


Abstract
Neuroendocrine tumors (NETs) are uncommon tumors with increasing incidence and prevalence. Current reports suggest that 68Ga-DOTATATE PET/CT imaging improves diagnosis and staging of NETs compared with 111In-DTPA-octreotide and conventional imaging. We performed a systematic review of 68Ga-DOTATATE for safety and efficacy compared with octreotide and conventional imaging to determine whether available evidence supports U.S. Food and Drug Administration approval. Methods: Medline, EMBASE, Web of Science, and Cochrane Reviews electronic databases were searched from January 1999 to September 2015. Results were restricted to human studies comparing diagnostic accuracy of 68Ga-DOTATATE with octreotide or conventional imaging for pulmonary or gastroenteropancreatic NET and for human studies reporting safety/toxicity for 68Ga-DOTATATE with 10 subjects or more thought to have NETs. Direct communication with corresponding authors was attempted to obtain missing information. Abstracts meeting eligibility criteria were collected by a research librarian and assembled for reviewers; 2 reviewers independently determined whether or not to include each abstract. If either reviewer chose inclusion, the abstract was accepted for review. Results: Database and bibliography searches yielded 2,479 articles, of which 42 were eligible. Three studies compared the 2 radiopharmaceuticals in the same patient, finding 68Ga-DOTATATE to be more sensitive than octreotide. Nine studies compared 68Ga-DOTATATE with conventional imaging. 68Ga-DOTATATE estimated sensitivity, 90.9% (95% confidence interval, 81.4%–96.4%), and specificity, 90.6% (95% confidence interval, 77.8%–96.1%), were high. Five studies were retained for safety reporting only. Report of harm possibly related to 68Ga-DOTATATE was rare (6 of 974), and no study reported major toxicity or safety issues. Conclusion: No direct comparison of octreotide and 68Ga-DOTATATE imaging for diagnosis and staging in an unbiased population of NETs has been published. Available information in the peer-reviewed literature regarding diagnostic efficacy and safety supports the use of 68Ga-DOTATATE for imaging of NETs where it is available.
Neuroendocrine tumors (NETs) are uncommon, with annual incidence approximately 50 per million persons, an almost 5-fold increase since 1973. This increase in incidence may partially reflect improvements in diagnosis. Estimated prevalence is 350 per million (1,2). Conventional imaging approved in the United States for diagnosis, staging, restaging, and assessment of treatment includes radiographs, CT, MRI, ultrasound (including endoscopic ultrasound), skeletal scintigraphy, and somatostatin receptor scintigraphy (SSRS), which is useful for imaging NETs, which typically express high levels of somatostatin receptors (3).
111In-DTPA-pentetreotide (octreotide) imaging, using planar, SPECT, or SPECT/CT imaging at 4, 24, and sometimes 48 h after injection, is the currently approved SSRS imaging modality in the United States. A breakthrough at the time (4), octreotide imaging limitations include relatively slow pharmacokinetics, high-energy γ-emissions, and unfavorable patient dosimetry limiting injectable activity to about 37–74 MBq (1–2 mCi), all resulting in relatively low-resolution images. Accordingly, newer, higher-affinity somatostatin analogs, labeled with radioisotopes with more favorable resolution and dosimetry, such as 68Ga, a positron emitter, are promising SSRS imaging agents.
Although several 68Ga-labeled SSRS imaging probes are reported (5), this systematic review and meta-analysis is limited to 68Ga-DOTATATE used in conjunction with PET with integral CT (PET/CT). If 68Ga-DOTATATE is equivalent to or better than octreotide imaging in safety and diagnostic efficacy, these results could support U.S. Food and Drug Administration approval, hopefully contributing to routine use of 68Ga-DOTATATE as the standard for SSRS imaging for patients with tumors with high expression of somatostatin receptor.
Several recent reviews describe 68Ga-DOTATATE imaging of pulmonary or gastroenteropancreatic (GEP) neuroendocrine tumors (5–9) but do not limit their reviews to comparing 68Ga-DOTATATE with octreotide imaging, combining results with other 68Ga-labeled synthetic somatostatin analogs. The lack of direct comparison of 68Ga-DOTATATE with octreotide imaging limits assessment of differential efficacy between these 2 radiopharmaceuticals. Previous reviews also did not summarize details of radiopharmaceutical compounding or observed 68Ga-DOTATATE toxicity. This review assesses the efficacy of 68Ga-DOTATATE compared with octreotide and conventional imaging and reports compounding details and safety information with the range of reported harms observed with 68Ga-DOTATATE, to determine whether sufficient data are present to support 68Ga-DOTATATE regulatory approval.
MATERIALS AND METHODS
This report follows Preferred Reporting Items for Systematic Reviews and Metaanalysis guidelines (http://www.prisma-statement.org/) for systematic reviews and meta-analyses (10). Study selection and definition of objectives with clinical relevance follows the Population, Intervention, Comparison, Outcome, and Study Type (PICOS) method (supplemental data, available at http://jnm.snmjournals.org).
Inclusion criteria are detailed in the PICOS table and include primary trials or studies with more than 10 human subjects conducted to investigate diagnosis for pulmonary or GEP NETs. Studies excluded were systematic reviews, meta-analyses, or case reviews with 10 or fewer subjects; studies not reporting 68Ga-DOTATATE compared with octreotide or conventional imaging; studies without pulmonary or GEP NET histology; studies reporting treatment, not diagnosis; and other reasons determined by reviewers making a study inapplicable. In studies with incomplete information, direct communication with the corresponding author was sought and, when provided, included in the analysis if the additional information allowed inclusion. Studies with overlapping populations were limited to the single report with the largest number of patients, or using the most recent imaging technology, as reported by the corresponding or senior author. Analysis was on a per-patient basis (i.e., diagnosis, staging, or impact on management) because, in patients with multiple lesions (primary tumor and metastases), each multiple lesion cannot be independently verified. An endpoint of cancer or benign diagnosis was established and included in data extraction. Gold standard definition, whether by pathology, imaging, or combination, was abstracted.
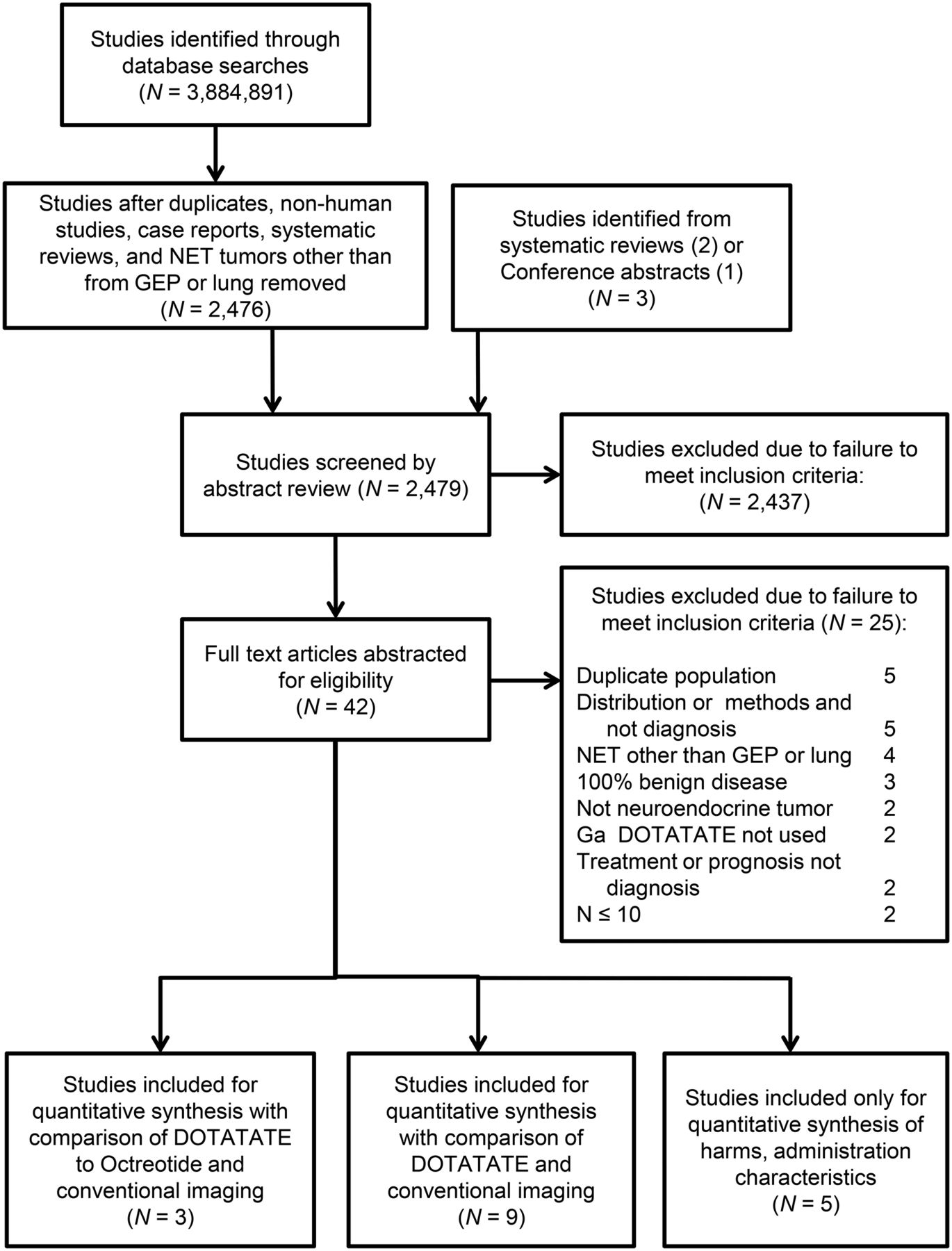
Study selection was from searching Medline, EMBASE, Cochrane Reviews electronic databases, and gray literature from January 1999 to September 29, 2015. There was no language restriction if an English translation for non-English articles or abstracts was available. Bibliographies from meta-analyses and literature reviews were examined separately, with papers of interest included in the final reviewed abstract list (Fig. 1). Article search criteria included all discovered expressions of pulmonary or GEP neuroendocrine tumors. Separately, any of the common expressions of DOTATATE or Octreotide or Pentetreotide or somatostatin or somatostatin-derived receptor were included. Formal search criteria and preliminary results for the Medline search are in the supplemental data.

Preferred Reporting Items for Systematic Reviews and Metaanalysis (PRISMA) diagram of studies from systematic review.
Summary sensitivity, specificity, and accuracy with 95% confidence intervals (CIs) were calculated for each imaging method, by study, when possible, though some studies reported only subjects with proven NET, precluding specificity measurements. Changes in treatments were abstracted from manuscripts. A random-effects model of combined sensitivity and specificity was estimated. Study characteristics possibly influencing estimates of sensitivity and specificity were included as fixed effects. A hierarchical summary receiver-operator curve was not estimated because of too few studies.
Abstracts collected by a research librarian were reviewed independently by 2 clinician reviewers masked to the other reviewer. If either reviewer determined that full data extraction was indicated, complete text review occurred with data extraction conducted independently by the reviewers. Conflicts were resolved by a third reviewer if needed. Any discrepancies in abstraction coding were resolved by consensus. Interrater reliability for study inclusion was measured by Cohen’s κ.
Quality Assessment
Reviewers assessed study quality according to prospective criteria using a modified Quality Assessment of Studies of Diagnostic Accuracy (QUADAS) set of 13 questions (supplemental data) (11,12). Questions addressed technical quality of index and reference tests, independence and accuracy of test interpretation, and sample size and population representation. Additional quality questions measured possible misclassification bias from preselection bias, incomplete diagnosis, or diagnosis driven by scan results. A quality score (maximum possible, 13) was created by adding the number of QUADAS criteria with which the study complied.
Harms were classified according to National Cancer Institute Common Toxicity Criteria for both metrics and grading of possible harms (13). When related safety or outcomes for 68Ga-DOTATATE were not reported, authors were contacted directly and requested to provide this information. All safety data are reported separately in the supplemental data. Other factors of interest abstracted from the study or via correspondence included range of DOTATATE peptide mass, range of injected activity, number of patients receiving 68Ga-DOTATATE, and whether the patients were receiving short- or long-acting octreotide medication at the time of 68Ga-DOTATATE scanning.
RESULTS
The electronic search returned 2,476 articles; bibliography reviews added 3 more. Thus, 2,479 abstracts were screened. After initial review, 2,437 articles were excluded. Inclusion agreement between reviewers was 99%; Cohen’s κ was moderately high at 0.70. Article exclusion occurred for multiple reasons, most commonly the radiopharmaceutical was not 68Ga-DOTATATE (n = 795), the article described treatment and not diagnosis (n = 578), or the article was a case review with 10 subjects or fewer (n = 674) (Fig. 1). Forty-two studies received full review, with 25 excluded on closer analysis. The remaining 17 met all inclusion criteria (Table 1). These 17 studies included 971 participants (median, 44; interquartile range, 22–51; average age, 56 y [95% CI, 56–66]), with 3 reporting direct comparison of 68Ga-DOTATATE with octreotide and conventional imaging (14–16), 9 studies comparing 68Ga-DOTATATE with conventional imaging (17–25), and 5 studies reporting comparison of 68Ga-DOTATATE with other radiopharmaceuticals without other direct imaging comparator but which were retained for reporting safety, toxicity, and method of 68Ga-DOTATATE synthesis and administration (26–30). Of the 17 included studies, 8 (47%) were retrospective (14,17,19,21,22,26–28), 8 were prospective (15,17,18,23,25,29–31), and 1 (20) did not report the data collection method. Eight studies (47%) did not mask interpreters, 4 performed some level of masking, and the remaining 5 did not report their masking methods.
Study Characteristics
Comparison with 111In-Octreotide or Conventional Imaging
A total of 169 patients were evaluated by both 68Ga-DOTATATE and octreotide in the 3 direct-comparison studies. By correspondence, Hofman et al. (14) reported 68Ga-DOTATATE PET/CT sensitivity and specificity in 40 patients of 100% and 86%, respectively. Deppen et al. (16) reported 68Ga-DOTATATE PET/CT sensitivity and specificity in 78 patients of 96% and 97%, respectively. Srirajaskanthan et al. (15) reported 68Ga-DOTATATE sensitivity of 87% and specificity of 100% in 51 patients with negative or weak octreotide scan results. Pooled cancer prevalence among all 11 studies including any comparative conventional imaging with 68Ga-DOTATATE PET/CT was 70%. In 10 of these studies, 5 had 100% of subjects with metastatic disease and 5 had a mix of malignant and benign patients, with all 10 reported per-patient results. Two studies (18,22) reported results by region or organ and not by patient and so were not included in our final meta-analysis because confirmation was not available for all areas of uptake.
Among the 10 remaining studies, with 465 patients, based on a random-effects model for 68Ga-DOTATATE PET/CT, the estimated sensitivity and specificity were 90.9% (95% CI, 81.4%–96.4%) and 90.6% (95% CI, 77.8%–96.1%), respectively (Fig. 2, forest plots). Pooled estimates of sensitivity and specificity were not influenced by any study characteristics, including study quality score, year of publication, having only cancer cases, or average age of participants. I2, which is derived from Cochran’s Q and reports the percentage of variation attributable to heterogeneity, was significant for sensitivity (65%) across the 10 studies that reported results on a per-patient basis. No heterogeneity in specificity was observed among the 5 studies (I2 = 0%) with both malignant and benign disease. However, both of these estimates of heterogeneity are likely underpowered because of too few studies and are reported here only for the sake of completeness (32). A hierarchical summary receiver-operator curve did not converge due to too few studies.
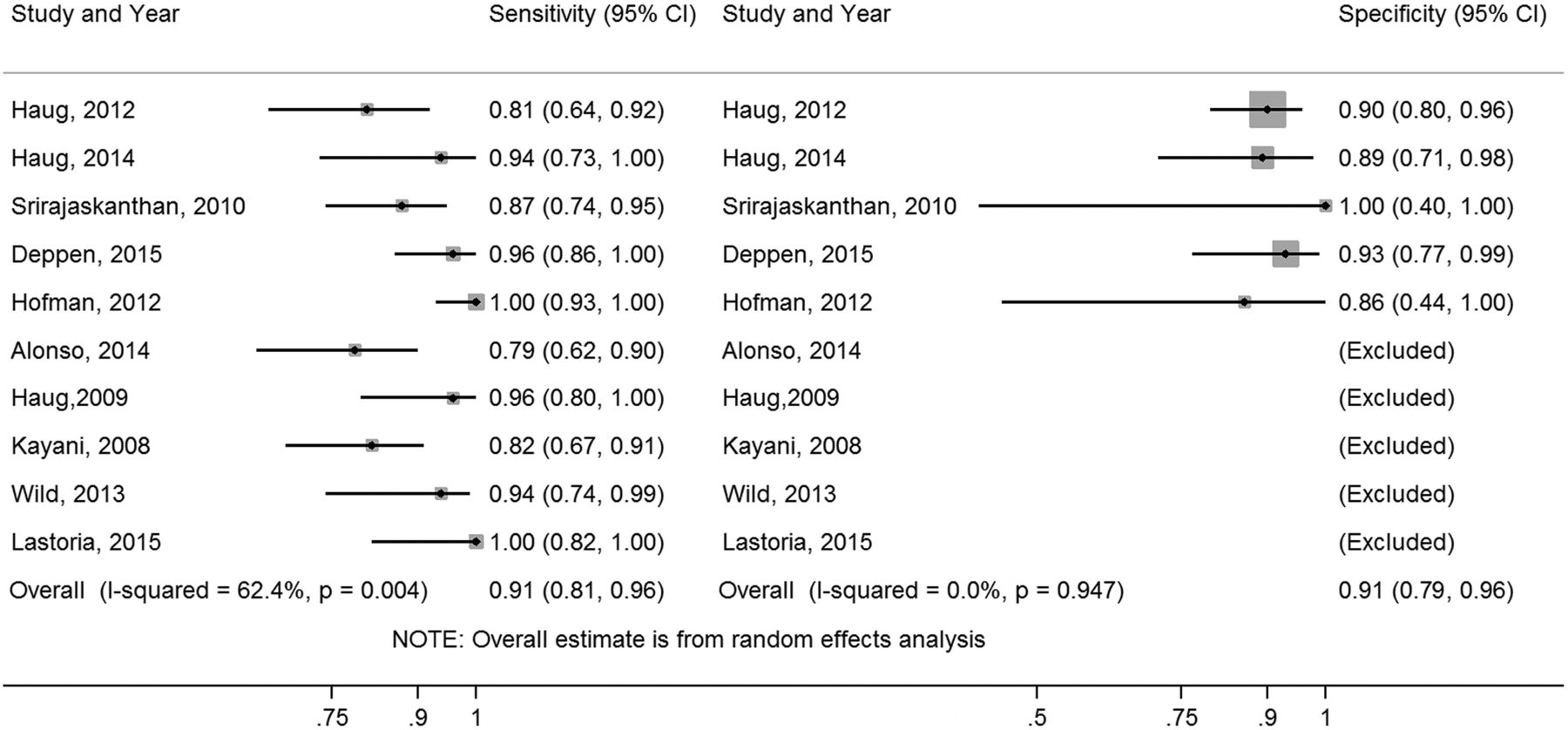
Forest plots with random-effects estimates and individual study sensitivity and specificity.
Deek’s funnel plot asymmetry test indicated no evidence for publication bias (P = 0.30) among the 5 studies reporting both sensitivity and specificity. A P value below 0.10 suggests possible publication bias; however, this bias estimate, with only 5 studies, suffers from low power, possibly underestimating publication bias. Publication bias was similar when including the additional 5 studies reporting only sensitivity (P = 0.26). It is important to note that the comparison standard for the presence or absence of disease differed across studies. Thus, the estimates of sensitivity and specificity of both 68Ga-DOTATATE and octreotide are not highly precise. Accordingly, the more robust measure of major or minor change in management is presented as a better marker of the impact of these scans on patient care.
Toxicity
There was minimal toxicity reported in the original manuscripts of all studies, either a short statement indicating that no adverse events were observed or no statement regarding toxicity. E-mail communication with the authors requesting more specific information on toxicity revealed additional information. Toxicity data for the use of 68Ga-DOTATATE, the range of DOTATATE peptide mass used, and the injected activity range are summarized in the supplemental data. The number of patients receiving 68Ga-DOTATATE, and whether the patients were receiving short-acting or long-acting octreotide medication at the time of the scan, are also shown. Only 1 study’s administered peptide mass was more than 50 μg (29), with the lowest mass ranging from 2 to 13 μg (22). Activity was under 220 MBq except in 1 study reporting 165–243 MBq (14). Deppen et al. (16), Etchebehere et al. (18), and Kunikowska et al. (29) were the only investigators reporting adverse events (n = 6). One subject had postscan tachycardia resolving without treatment (16); 2 had mild, unexplained symptoms determined by the local institutional review board to be not serious or to be related to the research (18); 2 with a history of gastritis reported abdominal pain associated with 68Ga-DOTATATE administration (effectively treated with an antispasmodic drug) (29); and the sixth subject (18) reported unilateral whole-body edema ipsilateral to the injected upper extremity, occurring within 24 h of injection and resolving spontaneously in less than 48 h, with no other sequelae, and not directly observed by medical staff. This last adverse event was determined by the local institutional review board to be not serious but possibly related to the research. Glucose testing among insulinoma patents found no changes in glucose levels (29).
Study Quality Scoring
Among the 12 studies comparing 68Ga-DOTATATE with any other imaging, 6 (50%) were retrospective, 5 were prospective, and 1 did not state the method of data collection. Four of the studies reported masking of interpreters to other patient information, and 5 did not mask scan interpreters. Three studies did not report their methods of masking (supplemental data). The median quality score across the 17 studies was 7 (interquartile range, 6–8). Quality varied from 11 of 13 QUADAS criteria in 1 study (23) to 3 of 13 quality criteria in 1 study (28). Five studies lacking comparative imaging information were included for toxicity and harm purposes only. Among 12 studies comparing 68Ga-DOTATATE with other imaging modalities, the mean quality score was 7.8 (95% CI, 6.7–9.1).
68Ga-DOTATATE PET/CT Compared with Octreotide Imaging
Hofman et al. (14), in a retrospective, masked review of 59 patients (52 proven or suspected bronchial or GEP NETs and 7 neural crest/mesenchymal tumors), determined the impact on care of 68Ga-DOTATATE compared with octreotide and conventional imaging. Reports from previous conventional imaging (contrast-enhanced CT, MRI, ultrasound, plain-film radiographs, and bone scintigraphy) were separately reviewed. 68Ga-DOTATATE better demonstrated disease extent (100%) than octreotide (83%) and conventional (68%) imaging. Treatment change impact measured by change in intended treatment before versus after 68Ga-DOTATATE scanning was high (intermodality) in 47%, moderate (intramodality) in 10%, low in 41%, and not assessable in 2%. High impact included identifying candidates for potentially curative surgery, identifying nonsurgical candidates, and changing type of systemic treatment. Compared with conventional imaging, 68Ga-DOTATATE imaging provided clinically significant information in 40 patients (56%), typically by identifying greater extent of disease. Compared with octreotide SPECT/CT, 68Ga-DOTATATE provided significant additional information in 33 of 40 (83%). On a per-lesion basis, 68Ga-DOTATATE PET/CT revealed 90 additional tumor foci (bone [18], liver [17], pancreas [15], locoregional nodes [13], distant nodes [11], small bowel [8], peritoneum [4], and pleura [4]). 68Ga-DOTATATE PET/CT had a high clinical impact compared with conventional and octreotide imaging.
Srirajaskanthan et al. (15) reported 68Ga-DOTATATE PET/CT results in 51 patients with negative (35) or equivocal (16) octreotide SPECT scans, reported by anatomic region. The patients were selected from 312 (16.3%) patients with NET with a Krenning score (33) less than 2 (uptake less than normal liver). Verification was via 3-phase CT or MRI. Forty-seven (92%) had evidence of tumor biochemically or by conventional imaging. Somatostatin analogs were not withdrawn in the 27 patients receiving these medications. Primary tumor sources were pulmonary (2), thyroid (2), thymus (2), pancreas (13), midgut (22), hindgut (2), paragangliomas (2), and unknown primary tumors (6). Previous treatments included surgery (9) and chemotherapy (10).
68Ga-DOTATATE PET/CT was positive in 168 of 226 focal lesions (74.3%) confirmed with conventional imaging, significantly greater than octreotide SPECT (P < 0.001). Impact on treatment assessed retrospectively demonstrated that 68Ga-DOTATATE had a major impact on 36 (71%). Four with negative 68Ga-DOTATATE and octreotide scans were excluded from peptide receptor radionuclide therapy. Seven of 51 patients (14%) with tumors on 68Ga-DOTATATE imaging but without symptoms began somatostatin analog treatment. Surgery was suggested in 4 (8%) patients based on potentially resectable disease confirmed with conventional imaging, but not seen with octreotide SPECT, although 1 declined surgery. 68Ga-DOTATATE imaging changed management in 70%. In 47 patients with evidence of tumor by MRI, by CT, or biochemically, 68Ga-DOTATATE PET/CT found disease in 41 (87.2%), with 39% referred for peptide receptor radionuclide therapy because of strong 68Ga-DOTATATE uptake despite being misclassified on octreotide SPECT.
In a prospective study, Deppen et al. (16) reported 68Ga-DOTATATE PET/CT scanning in 97 patients with known or suspected NETs, 78 also undergoing 111In-DTPA-octreotide scans, and reported quantitative toxicology and systematic tracking of possible harms from 68Ga-DOTATATE. 68Ga-DOTATATE imaging was compared with planar (4%), SPECT (33%), and SPECT/CT (62%) 111In-DTPA-octreotide scans. Though half of comparative 68Ga-DOTATATE scans occurred more than 180 d after the comparator 111In-DTPA-octreotide scan, no difference was found in level of treatment change comparing time between scans. A limitation of toxicity testing was that 28 participants were missing some or all postscan blood analyses.
Deppen et al. (16) had 3 important findings. First, 68Ga-DOTATATE was significantly more accurate (0.94; 95% CI, 0.89–1.00) than octreotide imaging (0.82; 95% CI, 0.74–0.90; P < 0.02). Second, 68Ga-DOTATATE imaging had a major impact (intermodality) on treatment decisions in 29 (37%) and minor (intramodality) impact on 9 (12%) (Fig. 3). Third, there were no adverse events requiring treatment. One patient with a baseline heart rate of 87 had postscan transient asymptomatic tachycardia (rate, 112), spontaneously returning to normal sinus rhythm within an hour. Four patients had minor and transient asymptomatic changes in laboratory tests. 68Ga-DOTATATE was equivalent or superior to 111In-DTPA-octreotide imaging in all 78 patients.

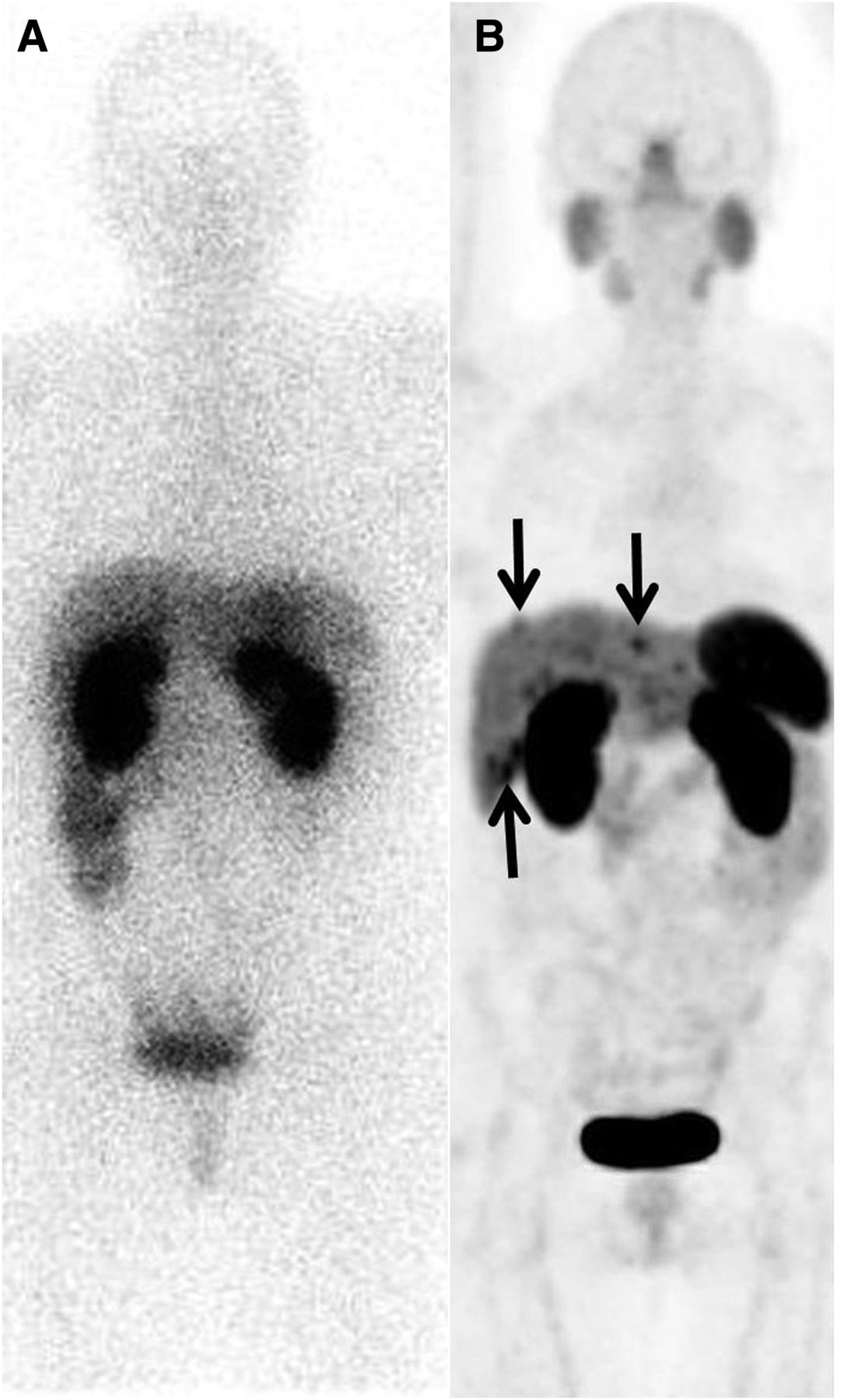
111In-DTPA-octreotide SPECT/CT (A) and 68Ga-DOTATATE PET/CT (B) (maximum-intensity projections shown) of patient with suspected recurrence of small bowel NET in liver. One metastasis was suspected on SPECT/CT (not shown). Nine liver metastases were found with PET/CT, resulting in change in surgical plan. Findings confirmed at surgery.
68Ga-DOTATATE PET/CT Compared with Conventional Imaging
Nine studies reported 68Ga-DOTATATE compared with conventional imaging (17,19,20,25) or with conventional imaging with other imaging including 68Ga-DOTANOC (22,23), 18F-DOPA (24), MRI (25), 99mTc-HYNIC-octreotide (18), or 18F-fluorodoxyglucose (21) (Table 1). These studies, summarized in the supplemental data, vary widely in patient populations and study purpose. Five studies examined 68Ga-DOTATATE accuracy in identifying metastatic disease (18,20–23).
DISCUSSION
Direct comparisons of octreotide and 68Ga-DOTATATE imaging for diagnosis and staging in biased populations of NETs have been published. One unbiased but unpublished prospective study (31) found 68Ga-DOTATATE significantly superior to octreotide in both diagnostic accuracy and impact on treatment. Limited published literature directly comparing 111In-DTPA-octreotide with 68Ga-DOTATATE imaging supports the superiority of 68Ga-DOTATATE PET/CT for diagnosis or reassessment of tumors with high somatostatin receptor expression. Available evidence also supports that 68Ga-DOTATATE imaging often demonstrates tumor uptake in some patients with negative or equivocal 111In-DTPA-octreotide scans, thereby identifying additional patients who might benefit from peptide receptor radionuclide therapy (34). No significant harms were reported. Additionally, 68Ga-DOTATATE PET/CT provides lower effective radiation dose (35), superior image quality, and greater patient convenience via a shorter examination time than 111In-DTPA-octreotide imaging.
CONCLUSION
Reports comparing 68Ga-DOTATATE PET/CT with 111In-DTPA-octreotide and conventional imaging support the added value of 68Ga-DOTATATE imaging with additional sites of tumor, including metastases and occult primaries often seen. The available evidence demonstrates that, in mass dose of 125 micrograms or less, 68Ga-DOTATATE has minimal toxicity. These reports have limitations from lack of consistent patient populations, prior treatment protocols, and confirmation. Given the superior image quality, lower radiation dosimetry, and greater patient convenience (2 h vs. 2–3 d for octreotide imaging), 68Ga-DOTATATE is clinically equivalent or superior to octreotide imaging and should be used where available.
DISCLOSURE
The costs of publication of this article were defrayed in part by the payment of page charges. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734. This work was supported by an unrestricted gift from the Society of Nuclear Medicine and Molecular Imaging and the Vanderbilt Institute for Clinical and Translational Research grant, UL1TR000011 from NCATS/NIH (REDCap database). No other potential conflict of interest relevant to this article was reported.
Footnotes
Published online Jan. 14, 2016.
- © 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
REFERENCES
- Received for publication August 19, 2015.
- Accepted for publication December 4, 2015.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Dual Somatostatin Receptor/18F-FDG PET/CT Imaging in Patients with Well-Differentiated, Grade 2 and 3 Gastroenteropancreatic Neuroendocrine Tumors
- Long-Term Outcomes of Submaximal Activities of Peptide Receptor Radionuclide Therapy with 177Lu-DOTATATE in Neuroendocrine Tumor Patients
- A Randomized, Factorial Phase II Study to Determine the Optimal Dosing Regimen for 68Ga-Satoreotide Trizoxetan as an Imaging Agent in Patients with Gastroenteropancreatic Neuroendocrine Tumors
- Peptide Receptor Radionuclide Therapy with 67Cu-CuSarTATE Is Highly Efficacious Against a Somatostatin-Positive Neuroendocrine Tumor Model
- Constrictive bronchiolitis in diffuse idiopathic pulmonary neuroendocrine cell hyperplasia
- Influential Factors in the Preparation of 68Ga-DOTATATE
- 64Cu-DOTATATE PET/CT for Imaging Patients with Known or Suspected Somatostatin Receptor-Positive Neuroendocrine Tumors: Results of the First U.S. Prospective, Reader-Masked Clinical Trial
- A Prospective Observational Study to Evaluate the Effects of Long-Acting Somatostatin Analogs on 68Ga-DOTATATE Uptake in Patients with Neuroendocrine Tumors
- 111In-Pentetreotide Scintigraphy Versus 68Ga-DOTATATE PET: Impact on Krenning Scores and Effect of Tumor Burden
- 64Cu-SARTATE PET Imaging of Patients with Neuroendocrine Tumors Demonstrates High Tumor Uptake and Retention, Potentially Allowing Prospective Dosimetry for Peptide Receptor Radionuclide Therapy
- Aetna and 68Ga-DOTATATE: A Sequel to "The Injustice of Being Judged by the Errors of Others" (1)
- PET Radiopharmaceuticals: Whats New, Whats Reimbursed, and Whats Next?
- Appropriate Use Criteria for Somatostatin Receptor PET Imaging in Neuroendocrine Tumors
- Current Concepts in 68Ga-DOTATATE Imaging of Neuroendocrine Neoplasms: Interpretation, Biodistribution, Dosimetry, and Molecular Strategies
- MANAGEMENT OF ENDOCRINE DISEASE: Flushing: current concepts
- Somatostatin Receptor 2-Targeting Compounds
- The Impact of Somatostatin Receptor-Directed PET/CT on the Management of Patients with Neuroendocrine Tumor: A Systematic Review and Meta-Analysis
- Principles of diagnosis and management of neuroendocrine tumours
- Association between neuroendocrine tumors biomarkers and primary tumor site and disease type based on total 68Ga-DOTATATE-Avid tumor volume measurements
- 68Ga-DOTATATE PET/CT Interobserver Agreement for Neuroendocrine Tumor Assessment: Results of a Prospective Study on 50 Patients
- Citius, Altius, Fortius: An Olympian Dream for Theranostics
- Comparison of the Impact of 68Ga-DOTATATE and 18F-FDG PET/CT on Clinical Management in Patients with Neuroendocrine Tumors