Article Text

Abstract
Objectives To further validate the diagnostic utility of 18F-AV-133 vesicular monoamine transporter type 2 (VMAT2) positron emission tomography (PET) in patients with clinically uncertain parkinsonian syndromes (CUPS) by comparison to clinical diagnosis at 3 years follow-up.
Design, setting and participants In a previous study, we reported that 18F-AV-133 PET in community patients with CUPS changed diagnosis and management and increased diagnostic confidence. The current diagnosis of this cohort was obtained from the patient and treating specialist and compared with the diagnosis suggested 3 years earlier by the 18F-AV-133 PET. A second 18F-AV-133 PET was available in those with a discordant or inconclusive final diagnosis.
Study outcome measures The primary end point was the proportion of patients who had a follow-up clinical diagnosis, which was concordant with their initial 18F-AV-133 PET scan. Secondary end points were the proportion of patients who had the same diagnosis at follow-up as that reached after the initial scan and the stability of diagnostic changes made after the first scan.
Results 81 of the 85 patients previously recruited to the CUPS study had follow-up of which 79 had a clinical diagnosis and 2 remained CUPS. The diagnosis was in agreement with the initial 18F-AV-133 PET scan result in 74 cases. Five patients had a discordant diagnosis; one patient with rubral tremor had a severely abnormal scan that had worsened when rescanned; four cases with normal initial and repeat scans had a clinical diagnosis of Parkinson’s disease. Two patients with suspected genetic disorders remained classified as CUPS and both had normal scans. In the 24 CUPS cohort patients where 18F-AV-133 PET initially changed diagnosis, this change was supported by follow-up diagnosis in all but the one rubral tremor case.
Conclusion 18F-AV-133 PET is a useful tool in improving diagnostic accuracy in CUPS providing results and diagnostic changes that remain robust after 3 years follow-up.
- diagnostic accuracy
- molecular imaging
- parkinson-s disease
- pet
- vmat2
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is a 3-year follow-up study evaluating the current clinical diagnosis of patients with clinically uncertain parkinsonian syndromes (CUPS), who have previously had a 18F-AV-133 positron emission tomography (PET).
The aim of the study is to evaluate the diagnostic accuracy and validate the optimal binding reduction threshold of 50% for abnormal scans.
The final diagnosis was nominated by the treating specialist and patient after a period of clinical follow-up.
The follow-up clinical diagnosis was compared with the diagnosis suggested by the 18F-AV-133 PET and the initial clinical diagnosis reached after the scan.
A repeat 18F-AV-133 PET was reviewed in patients who had a current clinical diagnosis that was discordant with the scan result or those with an unknown diagnosis.
Introduction
Parkinson’s disease (PD) is a common neurodegenerative condition, second only to Alzheimer’s disease and the most prevalent of the parkinsonian syndromes. Diagnostic certainty of PD and the other parkinsonian syndromes (multiple system atrophy (MSA),1 progressive supranuclear palsy (PSP)2 and corticobasal syndrome(CBS))3 can only be confirmed by histopathological demonstration of the characteristic pathology and resultant nigrostriatal degeneration. In clinical practice, diagnosis of PD relies on the presence of bradykinesia and at least one of rest tremor, rigidity or postural instability.4 Atypical or mild clinical features may delay diagnosis and introduction of appropriate therapies. In a tertiary movement disorders centre, the diagnostic accuracy of clinical assessment in postmortem clinicopathologically confirmed PD did improve from 79% to 90% over a 10-year period.5 6 However, the rate of misdiagnosis is likely higher in early disease and in the primary care setting. In community patients with parkinsonian features or on antiparkinsonian medications, only 53%–83% of patients fulfilled the criteria for probable PD.7 8 Other conditions that may mimic PD include essential tremor, dystonia, drug-induced parkinsonism (DIP), vascular parkinsonism and functional movement disorder. Misdiagnosis of these disorders can have significant prognostic and management implications.
Positron emission tomography (PET) and single photon emission computerised tomography (SPECT) imaging can accurately evaluate the nigrostriatal system and aid in early diagnosis of PD.9 Vesicular monoamine transporter type 2 (VMAT2) plays an integral role in presynaptic dopamine uptake and storage and is a reliable marker of nigrostriatal terminal integrity.10 11 18F-AV-133 is a novel 18F–labelled dihydrotetrabenazine analogue that selectively binds to VMAT2 with high affinity and allows for in vivo evaluation of VMAT2 density. Several clinical studies have demonstrated the feasibility of 18F-AV-133 PET technique to assist in the diagnosis of PD and dementia with Lewy bodies.10–14 18F-AV-133 PET has multiple potential advantages compared with dopamine transporter SPECT, including improved image quality and quantification, reduced tracer administration to scan interval time and reduced scan duration. Furthermore, there is no requirement for prescan thyroid blockade in contrast to the iodine-123-labelled SPECT dopamine transporter tracers.
In a previous study, we investigated the management impact of 18F-AV-133 PET imaging in patients with clinically uncertain parkinsonian syndromes (CUPS).14 The results of the 18F-AV-133 PET altered diagnosis in 23% of participants (11 of 47) and changed management in more than half of the cases (53%; 25 of 47). Furthermore, diagnostic confidence in clinicians increased in 74% of the participants after the scan, regardless of whether the result was normal or abnormal. Total enrolment in the CUPS study subsequently reached 85 and the present study aims to further confirm the diagnostic accuracy of 18F-AV-133 PET by comparing the results of the initial scan with the clinical diagnosis at 3 years follow-up in the total cohort.
Methods
Study subjects
All patients previously recruited in our CUPS study were eligible for the current study.14 Patients with CUPS were recruited from the private and public clinics of movement disorders specialists from across the city of Melbourne, Australia. The criteria for uncertainty of diagnosis was at the discretion of the referring clinician and included the presence of atypical features of parkinsonism including poor levodopa responsiveness, lack of disease progression, dystonia and young age of onset. Participants were excluded if they had a history of malignancy within the last 5 years or if they were unable to provide informed written consent.
Patient and public involvement
Patients and the public were not involved in the design or analysis of this study. Once published, the results of the study will be summarised in a letter and disseminated to the participants and doctors involved in patient recruitment.
Study design
This was a single-centre, prospective experimental study with a mean follow-up interval of 3 years±6 months (range: 18–68 months). The study was conducted in accordance with local and international standards. All participants provided written consent prior to their inclusion in the study. At the time of follow-up, phone calls were made to the treating movement disorders specialist and study participant to establish the current diagnosis for the patient. If the treating neurologist had changed during the follow-up period, the diagnosis was made by the most recent clinician involved in the care of the participant. The clinicians had access to the initial 18F-AV-133 PET scan results. The diagnostic categories were classified into parkinsonism with nigrostriatal degeneration (including idiopathic PD, MSA, PSP and CBS), other (including essential tremor, dystonia, DIP, functional (psychogenic), monosymptomatic resting tremor) or an unclear diagnosis, that is, remained CUPS. Follow-up diagnosis was considered in agreement with the initial PET scan diagnosis if it remained in the same binary diagnostic category, that is, parkinsonism with nigrostriatal degeneration or other. For example, if a participant had a change of diagnosis from PD to MSA during the follow-up period, this was still considered a concordant result. All participants had a follow-up 18F-AV-133 PET but only those for patients who had a clinical diagnosis which was discordant to the initial PET result are reported here.
PET scan protocol and image analysis
As previously described, a 20 min emission PET scan was obtained 2 hours after intravenous injection of approximately 250 MBq of 18F-AV133.11 14 For attenuation-correction purposes, a rotation transmission sinogram in three-dimensional (3D) mode with a single 137Cs point source was acquired prior to radiotracer injection. The final images were reconstructed using a 3D row-action maximum-likelihood algorithm. The regional tracer binding of the caudate nucleus and anterior and posterior putamen were calculated using the ratio of regional activity to primary visual cortex, the latter being a region devoid of monoaminergic terminals, and therefore suitable as a reference standard. Each individual image was spatially normalised to a normal 18F-AV-133 template using statistical parametric mapping software (SPM8; Wellcome Department of Cognitive Neurology). A standard region of interest (ROI) template was previously constructed manually over 13 slices for the caudate and 8 slices for the putamen (each slice 2 mm thick). The putamen ROI was bisected to give anterior and posterior putamen binding. Abnormal images were determined quantitatively and visually. Quantitatively, abnormal images were defined as those with >50% reduction in binding in the most affected posterior putamen, which corresponds to 4 SD below the mean of the healthy control reference group11 14 that consisted of 16 healthy controls; 9 males and 7 females, with a mean age of 72±5.1 (range 64–78 years). Scans were called visually abnormal when there was significant asymmetry in the posterior putamen or marked reduction in uptake in the putamen relative to the caudate nucleus. In two cases, visual analysis was abnormal when quantitative results were not but otherwise all classifications were concordant. The binding percentage for each region was calculated by subtracting the regional control group mean binding ratio from the patient result, then dividing this by the control group mean and then multiplying by 100. This threshold is based on multiple histopathological studies, which suggest that motor symptoms of PD only emerge after at least 50% loss of dopaminergic neurons in the substantia nigra.15 16 The 3-year follow-up data were also used to test the validity of the 50% binding reduction threshold by comparison to receiver operator characteristics (ROC) curve using the Youden criterion.
Outcome variables
The primary end point of the study was the proportion of patients who had a clinical diagnosis at 3 years follow-up, which was in agreement with the results of their initial 18F-AV-133 PET scan. Secondary end points were the proportion of patients who had the same diagnosis in the follow-up period as that reached after the initial scan and the stability of diagnostic changes made after the first scan.
Statistical analysis
The results of the study are expressed as a mean±SD with accuracy figures derived from two by two contingency tables. The diagnostic accuracy of 18F-AV-133 PET was further investigated using a ROC analysis and area under the curve (AUC),17 with binding reduction threshold determined using the Youden criterion.18 Data processing and statistical analysis was conducted using Microsoft Excel 2016 software, Minitab 18 (Minitab, Pennsylvania, USA) and R V.3.4.3.19
Results
Study population
Eighty-one of the 85 participants (95%) enrolled in our CUPS study (47 previously described in the study by Alexander et al)11 14 were reviewed after 3 years. Four patients were lost to follow-up. Patient characteristics are outlined in table 1. There were no significant differences when comparing participants involved in the study with those who were lost to follow-up.
Patient characteristics at baseline in the follow-up and lost to follow-up groups
Diagnosis summary
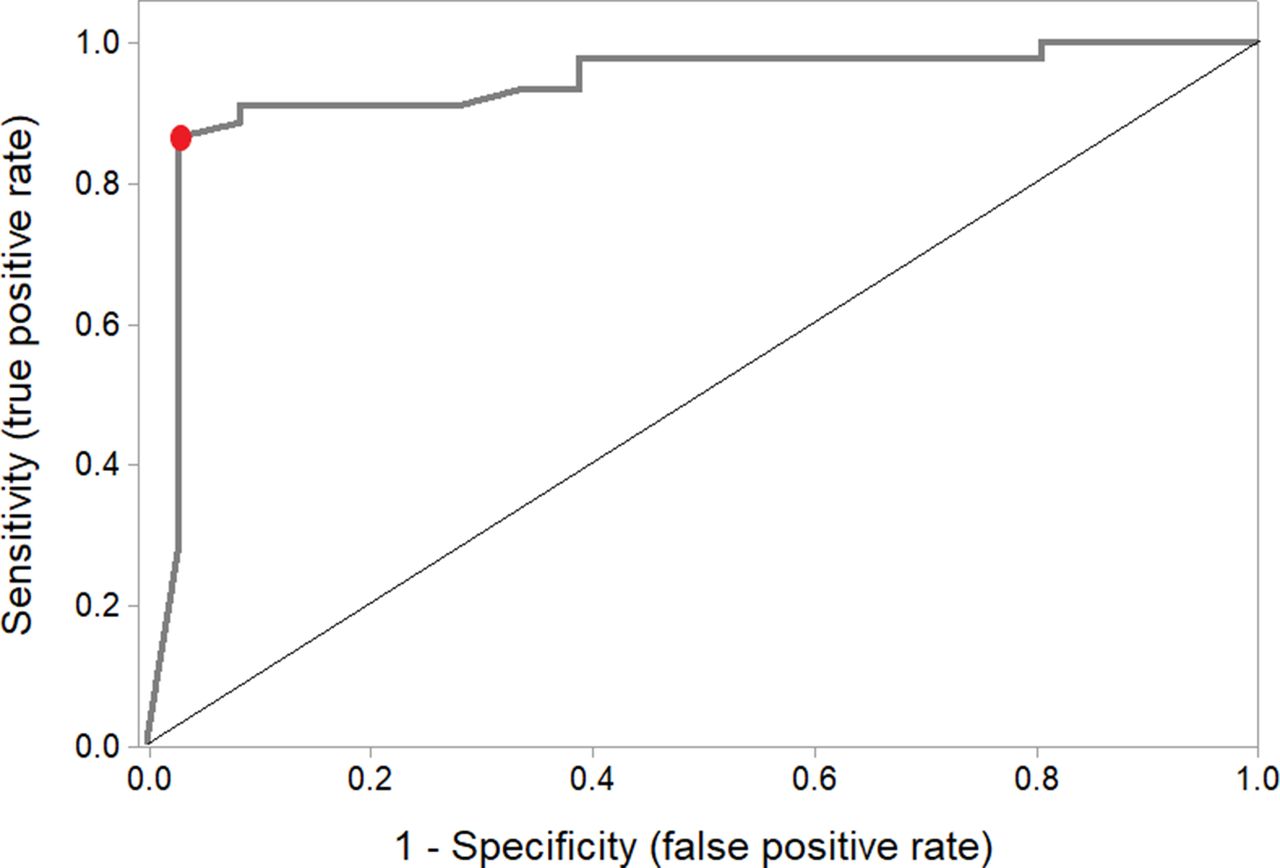
Of the 81 participants followed up, 79 (98%) had a specific clinical diagnosis and 2 cases had an inconclusive diagnosis, that is, remained CUPS. When a specific clinical diagnosis was available, the follow-up diagnosis was concordant with that suggested by the initial 18F-AV-133 PET scan in 74 cases (94%), with a positive predictive value of 98%, a negative predictive value of 89% and a sensitivity and specificity of 91% and 97%, respectively (table 2). The diagnostic agreement rate was slightly lower in the parkinsonism associated with nigrostriatal degeneration category compared with the ‘other’ category (91% vs 97%). The agreement rate of clinical diagnosis at follow-up was 67% when compared with the most likely prescan clinical diagnosis and was 97% when compared with the initial postscan diagnosis. The diagnostic accuracy of 18F-AV-133 PET in predicting parkinsonism with nigrostriatal degeneration was further evaluated with a ROC curve (figure 1). The calculated AUC was 0.94 (95% CI 0.88 to 0.99) with an optimal binding reduction threshold of 50% as per Youden criterion. The clinical diagnosis of all participants in the prescan, postscan and follow-up period are listed individually in online supplementary table 1.
Supplementary file 1
Correlation between 18F-AV-133 positron emission tomography (PET) scan result and diagnosis after 3 years
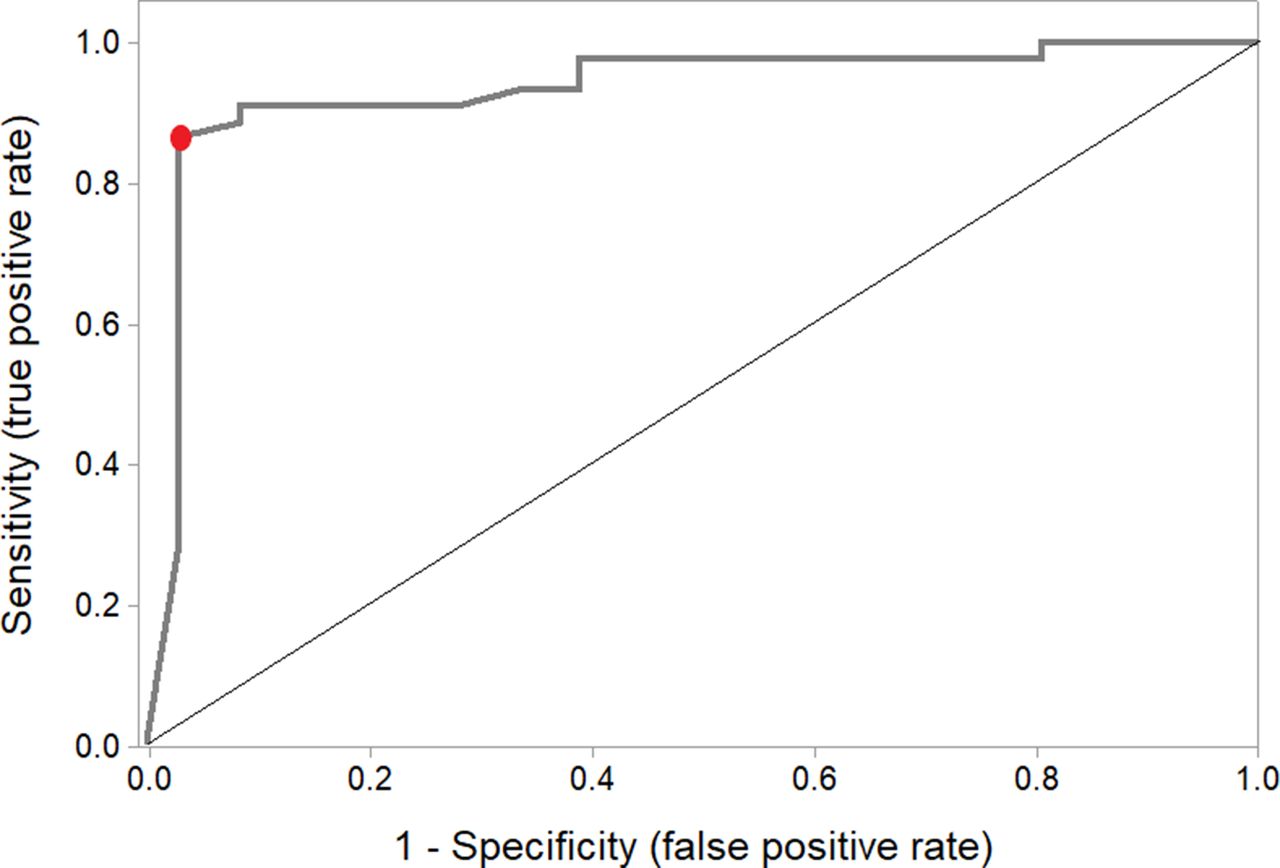
Receiver operator characteristics curve of 18F-AV-133 positron emission tomography for predicting nigrostriatal degeneration in patients with clinically uncertain parkinsonian syndrome. The red dot denotes the optimal binding reduction threshold of −50% as determined by the Youden criterion.
Discordant clinical diagnosis with imaging results
Five patients (6%) had a follow-up clinical diagnosis that did not concur with the results of their 18F-AV-133 PET scan (table 3). One participant with an abnormal scan was diagnosed prescan as rubral tremor, postscan as PD and at follow-up, diagnosis had returned to rubral tremor despite worsening of the scan (figure 2). This patient has an asymmetrical, resting, action and postural upper limb tremor that is levodopa responsive but has remained relatively stable for 30 years with no bradykinesia or rigidity. Brain MRI did not reveal a structural lesion that accounted for reduced 18F-AV-133 uptake in the absence of nigrostriatal degeneration.

{kind=link}
{kind=link}
18F-AV-133 vesicular monoamine transporter type 2 positron emission tomography (PET) in two discordant cases. Patient with ‘rubral tremor’ showing bilateral, asymmetrical reduction in tracer uptake at baseline (A) and follow-up 2 years later (B) with decline from −85% to –94% in the left posterior putamen. (C) Normal 18F-AV-133 PET scan in a patient diagnosed with Parkinson’s disease, unchanged in 2-year follow-up scan (D).
Scan results and diagnosis of patients with clinical diagnosis discordant to scan results or unknown
Three participants with a follow-up clinical diagnosis of PD had a normal 18F-AV-133 PET scan. In two of these patients, the managing clinician now considers them as having PD phenotype due to symptoms without evidence of dopaminergic deficit (SWEDD). Follow-up imaging in these two patients 2 years later remained stable (figure 2 shows one of these cases). One patient had an initial prescan and postscan diagnosis of dystonia. During the follow-up period, the diagnosis was revised to PD in the context of emerging bradykinesia and a good response to levodopa. Follow-up imaging at 3 years remained normal.
One patient had a follow-up diagnosis of progressive atypical parkinsonian syndrome. The initial and repeat 18F-AV-133 PET scan 2 years later showed stable and symmetrical binding in the lower range but <50% reduced cut-off (posterior putamen binding of −39% and −34%, respectively).
Cases with uncertain diagnosis
Two cases continue to be CUPS. One participant, a young male, had a prescan diagnosis of an unknown neurodegenerative condition. He had a normal 18F-AV-133 PET scan and the postscan diagnosis remained unclear. The patient’s symptoms have progressed but the current diagnosis remains ‘undefined neurogenetic condition’. The patient did not return for repeat 18F-AV-133 PET imaging. The second participant also had a normal initial 18F-AV-133 PET scan. The prescan diagnosis was PD and the immediate postscan diagnosis was unclear. At follow-up, the participant clinically presents with a dystonia parkinsonism syndrome. A second 18F-AV-133 PET scan 1.5 years after the initial study remained in the normal range but showed a decline in posterior putamen tracer binding from 9% to −24%. This participant has a sibling with early onset PD who had an abnormal 18F-AV-133 PET.
Follow-up after prescan to postscan diagnostic change
Of the 81 CUPS with 3-year follow-up, 24 had a change in binary diagnostic classification due to the initial 18F-AV-133 PET (see online supplementary table 1). Of these, the current clinical diagnosis remained the same as the postscan diagnosis in 23 (96%) patients. The patient with an original diagnosis of rubral tremor was reclassified as PD afteran initial abnormal 18F-AV-133 PET but the diagnosis had reverted to rubral tremor at follow-up.
Discussion
Our study provides further evidence that 18F-AV-133 PET is a feasible adjunctive tool in the diagnosis of degenerative parkinsonism. The 3-year follow-up data validated the 50% binding reduction threshold and clinical diagnosis remained remarkably concordant with the results of the 18F-AV-133 PET scan (94% agreement rate) with an impressive sensitivity and specificity of 91% and 97%, respectively. This is highly comparable to the sensitivity (87%–98%) and specificity (80%–100%) reported in the widely used 123I-FP-CIT SPECT scans (DaTSCAN).20–23 When a follow-up diagnosis had been made, the diagnosis was in agreement with the prescan diagnosis in only 67% of cases, but was in agreement with the postscan diagnosis made with the aid of the 18F-AV-133 PET scan in 97%, highlighting the diagnostic challenges in early PD.
Four patients had a clinical diagnosis of PD or atypical parkinsonism despite a normal 18F-AV-133 PET scan. This discrepancy has been widely reported with other measures of dopaminergic integrity and is referred to as SWEDD. The number of SWEDD cases in the literature has been described to be between 3.5% and 20% in patients with clinical features of PD undergoing DAT scanning.24 However, the entity of SWEDD remains controversial and may characterise a heterogenous group of conditions. Some studies have suggested that the tremor dominant presentation may represent adult-onset dystonia.25 26 However, pathologically confirmed cases of MSA and corticobasal ganglionic degeneration with normal DaTSCAN have been described in the literature.27–29 A patient with levodopa-responsive parkinsonism and dyskinesia and a G2019S mutation in the LRRK2 gene with a normal 18F-fluorodopa PET scan30 has been reported, suggesting that imaging of the nigrostriatal pathway may be normal in some cases of early PD.31 In the current study, an abnormal scan was defined as ≥50% reduction in tracer binding in the posterior putamen compared with healthy controls. This threshold is based on postmortem studies suggesting that the clinical features of parkinsonism emerge after >50% loss of dopaminergic neurons in the substantia nigra.15 16 Therefore, it is feasible that this prescribed range will miss preclinical or early PD with very mild motor symptoms. This is supported by the observation of progressive clinical and 18F-AV-133 binding decline in our patient with a suspected genetic dystonia parkinsonism syndrome. Further studies evaluating 18F-AV-133 PET in at-risk patients such as those with REM sleep behaviour disorder32 may shed light on the reasons for false negatives and could help identify an appropriate threshold for detection of preclinical individuals. Our two SWEDD cases had posterior putamen binding of −16.5% and −17% and demonstrated no decline with repeat scans after 2 years. Consistent with the literature of SWEDD, these subjects did not show clinical progression over the follow-up period.24 33 The one patient who was reclassified from dystonia to PD at follow-up had minimal decline in the scans from a posterior putamen binding of 3% to −14% after 2 years.
There were three patients who had a change in diagnosis from PD to MSA during the follow-up period. This is consistent with the literature, which suggests that presynaptic dopaminergic imaging cannot differentiate PD from atypical parkinsonian syndromes.9 Evaluation of the postsynaptic dopaminergic systems with D2 receptor binding ligands or metabolic imaging with 18F-FDG-PET has been suggested to further differentiate idiopathic PD from atypical parkinsonism.34 35
There are advantages of 18F-AV-133 PET including improved spatial resolution and there is reduced tracer uptake and scan acquisition time in comparison to DaTSCAN, without the need for thyroid blockade or other patient preparation. In addition to its role in diagnosis, the 18F-AV-133 PET may prove to be a valuable tool for disease monitoring and in patient selection and evaluation of the therapeutic impact of interventions in clinical trials.
There are limitations to the current study. The definitive diagnosis of PD relies on histopathological evidence5 and this is not available in this cohort at this time. However, in view of the logistical challenges of postmortem studies, a clinical diagnosis such as that outlined by the UK Brain Bank criteria is commonly accepted as a substitute gold standard.4 Additionally, a long clinical follow-up period, such as the one employed in this study, has been reported to improve diagnostic accuracy.36 Postmortem studies of autopsy-confirmed PD have revealed a correlation between ligand uptake in DaTSCAN and nigrostriatal neuronal loss.37 38 Similar histopathological studies would be worthwhile to further validate the diagnostic accuracy of 18F-AV-133 PET.
Conclusion
This study validates and extends the findings of our previous CUPS study, providing further evidence of the diagnostic value of 18F-AV-133 PET, with a robust impact after 3 years of follow-up indicating that management change initiated by 18F-AV-133 PET scan findings, was and remains appropriate.
Acknowledgments
The authors would like to thank Drs Andrew Hughes, Andrew Evans, David Williams, John Merory, Katya Kotchet, Katrina Reardon, Richard Peppard, Malcolm Horne and Dominic Thyagarajan for their role in patient recruitment.
References
Footnotes
Contributors SSX was involved in statistical analysis and wrote the manuscript. PKA, YL and VD were involved in the research project execution and statistical analysis. SB was involved in the research project organisation and execution. RSM and KY were involved in research project execution. VLV was involved in statistical analysis design, execution, review and critique. CCR was involved in research project conception, organisation and execution, statistical analysis review and critique and manuscript review and critique.
Funding This was an investigator-initiated study supported by a grant from Avid Radiopharmaceuticals. CCR has received research grants for imaging in dementia from Piramal Imaging, GE Healthcare, Cerveau, Astra Zeneca, Biogen and Navidea. He has been a consultant or paid speaker at sponsored conference sessions for Piramal Imaging, GE Healthcare, Astra Zeneca, Roche and Biogen. VLV has been a consultant or paid speaker at sponsored conference sessions for Piramal Imaging, GE Healthcare, Astra Zeneca and Novartis.
Competing interests A grant for this study was provided to Professor Rowe to support this study by Avid Radiopharmaceuticals, who developed and own the rights to 18 F-AV-133.
Patient consent Obtained.
Ethics approval Austin Health Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available for sharing.