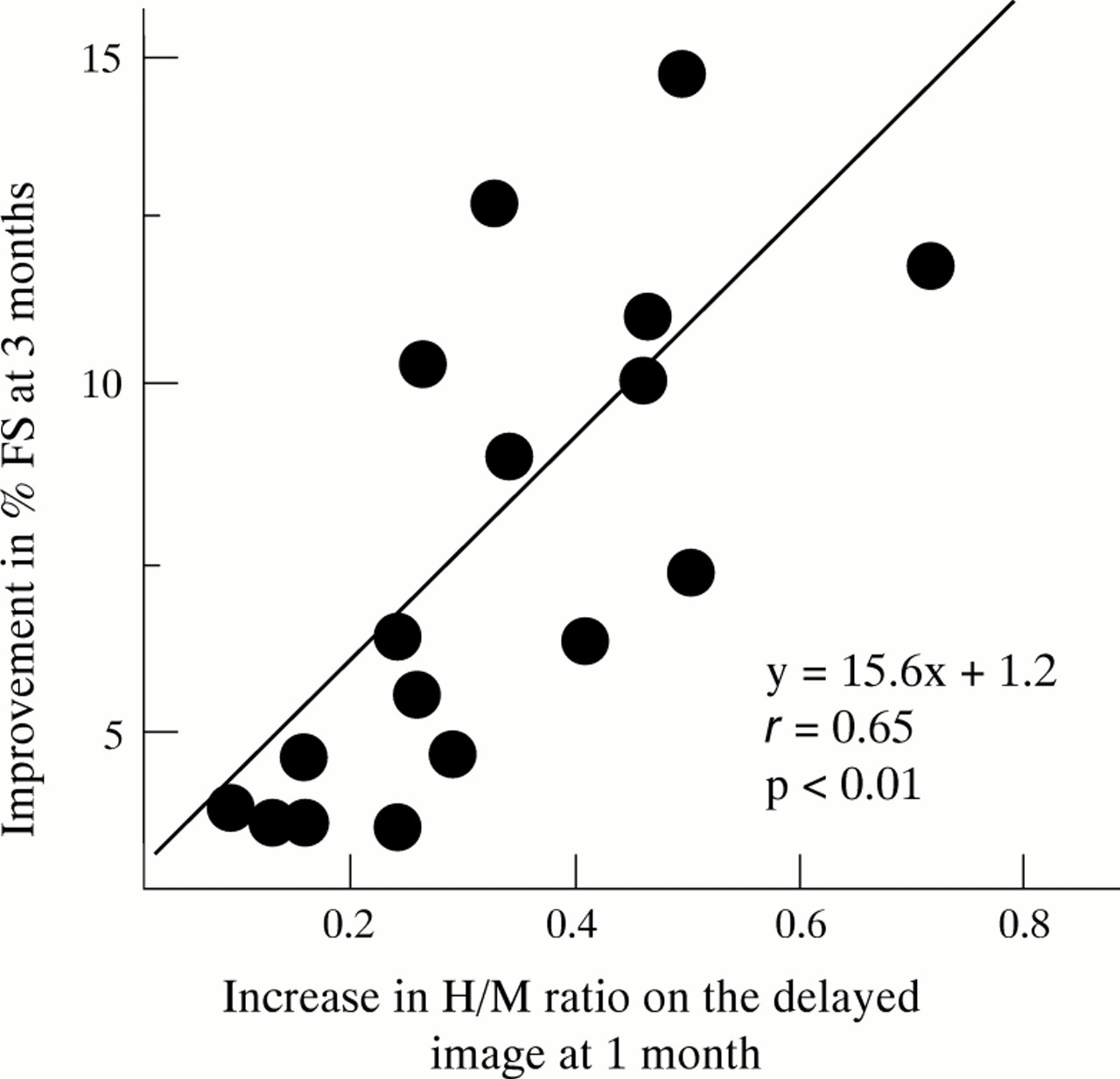
After one month of treatment, the H/M ratios on the initial image had not changed significantly in either group (group A, from 2.58 (0.38) to 2.60 (0.34); group B, from 1.85 (0.35) to 1.84 (0.28), n = 6). During the same period, the H/M ratio on the delayed image increased in group A (from 2.33 (0.63) to 2.50 (0.60), p < 0.01v baseline), but not in group B (from 1.55 (0.34) to 1.60 (0.28), n = 6, NS) (fig 4). The washout rate also tended to decrease in group A after one month of treatment (from 42.8 (11.5) to 41.7 (10.1), NS), but not in group B (from 57.1 (14.3) to 60.2 (10.4), n = 6, NS). The increase in the H/M ratio on the delayed image at one month correlated with the degree of improvement in %FS at three months (r = 0.65, p < 0.01; fig5).

Serial changes in heart to mediastinum (background) radioactivity ratio (H/M ratio) on MIBG scintigraphy. After one month of β blocker treatment, the H/M ratio on the delayed image was increased in group A (empty circles), but not in group B (filled circles). At three months, the H/M ratio on the delayed image showed further improvement in group A. The H/M ratio on the initial image did not change significantly in either group.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correlation between the degree of improvement in fractional shortening of the left ventricle (%FS) at three months of β blocker treatment and the improvement in the H/M ratios on the delayed image at one month of treatment in group A.
At three months, the H/M ratio on the delayed image in group A (2.65 (0.62); p < 0.01 v baseline and the one month value, fig 4) showed further improvement, though the H/M ratios on the initial image did not change significantly (2.68 (0.36), NSv baseline and the one month value).
Discussion
PREDICTION OF HIGH RISK PATIENTS FOR β BLOCKER TREATMENT
In this study, we found that the response to metoprolol was not related to baseline neurohormonal indices (noradrenaline, ANF), the size of the left ventricular chamber, or left ventricular fractional shortening in heart failure patients, in agreement with a previous report on the response to bisoprolol.14 This suggests that patients with a low fractional shortening and a large left ventricular end diastolic dimension, as determined by echocardiographic examination, did not necessarily deteriorate on β blocker treatment and should not therefore be excluded from receiving this treatment. We also showed that MIBG imaging was an excellent predictor of patients at high risk for β blockade: the H/M ratios on the initial and delayed images were low (1.85 (0.35), and 1.55 (0.34), respectively) and the washout rate was high (57.1 (14.3)%) in the high risk patients (group B) who showed poor progress on β blocker treatment. Heart failure patients with H/M ratios of < 2.0 on the initial image could not be expected to tolerate up to 20 mg of metoprolol.
Sympathetic abnormalities are assessed by MIBG imaging because MIBG is distributed to the sympathetic nerve terminals, where it shares uptake and storage mechanisms with noradrenaline.15 ,16 Schoferet al reported that the H/M ratio was significantly correlated with the myocardial content of noradrenaline,17 suggesting that a decrease in MIBG uptake is related to sympathetic dysfunction. Our results therefore suggest that heart failure patients with severe sympathetic dysfunction, in whom the H/M ratios on the initial MIBG image were decreased, were at high risk for β blocker treatment. Patients with a low MIBG uptake should be excluded from β blocker treatment and should be considered for other therapy (for example, heart transplantation).
REDUCTION IN LEFT VENTRICULAR DIMENSION AND H/M RATIO ON MIBG IMAGING
We observed that an improvement of impaired myocardial sympathetic nerve activity, as detected by the H/M ratio on the delayed MIBG image, preceded the improvement in left ventricular function after β blockade. Shelley et al reported that the left ventricular ejection fraction on day 1 of β blocker treatment was depressed but returned to baseline by one month and improved between one and three months in patients with congestive heart failure.5 This suggested that the initial mild depression of left ventricular function may have been caused by the negative inotropic properties of β blocker treatment, but that β blockers induced healing and caused improvement in myocyte function during the dose titration. In other words, when the improvement in myocyte function exceeds the negative inotropic effect of the β blocker, left ventricular function improves. Our results suggested that MIBG imaging can detect the stage of the healing and initial improvement before there is overt left ventricular functional improvement, which is not possible with echocardiographic or neurohormonal indices.
We also showed that the degree of the improvement in the H/M ratio on the delayed image at one month of treatment quantitatively predicted the degree of improvement in left ventricular function at three months of treatment. This suggests that monitoring MIBG imaging in the first month after starting treatment was helpful in predicting future improvement in left ventricular function.
In contrast to the improvement in the H/M ratio on the delayed MIBG image, the MIBG washout rate did not improve after one month of treatment. This suggests that improvement in the washout rate did not predict improvement in left ventricular function after β blocker treatment, although such treatment is known to diminish sympathetic hyperactivity at the nerve terminals, a feature that is normally well reflected in the MIBG washout rate. The reason for this discrepancy may be that, because left ventricular function was influenced not only by sympathetic hyperactivity at the nerve terminals but also by the damaged myocardium of the left ventricular wall, improvement in left ventricular function was not necessarily mirrored by improvement in sympathetic hyperactivity after β blocker treatment. The fact that the H/M ratio did not improve during the course of the study supports that hypothesis.
STUDY LIMITATIONS
This study has two main limitations. First, the quantification of myocardial MIBG activity on scintigraphic images presents technical limitations. The marked decrease in MIBG uptake in our patients with severe dilated cardiomyopathy created difficulties in image reconstruction. The ideal cardiac region of interest includes myocardial activity, but excludes adjacent lung and liver activities. Ventricular enlargement may lead to an underestimation of myocardial activity. It is difficult to determine the cardiac region of interest for these reasons. Second, the numbers of patients were small, so this can only be considered a pilot study. A further study involving a larger sample size should now be undertaken.
CONCLUSIONS
MIBG imaging predicts the response to β blocker treatment in patients with heart failure caused by idiopathic dilated cardiomyopathy. Thus monitoring of MIBG accumulation may be helpful in identifying the timing and degree of functional improvement when this treatment is given. MIBG imaging appears to be more sensitive than echocardiography or neurohormonal indices in assessing the effects of β blockade.
Acknowledgments
This study was supported by the Research Grant for Cardiovascular Diseases (8A-5) from the Ministry of Health and Welfare, Tokyo, Japan, in 1996 and 1997.