


Abstract
99mTc-EC20 is a folate receptor (FR)–targeted imaging agent consisting of the vitamin folate conjugated to 99mTc. FR is expressed on a variety of epithelial cancers, with advanced cancers often expressing FR at significantly higher levels than earlier stages of the disease. The goals of this pilot study were to determine the percentages of various solid tumors that accumulate 99mTc-EC20 in vivo and to correlate 99mTc-EC20 uptake with immunohistochemistry (IHC) analysis of FR expression in available biopsied tumor tissue. Methods: A total of 154 patients with proven or suspected cancer and at least one lesion of ≥1.5 cm underwent imaging with 99mTc-EC20. The majority of these patients (77%) had a diagnosis of renal cell carcinoma. The remaining patients had a variety of other solid tumors. Whole-body planar images were obtained 1–2 h after injection, followed by SPECT of the region containing index lesions. The uptake of 99mTc-EC20 in tumors was scored as no uptake, mild uptake, or marked uptake. The resultant 99mTc-EC20 data were analyzed for correlation with the expression of the α-isoform of FR, as determined by IHC analysis, in tissue available from prior or subsequent surgery or biopsy. Results: The administration of 99mTc-EC20 was well tolerated. Tumors with increased 99mTc-EC20 uptake were identified in 68% of patients, and IHC results were positive for the expression of the α-isoform of FR in 67% of patients. The agreement between methods was 61% overall (κ = 0.096; 95% confidence interval = −0.085 to 0.277), with 72% agreement of positive results and 38% agreement of negative results. Conclusion: In vivo imaging with 99mTc-EC20 identified approximately two thirds of patients as having FR-positive tumors. Agreement between imaging and in vitro IHC was poor but was potentially confounded by a lack of correlation between the time of tissue sampling and the time of 99mTc-EC20 imaging, the heterogeneous expression of FR in metastatic lesions from the same patient, and the inability to detect the β-isoform of FR by IHC. This pilot study of 99mTc-EC20 scintigraphy indicates that the agent is safe and well tolerated and that this noninvasive procedure may have utility in selecting patients likely to benefit from FR-targeted therapy.
Folate transfers one-carbon chemical units from donor to acceptor molecules in a variety of biosynthetic processes (1), including the synthesis of nucleotide precursors of DNA. In cellular metabolism, the proliferative or kinetic state of the cell influences the rate of internalization of folate, indicating that it is critical to rapidly dividing cells, including many cancers.
Before facilitating any bioprocess, however, folate must gain entry into the cell, and in mammalian cells, entry proceeds via 2 distinct transport systems: the reduced folate carrier system, which is the primary method of folate entry into normal cells, and the folate receptor (FR) system. Although it has been noted that the FR glycoprotein is expressed in a minority of normal tissues, it is expressed at high levels on the surface of some epithelial tumors, such as ovarian cancer (2).
Studies evaluating over 8,000 tissue samples have shown that FR is overexpressed in cancers of the ovaries (>95% of samples tested exhibited FR expression at least 6 times greater than normal expression levels), mesothelium (≈100%), lungs (>75%), kidneys (≈65%), endometrium (≈60%), breasts (>60%), and cerebrum (≈50%) and clinically nonfunctional pituitary adenomas (∼80%). It has been hypothesized that the proliferative or metabolic state of malignant cell types causes the upregulation of FR to facilitate the entry of folate for accelerated synthetic and metabolic processes (3–15).
The overexpression of FR on tumor cells relative to that on normal cells provides a potential mechanism for targeted antitumor therapy (16). Various FR-targeted therapies intended to deliver potent cytotoxic antitumor agents to cells that selectively express FR are currently under development (17–19).
An important adjunct to the development of molecularly targeted therapies, including FR-targeted therapy, is the codevelopment of diagnostic tests to provide information on the presence or absence of the molecular target in question. Such diagnostic tests would allow for the “preselection” of individuals who might benefit from FR-targeted treatment and would likely play a critical role in the design and implementation of therapeutic trials. EC20 is a 99mTc-based folate-linked radiopharmaceutical that has been developed to identify patients whose tumors express FR. 99mTc-EC20 has the potential to provide the noninvasive detection of tissues expressing FR. 99mTc-EC20 targets FR with a mechanism that is identical to that used for targeting experimental therapeutic molecules (such as EC145 and EC0225) to the receptor.
The uptake of 99mTc-EC20 into solid tumors was assessed in a series of single-arm, open-label pilot studies to determine the percentages of patients whose tumors would show 99mTc-EC20 uptake; to determine the correlation of 99mTc-EC20 imaging results with the results of immunohistochemical (IHC) staining of tumor tissue for FR; and to provide information on the safety of a single injection of 99mTc-EC20 in patients with solid tumors.
MATERIALS AND METHODS
Patients
Eligible patients were at least 18 y of age and had known or suspected metastatic renal cell carcinoma (protocols EC20.3 and EC20.9), pituitary adenoma (protocol EC20.7), solid tumors (protocol EC20.8), or ovarian carcinoma or recurrent endometrial carcinoma (protocol EC20.4). Patients with at least one identifiable lesion of ≥1.5 cm, as diagnosed by CT, MRI, or ultrasonography, and good renal function (serum creatinine level ≤1.5 times the upper limit of the normal range) were enrolled in the study. Patients were asked to provide a formalin-fixed, paraffin-embedded tissue sample of the primary tumor or site(s) of metastatic or recurrent disease obtained by a previous surgical or biopsy procedure for the purpose of an IHC assay of FR (α-isoform) or were asked to provide tissue obtained at surgery or biopsy scheduled after 99mTc-EC20 imaging.
Patients were excluded from the study if they were participating simultaneously in the study of other investigational agents, had received an investigational agent or therapeutic chemotherapy within 7 d of enrollment in this trial, were unable to tolerate the conditions for radionuclide imaging, or had received another radiopharmaceutical that would have interfered with the assessment of 99mTc-EC20 distribution. Pregnant or breast-feeding women were also excluded from the study. The study protocol was approved by the institutional review board at each participating study center, and all patients gave written informed consent before participation.
Radiopharmaceutical Preparation
EC20 for injection was packaged as a sterile lyophilized powder in a single reagent vial containing the components EC20 (100 μg), sodium α-d-glucoheptonate dihydrate (80 mg), and tin(II) chloride dihydrate (80 μg). 99mTc-EC20 was prepared by adding up to 1,850 MBq of 99mTc-sodium pertechnetate into the vial and heating the vial in a boiling water bath for 18 ± 2 (mean ± SD) min. The radiochemical purity of 99mTc-EC20 was determined by thin-layer chromatography (20) at the time of preparation and was required to be ≥90% for administration.
Imaging Procedure
Tracer dose and imaging time were chosen in part on the basis of previous studies of 99mTc-EC20 in humans (21). Pharmacokinetic studies showed that the disappearance of decay-corrected radioactivity from blood fits a 2-compartment model, with harmonic means of 25 min and 29 h. These data likely reflect rapid serum clearance and urinary excretion but slow movement of the tracer from a peripheral compartment back to the blood. On the basis of human biodistribution data, radiation dosimetry with 99mTc-EC20 is comparable to that with other diagnostic radiopharmaceuticals, with an average effective dose of 1.1 mrem/MBq and the largest absorbed dose of 9.2 mrem/MBq (to the kidneys).
Patients were instructed to discontinue taking folic acid supplements for at least 2 d before their scheduled imaging study. On the day of the imaging study, patients were administered 2 intravenous injections: 1 mg of folic acid (to reduce the uptake of 99mTc-EC20 in normal tissues) and, 1–3 min later, 0.1 mg of EC20 labeled with 555–925 MBq of 99mTc-pertechnetate over 30 s in a total injection volume of 1–2 mL. Each injection was given as a slow intravenous push via a free-flowing indwelling intravenous catheter in an upper-extremity vein (i.e., in the antecubital fossa). The mean administered activity was 851 MBq (range, 606.8–1,054.5 MBq). The mean activity injected per kilogram of body weight was 10.73 MBq (range, 4.81–19.98 MBq/kg).
At approximately 1–2 h after injection, anterior and posterior midthigh to head planar images were acquired in a 256 × 1,024 (minimum) matrix word-mode format with a total scan time of 20–35 min. The images were obtained with a dual-detector, large–field-of-view γ-camera that was equipped with low-energy, high-resolution parallel-hole collimators. A 20% symmetric energy window was centered over the 140-keV photopeak of 99mTc.
SPECT images of the region that was known to contain the target lesion(s), as identified by conventional imaging (CT, MRI, or ultrasonography), were obtained after planar imaging. The SPECT images included 120–128 total projections over 360° with 15–20 s per stop and were reconstructed in 3 orthogonal planes.
Image Interpretation
An on-site nuclear medicine physician, who was unaware of the outcome of the IHC assay, evaluated the planar and SPECT images for the uptake of 99mTc-EC20 in the identified lesions. The physician used the conventional imaging studies to identify up to 3 presumed malignant lesions of ≥1.5 cm (one dimension) for each patient and compared the uptake of 99mTc-EC20 in these lesions with the background. The uptake of 99mTc-EC20 in the lesions was scored as no uptake (less than or equal to background), mild uptake (slightly increased compared with background), or marked uptake (strikingly increased compared with background). A result of “no uptake” was scored as 99mTc-EC20 negative, whereas a result of “mild uptake” or “marked uptake” was scored as 99mTc-EC20 positive (EC20+). On the basis of the expected uptake observed in animal models and a phase I dosimetry study, the uptake of 99mTc-EC20 in the kidneys, liver, bladder, and spleen was assessed with the same 3-point scale as that used for malignant lesions. Additional areas of uptake were recorded when noted by the physician.
Tissue FR Assay
The formalin-fixed, paraffin-embedded tissue samples available from surgery or biopsy were analyzed for FR by an IHC assay specific for the α-isoform of FR. Evaluation of the stained samples was accomplished in a semiquantitative manner with a light microscope to assess the degree of circumferential membranous staining in the tumor cell population. The findings were classified into 1 of 4 categories: 0 = no staining in tumor cells above background; 1+ = weak staining in ≥5% of tumor cells; 2+ = moderate staining in ≥5% of tumor cells; and 3+ = strong staining in ≥5% of tumor cells. A staining result of 0 was scored as IHC negative, whereas a staining result of 1+, 2+, or 3+ was scored as IHC positive.
Safety Assessment
Vital signs were obtained within 5 min of injection (baseline) and at 1 h after injection. Blood and urine specimens for clinical laboratories were obtained within 2 h of injection and at 22–28 h after injection. Treatment-emergent adverse events were monitored through the time of the patient's follow-up laboratory measurements at 22–28 h after injection. Additionally, the patients were instructed to report any adverse events that occurred up to 7 d after injection.
Statistical Methods
The number of patients characterized as having tumors with no uptake, mild uptake, or marked uptake of 99mTc-EC20 and the number of patients who had IHC staining results of 0, 1+, 2+, or 3+ were tabulated, and the percentage of patients who had EC20+ tumors, as determined by 99mTc-EC20 imaging (i.e., those whose tumors showed mild or marked uptake), and FR-positive (FR+) tumors, as determined by IHC staining (i.e., those who had a score of 1+, 2+, or 3+) were calculated. A 2 × 2 frequency table was constructed to compare the 99mTc-EC20 imaging and IHC staining results.
The overall percentage of agreement of the 2 methods, the agreement of positive 99mTc-EC20 imaging results and positive IHC results, and the agreement of negative 99mTc-EC20 imaging results and negative IHC results were calculated. A κ-coefficient with a 95% confidence interval (CI) was calculated to examine the agreement between the 2 methods (22,23).
Adverse events, clinical laboratory evaluations, and vital signs were summarized descriptively. Quantitative laboratory measurements were categorized according to the normal reference range (low, normal, and high), and shift tables of the frequencies for preinjection versus postinjection categories were prepared. Changes in laboratory values and vital signs that met predefined criteria for clinical significance were summarized.
RESULTS
Patients
A total of 155 patients were enrolled and underwent imaging with 99mTc-EC20 at 6 centers between 15 April 2003 and 31 August 2005. One patient later withdrew his consent for his scan to be included in the study and therefore was included only in the safety data presented here, not the imaging data. One patient received a second administration of 99mTC-EC20 approximately 77 d after his initial imaging to assess uptake after resection of his primary tumor. This patient's data for both assessments were included in assessments of efficacy and safety but were counted only once for the determination of baseline demographics. The study population was primarily white (92%) and male (64%) and ranged in age from 32 to 80 y (mean, 57.8 y). The tumor types were primarily renal cell carcinomas (119 patients), benign ovarian tumors (8 patients), ovarian carcinomas (7 patients), breast carcinomas (6 patients), and pituitary adenomas (6 patients). The remaining 8 patients had small cell lung carcinoma; lung carcinoma (type unspecified); colon, endometrial, and thyroid carcinomas; non-Hodgkin's lymphoma; sarcoma; and glioma (1 patient each). Approximately 88% of patients had metastatic disease at the time of study entry, with the lungs (74%), lymph nodes (45%), liver (29%), and bone (23%) representing the primary sites of metastasis.
The mean time from the initial cancer diagnosis to the time of the 99mTc-EC20 scan was 45.2 mo (range, −0.8 to 221.3 mo), and the mean time from the most recent recurrence or progression to the time of the 99mTc-EC20 scan was 2.4 mo (range, −0.6 to 36.6 mo). A total of 155 patients completed the study (i.e., they received 99mTc-EC20) and had at least one scan (either planar imaging or SPECT).
Biodistribution
The percentage of patients with uptake in the liver, kidneys, bladder, spleen, and other organs are shown in Table 1. Physiologic (usually marked) uptake of 99mTc-EC20 was noted in the kidneys and bladder in almost all patients, consistent with the known expression of FR on the proximal tubules of the kidneys (24) and the urinary excretion of the tracer. Mild to marked uptake was also seen in the liver in all patients, causing hepatic lesions (when present) to appear as photopenic defects, even in patients with marked uptake in lesions elsewhere in the body. Hepatic uptake of 99mTc-EC20 has been seen in animal models (20); however, it can be partially blocked by inhibitors of organic anion transport, suggesting that it is mediated, at least in part, by mechanisms other than FR binding (C.P. Leamon, oral communication, July 2007). Uptake (usually mild) was frequently seen in the spleen and rarely in other organs not associated with the tumors, such as the thyroid, lymph nodes, bowel, stomach, and joints. Uptake in the thyroid, bowel, stomach, and choroid plexus was uncommon and likely was related to a small amount of free 99mTc-pertechnetate which was easily recognizable and had no appreciable effect on image interpretation. Spleen uptake is related to the known presence of the β-isoform of FR in normal splenic tissue, as well as the presence of FRs on activated macrophages (25,26). Uptake (usually mild) in bone marrow was observed in nearly all patients and was assumed to reflect the normal physiologic distribution of the tracer.
Biodistribution of 99mTC-EC20
Efficacy Results
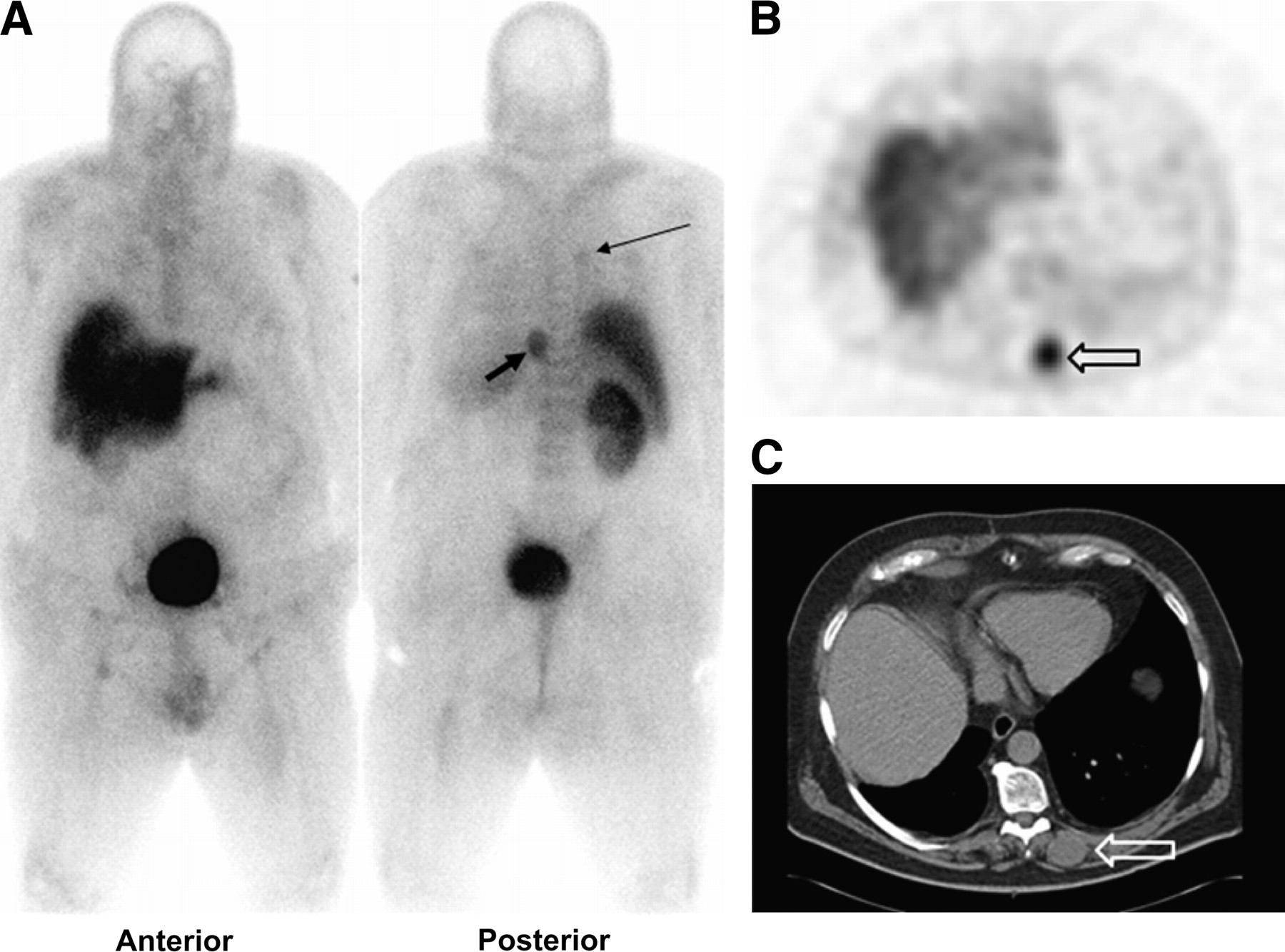
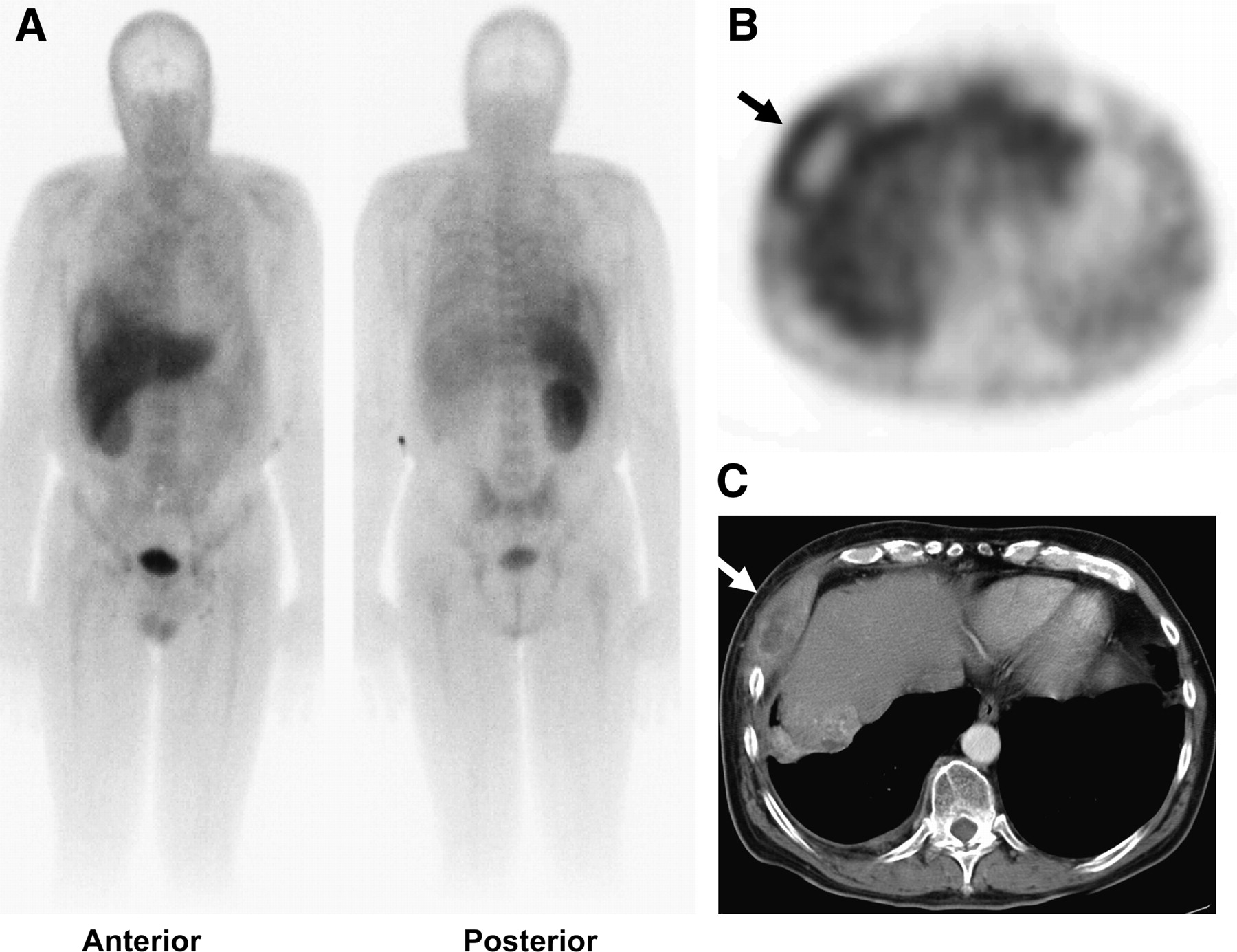
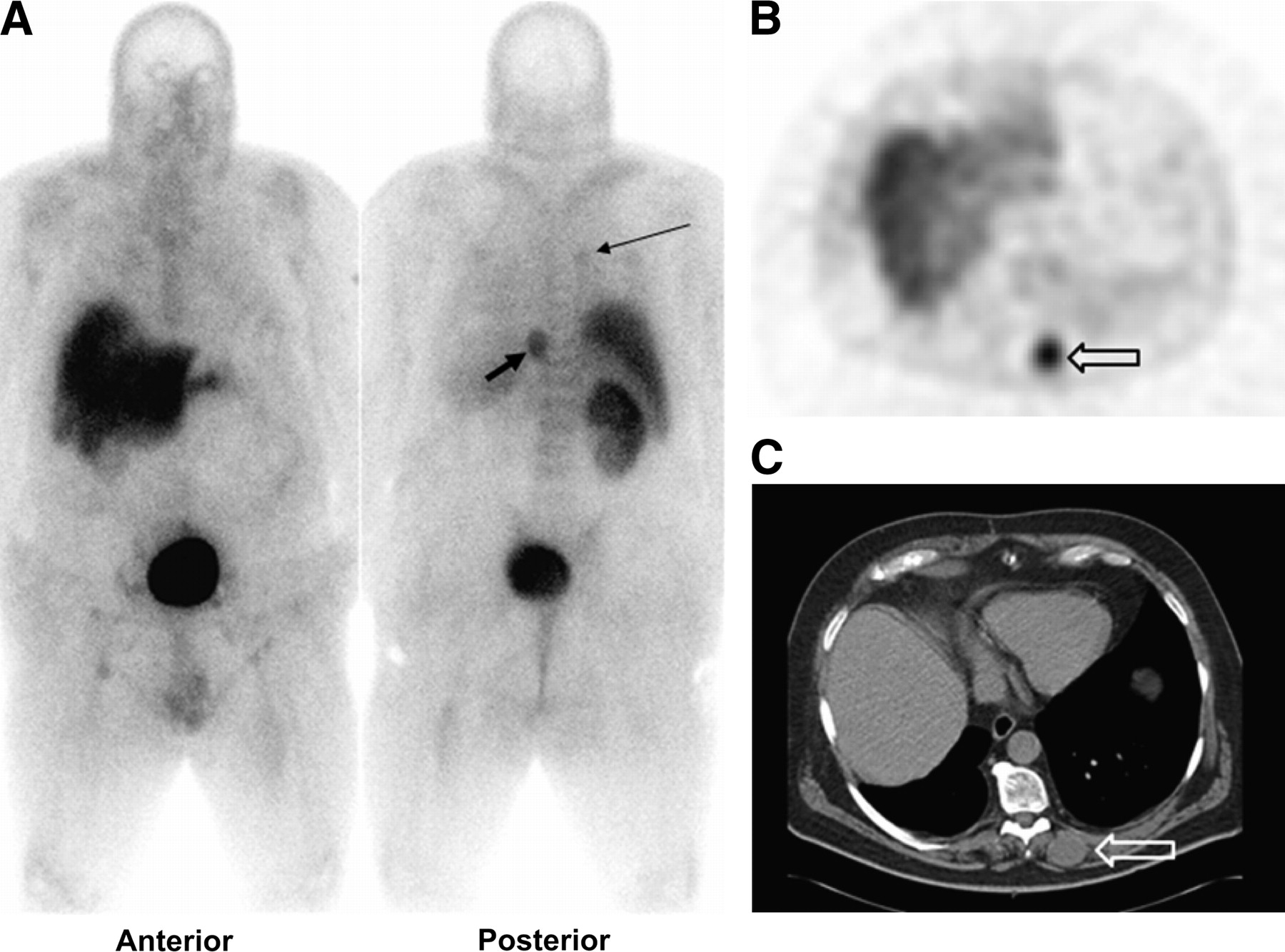
99mTc-EC20 images were evaluated for 154 patients; conventional images for the identification of target lesions were unavailable for 1 patient for comparison with the 99mTc-EC20 images. Of the 154 patients who were evaluated, 105 (68%) had at least one metastatic site that showed uptake of 99mTc-EC20 on either planar imaging or SPECT and were therefore classified as having EC20+ tumors (Table 2). Of the 105 patients who had EC20+ tumors, 57 (54%) had tumors that showed marked uptake of 99mTc-EC20 and 48 (46%) had tumors that showed mild uptake. A total of 374 lesions were evaluated by planar imaging, and 369 lesions were evaluated by SPECT. When assessed by planar imaging, 141 lesions (38%) showed 99mTc-EC20 uptake, with 66% of these showing mild uptake and 34% showing marked uptake. When assessed by SPECT, 185 lesions (50%) showed 99mTc-EC20 uptake, with 58% of these showing mild uptake and 42% showing marked uptake. Figure 1 shows representative whole-body planar scintigrams, SPECT images, and corresponding CT images that exhibit the localization of 99mTc-EC20 in a radiographically demonstrable chest wall metastasis. Figure 2 shows marked uptake in a metastasis in the paraspinal muscles. Figures 1 and 2 also demonstrate subtle uptake in other, smaller metastases.

Anterior and posterior whole-body planar (A) and transverse SPECT (B) 99mTc-EC20 images in 59-y-old man with renal cell carcinoma revealed large, destructive right chest wall metastasis (arrow). Scintigraphic findings correlated well with those on CT image (C), including photopenia in area of central necrosis. These scintigraphic results suggested that lesion was FR+. Note faint uptake in left renal fossa, thought to represent postsurgical inflammation. Mild uptake in right lung and right paratracheal region corresponded to other sites of metastatic disease demonstrated on CT (not shown). Small foci of mild 99mTc-EC20 uptake were noted in inguinal regions bilaterally; this finding was seen in many patients and may be secondary to FRs on activated macrophages.
99mTc-EC20 images of 57-y-old man with known pulmonary metastases from renal cell carcinoma. Anterior and posterior whole-body planar images (A) revealed faint uptake of tracer in right upper-lobe pulmonary nodule (1.8 × 2.1 cm) (thin arrow) that was demonstrated on CT (not shown). More intense tracer uptake was seen in mass (2.7 × 3.5 cm) (thick arrow) in left paraspinal muscles. Planar images also revealed faint bilateral inguinal nodal uptake of 99mTc-EC20. Paraspinal mass also was demonstrated on transverse SPECT image (B) and corresponding CT image (C) (arrows).
99mTc-EC20 Image Evaluation
Of the 155 patients who completed the study, 123 had samples available for IHC staining. As determined by IHC staining for the α-isoform of FR, 67% of these patients had FR+ tumors (Table 3). Overall, the 99mTc-EC20 image evaluations corresponded to the IHC staining results for 61% of the patients (Tables 4 and 5). The κ-coefficient was 0.096 (95% CI = −0.085 to 0.277), indicating poor chance-corrected agreement. The agreement of EC20+ results with FR+ results was 72%, whereas the agreement of 99mTc-EC20–negative results with FR-negative results was 38%.
Distribution of IHC Scores
Comparison of 99mTc-EC20 Imaging Results and IHC Staining Results
Agreement of 99mTc-EC20 Imaging Results and IHC Staining Results
Fewer than 5% of patients had metastatic disease detected by 99mTc-EC20 imaging that was not detected by CT. None of these additional sites of metastatic disease would have changed the staging of the tumors (other metastatic sites had been detected by CT).
Approximately 30% of the patients were found to have mild to moderate uptake within numerous small foci in the inguinal and axillary regions. When present, these were always multifocal and bilateral. Lymph nodes in these regions were consistently considered normal on the basis of CT criteria.
Safety Results
A total of 17 adverse events were reported in 13 (8%) of the 155 patients receiving 99mTc-EC20. Only 3 events (lower abdominal pain in 1 patient and nausea and vomiting in 1 patient) were considered by the investigator to be “possibly related” to the study treatment. Adverse events in 7 patients resulted in hospitalization and, thus, were categorized as serious adverse events. None of the serious adverse events was considered by the investigator to be “related” to the administration of 99mTc-EC20.
No “clinically important effects” were observed with regard to hematology, serum chemistry, or urinalysis, as judged on the basis of the mean change in values from before injection to after injection of 99mTc-EC20. No systematic shifts from normal values before injection to abnormal values after injection were observed for any laboratory test, and none of the patients had postinjection laboratory values that the investigator considered to be clinically significant. No “clinically important effects” were observed for heart rate or for systolic or diastolic blood pressure at 1 h after injection of 99mTc-EC20.
DISCUSSION
High-affinity FRs are overexpressed in several human cancers, including those of the ovaries, brain (i.e., meningiomas, ependymomas, and brain metastases), endometrium, and kidneys (3–13). 99mTc-EC20, an FR-targeted diagnostic agent, allows for noninvasive, whole-body assessments of FR expression status and, thus, may identify patients who have FR+ tumors and who may benefit from FR-targeted therapy. Preclinical (animal) imaging studies have been performed with normal and M109 tumor–bearing BALB/c mice (19,20). These studies showed scintigraphically detectable uptake in FR+ tumors placed intraperitoneally or subcutaneously. The uptake of 99mTc-EC20, quantified by an in vitro assay, was proportional to FR density and to tumor size. Such results suggested that 99mTc-EC20 could be used to detect FR+ tumors in humans noninvasively. This report represents the first published data on the use of 99mTc-EC20 to image tumors in humans.
A single injection of 99mTc-EC20 was well tolerated. Only 8% of patients experienced an adverse event during administration and the follow-up period, and only 3 adverse events were considered to be “possibly related” to the injection. No drug-related serious adverse events occurred, and no clinically important effects of 99mTc-EC20 on laboratory assays or on the monitoring of vital signs were observed.
The results of the present study of 154 patients with a variety of solid tumors demonstrated that 68% of the patients showed uptake of 99mTc-EC20 in their tumors (i.e., EC20+ tumors). In comparison, IHC staining for the α-isoform of FR in 123 patients demonstrated that 67% of these patients had FR+ tumors. In all patients, the correlation of the 99mTc-EC20 imaging results with the IHC staining results was 61%, although there was better agreement for positive imaging and staining results than for negative imaging and staining results (72% vs. 38%). Chance-corrected agreement between 99mTc-EC20 imaging results and IHC staining results was poor (κ = 0.096; 95% CI = −0.085 to 0.277).
When considering the relatively poor agreement between the results of 99mTc-EC20 imaging and IHC, one must recognize that the present study was not designed as a lesion-to-lesion comparison of 99mTc-EC20 imaging and IHC. In most cases, the tissue samples available were limited to the primary neoplasm (often obtained months or years before study entry), and scanning was performed in patients with metastatic disease after resection of the primary neoplasm. Surgical removal or biopsy and IHC analysis of all of the metastatic lesions imaged in the present study would have been scientifically preferable but was not performed for practical and ethical reasons. Furthermore, the clinical relevance of such data is limited because of differences in the types of FRs detected by IHC and imaging, as discussed in the next paragraph.
Discrepant results for the 2 methods may reflect a difference in the FR status of the primary neoplasm versus the metastatic disease after excision of the primary tumor or heterogeneity in FR expression between metastatic lesions within a patient. In fact, evidence supporting both of these hypotheses exists. Studies comparing FR expression with tumor stage have suggested that FR expression is increased in more advanced (i.e., metastatic) disease (11). In the present study, 42% of patients with renal cell carcinomas had a heterogeneous mixture of lesions, including some with no uptake and others with mild or marked uptake. An additional consideration is that only 1 of the 2 FR isoforms (α-isoform) is detected by IHC, and IHC may detect nonfunctional as well as functional receptors. In contrast, 99mTc-EC20 is capable of recognizing and binding to both the α-isoform and the β-isoform of FR and only binds functional receptors that are accessible to the imaging agent. All of these issues suggest that 99mTc-EC20 imaging may be a more accurate means of predicting the response to FR-targeted therapy than is IHC, particularly IHC performed on the primary tumor. The ultimate test of this hypothesis will require a therapeutic clinical trial in which the response to FR-targeted therapy is correlated with 99mTc-EC20 scan results. Such a trial is already under way.
Other explanations for the lack of correlation include the possibility that uptake, particularly in larger and more destructive lesions, may have been secondary to associated inflammation, an observation consistent with the presence of FRs on the surface of activated macrophages (26) and the localization of 99mTc-EC20 uptake in the joints of patients with active rheumatoid arthritis (27). Finally, the high background activity found in the liver precluded an assessment of the FR status of hepatic metastases, as all metastases were either undetectable or photopenic.
Few previously unknown sites of metastatic disease were discovered on the scans. However, the present study was not designed to test the usefulness of 99mTc-EC20 in improving the staging of renal cell carcinomas or other cancers. The majority of patients enrolled in the present study already had known distant metastases; therefore, staging was not likely to be altered. A study addressing this topic would best be performed with patients who have lower stages of disease.
An interesting incidental finding was that of mild to moderate uptake within numerous foci in the inguinal and axillary regions bilaterally in some patients. Although the basis and clinical relevance of this uptake are uncertain, the uptake may identify lymph nodes harboring activated macrophages, known to express FRs.
CONCLUSION
A single intravenous injection of 99mTc-EC20 resulted in detectable uptake on planar scintigraphy or SPECT for 68% of patients and was well tolerated by adult patients with a variety of solid tumors. The true accuracy of scintigraphy in identifying patients with FR+ metastases and thereby successfully selecting patients for FR-directed therapy could not be assessed in the present study. The 99mTc-EC20 imaging results, which mainly assessed metastatic sites, did not correlate well with the IHC staining results. However, IHC analysis was largely limited to primary tumor samples; therefore, the lack of correlation is not surprising, given that the FR status of metastases is often different from that of the primary tumor and given the other reasons discussed earlier.
99mTc-EC20 imaging is a safe, noninvasive procedure that may identify FRs in recurrent or metastatic disease without the need for biopsy and that may have utility in identifying patients who may benefit from treatment with FR-targeted therapy.
Acknowledgments
The study was supported by Endocyte, Inc. The authors gratefully acknowledge the contributions of the following investigators: Farrokh Dehdashti, Washington University, St. Louis, MO (image review); James W. Fletcher, Indiana University Hospital, Indianapolis, IN (image review); Raghuveer Halkar, Emory University, Atlanta, GA (image review); Val J. Lowe, Mayo Clinic, Rochester, MN (image review); and Joel Picus, Washington University, St. Louis, MO (patient recruitment). We also thank Sue Bever (study management), Natalie Carnahan (data management), and Sujana Santhapuram (data management) of Endocyte, Inc., for their contributions to this study and Dr. Chris Leamon for help in preparing the article.
Footnotes
-
COPYRIGHT © 2008 by the Society of Nuclear Medicine, Inc.
References
- Received for publication November 30, 2007.
- Accepted for publication February 28, 2008.





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Identification of a PET Radiotracer for Imaging of the Folate Receptor-{alpha}: A Potential Tool to Select Patients for Targeted Tumor Therapy
- A Microdosing Study with 99mTc-PHC-102 for the SPECT/CT Imaging of Primary and Metastatic Lesions in Renal Cell Carcinoma Patients
- Folate Receptor {beta}-Targeted PET Imaging of Macrophages in Autoimmune Myocarditis
- Is Targeting the Folate Receptor in Ovarian Cancer Coming of Age?
- The Thymidine Phosphorylase Imaging Agent 123I-IIMU Predicts the Efficacy of Capecitabine
- A 99mTc-Labeled Ligand of Carbonic Anhydrase IX Selectively Targets Renal Cell Carcinoma In Vivo
- Folate Receptor-{beta} Imaging Using 99mTc-Folate to Explore Distribution of Polarized Macrophage Populations in Human Atherosclerotic Plaque
- Imaging the Folate Receptor on Cancer Cells with 99mTc-Etarfolatide: Properties, Clinical Use, and Future Potential of Folate Receptor Imaging
- Targeting Folate Receptors to Treat Invasive Urinary Bladder Cancer
- Phase I Study of Folate Conjugate EC145 (Vintafolide) in Patients With Refractory Solid Tumors
- Folic Acid Conjugates for Nuclear Imaging of Folate Receptor-Positive Cancer
- In Vivo Assay of Folate Receptors in Nonfunctional Pituitary Adenomas with 99mTc-Folate SPECT/CT
- Impact of High and Low Folate Diets on Tissue Folate Receptor Levels and Antitumor Responses Toward Folate-Drug Conjugates