


Abstract
Patients with rising prostate-specific antigen (PSA) levels after definitive local therapy of prostate carcinoma present a diagnostic dilemma. A local recurrence would be amenable to additional local therapy with curative intent, whereas metastatic disease would require palliative androgen ablation therapy. In this study, we evaluated the effectiveness of PET with 11C-acetate (AC PET) for evaluation of patients with rising PSA after radical prostatectomy or radiation therapy. We also compared the reliability of AC PET in detecting recurrent prostate cancer with that of PET with 18F-FDG. Methods: Two groups of patients with PSA recurrence were enrolled in this study: group A, 30 patients after prostatectomy, and group B, 16 patients after radiation therapy. After administration of 1,110 MBq (30 mCi) of 11C-acetate, whole-body PET images were obtained. After allowing for 11C decay, 555 MBq (15 mCi) of 18F-FDG were administered and repeated whole-body imaging was performed. The PET findings were scored as positive or negative in each of the following regions: prostatic bed, pelvic nodes, paraaortic nodes, and other sites (bone or soft tissue). PET findings were correlated with those of CT, bone scintigraphy, and biopsy. Results: Twenty-seven of 46 AC PET studies (59%) had positive findings, whereas only 8 18F-FDG PET studies had positive findings (17%). Limiting the analysis to patients with findings confirmed by CT, bone scintigraphy, or biopsy or considered highly likely to represent tumor, 14 (30%) had disease identified by AC PET, whereas only 4 (9%) had disease identified by 18F-FDG PET. CT was performed on 22 patients and had positive findings in 3 (14%). Thirteen of 22 patients (59%) with serum PSA > 3 ng/mL had positive AC PET findings, whereas only 1 of 24 patients (4%) with serum PSA levels ≤ 3 ng/mL had positive findings. Conclusion: AC PET demonstrates marked uptake in prostate cancer and has higher sensitivity than 18F-FDG PET. These preliminary data show that 11C-acetate is a promising tracer for detection of recurrent prostate cancer.
Prostate cancer is the most commonly diagnosed cancer and the second leading cause of cancer death in men over the age of 40 y in the United States (1). Despite effective therapy (radical prostatectomy or radiation) for localized prostate carcinoma, some patients have local recurrences or distant metastases after treatment. Although conventional imaging modalities are used in follow-up, the role of CT and MRI in revealing nodal disease or distant metastases is controversial (2), thus hampering identification of recurrence.
Recurrent or persistent disease after treatment by prostatectomy or radiation therapy is often first detected as the reappearance of a measurable level of prostate-specific antigen (PSA) or a rise in PSA. No imaging method reliably detects disease in these patients with PSA recurrence, although CT and scintigraphy are sometimes used. Overall, approximately 30% of men with detectable PSA levels after radical prostatectomy have local recurrences, whereas approximately 70% are anticipated to have distant disease alone or combined with local disease (3). In patients with recurrent disease, a key treatment decision is based on whether the disease is localized in the prostate fossa, and thus amenable to radiotherapy, or widespread, requiring androgen ablation therapy or systemic chemotherapy. If the sites of cancer in the early phase of recurrent disease were known, patients would be treated properly, leading to fewer side effects, a better prognosis, and reduced treatment cost.
PET for tumor imaging using the radiopharmaceutical 18F-FDG was first introduced to image brain tumors almost 20 y ago (4). 18F-FDG PET is now a widely accepted and highly effective way to image a wide variety of cancers (e.g., (5)).
This success of 18F-FDG PET in many cancers has led several groups to evaluate this radiopharmaceutical in prostate cancer. Unfortunately, the primary disease within the gland cannot be reliably imaged (6–10). This poor performance of 18F-FDG PET is likely related to the relatively slow growth of most prostate cancers, with a consequently low glucose metabolic rate, as well as to other factors, including significant excretion of the tracer into the adjacent urinary bladder. 18F-FDG PET has been shown to have relatively high sensitivity when applied only in patients with aggressive prostate cancers, such as those with a high histologic grade, high clinical stage, or high serum PSA level (8). Therefore, 18F-FDG PET has some value for diagnosis of prostate cancer and should be considered for use in such patients. Radioimmunoscintigraphy (RIS) with the monoclonal antibody 111In-capromab pendetide (ProstaScint; Cytogen Corp., Princeton, NJ) is performed at many institutions (11). Although imaging with this radiopharmaceutical may be of value, the sensitivity and specificity are far from ideal, with most reports indicating a range of 50%–70% for both measures.
Recently, PET using 11C-acetate (AC PET) was evaluated in patients with prostate cancer (12,13). Investigators from the Michigan and Fukui groups showed a high sensitivity of AC PET for prostate cancer lesions. Therefore, we undertook this study to confirm the findings of these initial reports in a larger number of patients with recurrent prostate cancer after attempted curative therapy. Preliminary reports of this work were presented at the 48th annual meeting of the Society of Nuclear Medicine in Toronto, Ontario, Canada, in 2001 and at the 97th annual meeting of the American Urological Association in Orlando, Florida, in 2002 (14,15).
MATERIALS AND METHODS
Patient Selection
Between June 2000 and February 2002, 2 groups of patients were studied—patients who had recurrent disease manifested by a detectable serum PSA after radical prostatectomy (group A), and patients who failed radiation therapy as the primary treatment for their disease (group B). The serum PSA value was determined with a double monoclonal antibody radioimmunoassay (Tandem-R; Hybritech, Inc., San Diego, CA). The rather restrictive criteria set forth below were designed to maximize the chance of detecting disease by PET. Inclusion in group A required prior radical prostatectomy, a preoperative PSA level > 10 ng/mL, a detectable postoperative PSA, and at least 1 of the following: a positive tumor margin at surgery, seminal vesicle involvement by tumor, extracapsular extension of tumor, involvement of ≥25% of the prostate by tumor, or positive nodes at surgery. Inclusion in group B required prior radiation therapy for prostate cancer, a rising PSA based on 3 consecutive measurements, and either a pretreatment PSA level > 10 ng/mL or a Gleason score ≥ 7 for the original diagnostic biopsy. None of the patients in either group were currently being treated with hormone ablation.
The study was approved by the Institutional Review Board and the Radioactive Drug Research Committee of Washington University School of Medicine. All patients gave written informed consent for study participation.
Imaging Protocol
All patients underwent AC PET and 18F-FDG PET on the same day. 18F-FDG PET was performed after a fast of at least 4 h. To exclude fasting hyperglycemia, a blood sample for determination of blood glucose level was obtained before 18F-FDG injection. To facilitate clearance of urinary activity, a Foley catheter was placed in the bladder and 20 mg of furosemide were administered intravenously. Patient hydration was established by infusion (typically 1,000 mL) of 0.9% saline solution throughout the study through an intravenous catheter. Patients in whom a Foley catheter could not be placed were studied without intravenous hydration or administration of furosemide; however, oral hydration was encouraged.
PET imaging was performed with an ECAT EXACT HR+ tomograph (CTI Corp., Knoxville, TN). After standard transmission scanning of the torso, 1,110 MBq (30 mCi) of 11C-acetate were injected and 15 min of dynamic emission imaging of the pelvis was performed. Then, static emission scanning of the rest of the torso was performed over an additional 20–25 min. At the end of image acquisition, the patient left the scanner and was injected with 555 MBq (15 mCi) of 18F-FDG. A series of transmission and emission scans at the same levels as for the AC PET study was obtained beginning approximately 40–90 min after administration of 18F-FDG (75–130 min after 11C-acetate injection), a time adequate to permit essentially complete decay of 11C-acetate with a half-life of 20 min.
For both PET studies, a segmentation algorithm was used to generate the transmission map (16), and transaxial slices were reconstructed by the ordered-subset expectation maximization iterative algorithm followed by Butterworth filtering. Typical reconstructed resolution was 8 mm in full width at half maximum.
Image Interpretation
The AC PET and 18F-FDG PET images were independently evaluated visually by 2 experienced observers who were unaware of the clinical information except for the selection criteria for this study. They were asked to record the site of any abnormalities and, afterward, the results of correlation with other imaging studies if any were available. The 18F-FDG PET images were evaluated first, followed by the AC PET data. Only minor discrepancies arose between the 2 reviewers’ interpretations, and these were resolved by a joint reading.
Correlation with Other Studies
The PET findings were correlated with the results of biopsy or directly with bone scintigraphy, conventional radiography, or CT, when available. Lesions seen on PET confirmed to represent tumor by biopsy, by bone scintigraphy with radiographic confirmation, or by correspondence to a definite mass seen on CT were considered indicative of a high probability of disease. PET findings without independent confirmation that were believed likely to represent malignancy because of the intensity of tracer uptake and, for lymph nodes, the characteristic focal appearance were also scored as high probability. PET findings of lesser intensity or without a completely characteristic appearance—typically when there was concern that the focus represented activity in bowel or bladder—were scored as intermediate probability. Frequently, a focus of uptake was clearly due to bowel or urinary uptake and was not tabulated as a finding. Other areas of mild uptake, most commonly in inguinal lymph nodes, were seen frequently with AC PET and were not judged to represent tumor because of their mild nature and lack of correlation with areas of clinical concern.
Statistical Evaluation
The age, serum PSA value, and Gleason score of the 2 groups were tested with the Mann-Whitney nonparametric 2-sample test. Univariate analysis for categoric values was performed using the Fisher exact test. For both tests, a probability value < 0.05 was considered significant.
RESULTS
Patient Population
The study population consisted of 46 patients with adenocarcinoma of the prostate (median age, 65 y; range, 49–79 y). The primary curative treatment was radical prostatectomy in 30 patients (group A) and radiation therapy with or without hormonal therapy in 16 patients (group B). The mean Gleason score for the postprostatectomy group was slightly higher than that for the postradiation group (7.6 ± 0.9 vs. 6.6 ± 0.8, P = 0.001). The mean PSA values were 4.9 ng/mL (range, 0.3–47.5 ng/mL) for group A, 5.8 ng/mL (range, 0.5–11.5 ng/mL) for group B, and 5.2 ng/mL overall. The 2 groups did not significantly differ in age or serum PSA value at the time of the PET study. The demographic characteristics and PET, CT, bone scan, and biopsy findings are summarized in Table 1.
Clinical Information and Imaging and Biopsy Findings
Detection of Relapse
Typical PET studies are shown in Figs. 1–3. With AC PET, 27 of 46 patients (59%) had positive findings considered to indicate a high or intermediate probability of recurrent tumor, whereas only 8 (17%) had positive findings with 18F-FDG PET (Table 2). Limiting the analysis to the high-probability studies, the yield of AC PET for recurrent disease was 30%, versus only 9% with 18F-FDG PET; all patients with abnormal 18F-FDG PET findings also had positive AC PET findings.

Coronal 18F-FDG PET (A) and AC PET (B) images are shown for patient 14, 77-y-old man with PSA relapse and serum PSA value of 10.5 ng/mL 8 y after radical prostatectomy and 5 y after salvage external-beam radiation therapy. Histologic diagnosis showed Gleason score of 8 at surgery. CT and 111In-capromab pendetide studies were negative for tumor. 18F-FDG PET shows only urinary activity in right ureter (u) and bladder (b). AC PET shows high uptake in multiple paraaortic lymph nodes (n). Incidentally noted is normal uptake in pancreas (panc).
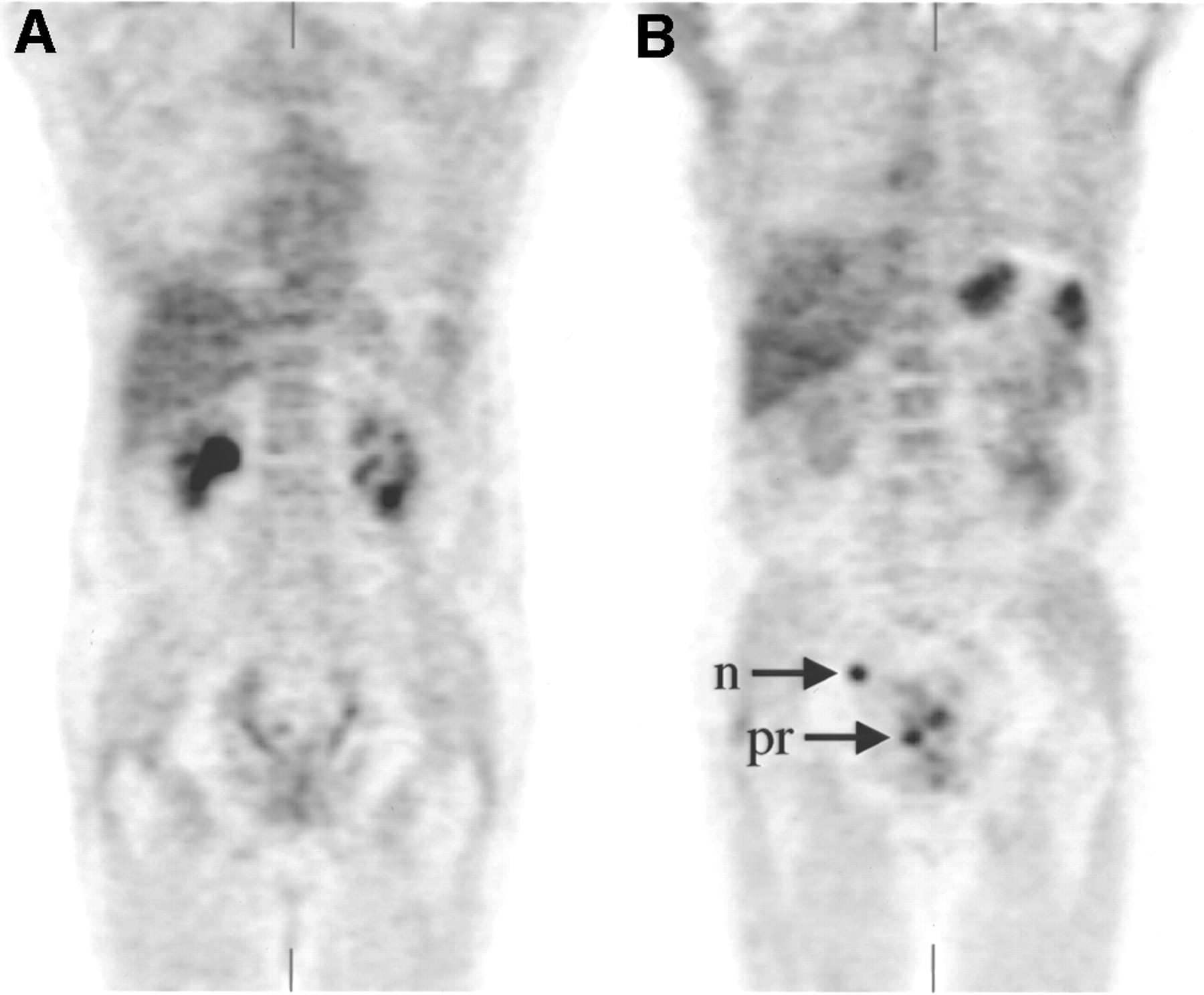
Coronal images are shown for patient 3, 71-y-old man with PSA relapse and serum PSA value of 3.7 ng/mL 8 y after radical prostatectomy. Histologic diagnosis showed Gleason score of 10 at surgery. (A) 18F-FDG PET is negative for tumor. (B) AC PET shows high uptake in right common iliac lymph node (n) and prostatic bed (pr).

Coronal and transaxial 18F-FDG PET (A) and AC PET (B) images and CT image (C) are shown for patient 23, 73-y-old man with increasing serum PSA value of 9.1 ng/mL 2 y after external-beam radiation therapy. Histologic diagnosis showed Gleason score of 7 at time of treatment. 18F-FDG PET shows no uptake in prostate and pelvic lymph nodes. AC PET shows bilateral high uptake in iliac lymph nodes (n). CT shows corresponding 1.5 cm iliac nodes (n).
Positive PET Studies
Considering individual sites (Tables 1 and 3), in group A local recurrence was detected by AC PET in 2 patients (7%), with 1 confirmed by biopsy. Ten patients (33%) had lymph node metastases. Two group A patients (7%) had bone metastases; these were confirmed by bone scintigraphy in one, and no recent bone scan was available for the other. In group B, 10 patients (62%) showed positive AC PET findings in the prostate bed, with 2 confirmed by biopsy. Six group B patients (38%) had lymph node metastases. Two group B patients (13%) had bone metastases.
Sites Detected by AC PET
CT was performed on 22 patients and had positive findings in 3 (14%) (Table 4). AC PET findings were positive in all 3 patients and in an additional 10 patients (Table 2), although confirmatory proof was not available in these patients. 18F-FDG PET findings were positive in only 2 of those patients. Excluding the 2 patients with positive bone scintigraphy findings, AC PET had positive findings in 11 patients and 18F-FDG PET in only 2. Among the 7 positive with disease independently confirmed by CT, bone scintigraphy, or prostate biopsy, AC PET had positive findings in 5 and 18F-FDG PET in 2.
Non-PET Imaging Results
As shown in Figure 4, 13 of 22 patients (59%) with a serum PSA level > 3 ng/mL had high-probability AC PET, whereas only 1 of 24 patients (4%) with a serum PSA level ≤ 3 ng/mL had a high-probability study (P < 0.001).
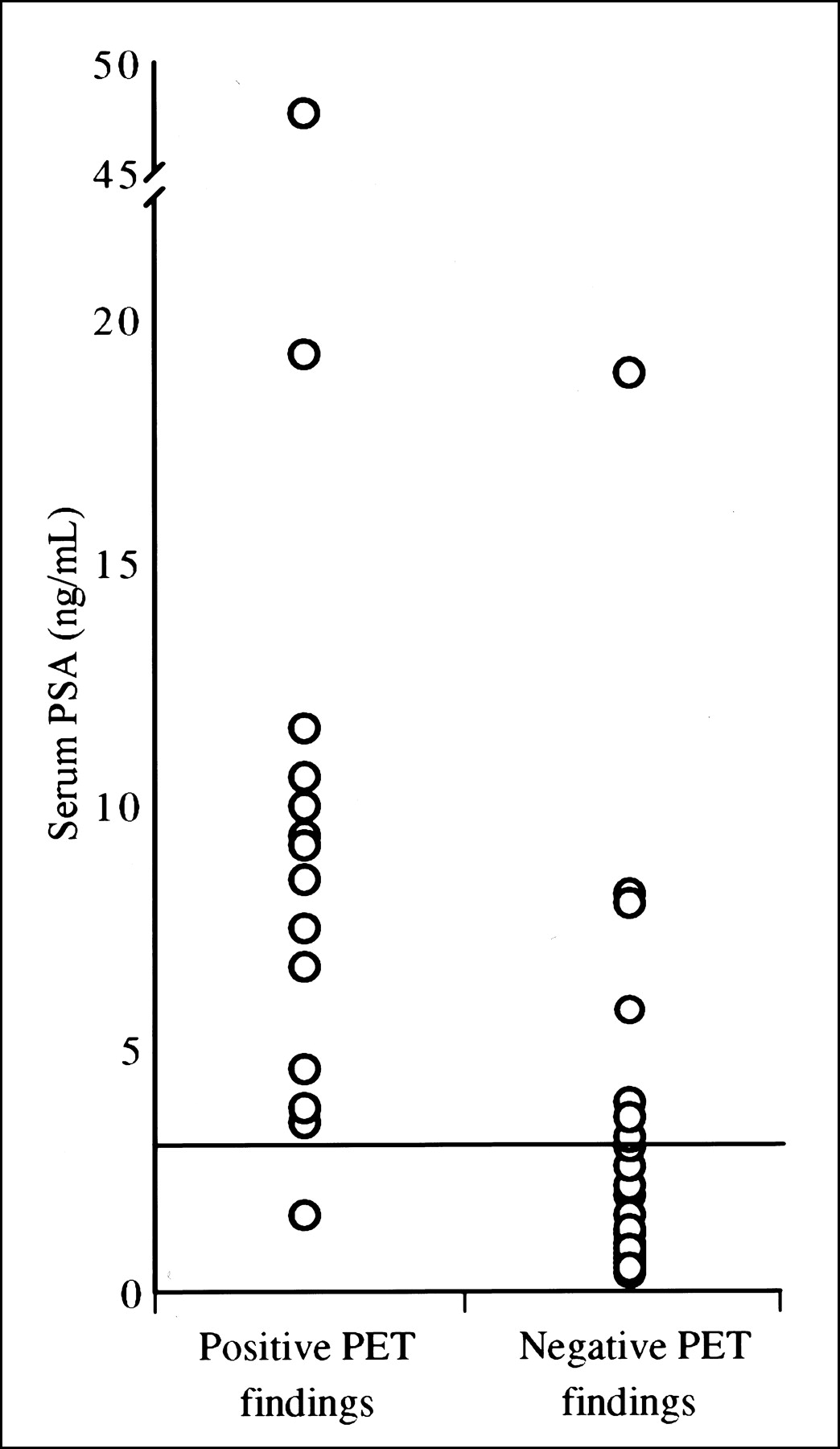
AC PET results are shown as function of PSA level. Thirteen of 22 patients with serum PSA level > 3 ng/mL had positive AC PET findings, whereas only 1 of 24 patients with serum PSA level ≤ 3 ng/mL had positive findings.
DISCUSSION
Patients with clinically localized prostate cancer are treated by radical prostatectomy or radiation therapy. However, it is reported that 21% of patients who receive initial treatment with definitive local therapy require further treatment because of recurrent disease (17). Monitoring of the serum PSA level is the most reliable way to detect early recurrence. Selection of appropriate therapy in these patients with PSA recurrence depends on whether the disease is localized or widespread. PSA velocity has been used to predict the site of recurrence (18,19). Analyzing the data from patients after radical prostatectomy, Partin et al. (18) reported that a PSA velocity of ≤0.75 ng/mL/y was seen in 94% of patients with local recurrence, whereas a PSA velocity > 0.75 ng/mL/y was present in 46% of patients with metastatic disease. In patients treated by radiation therapy, PSA velocity is less useful for prediction of recurrent disease, primarily because PSA is often detectable after radiation therapy (since the entire gland is not ablated). In these patients, PSA nadir is used to indicate recurrence, although the time to PSA nadir, approximately 27–42 mo, is too long to permit early detection.
Conventional imaging methods, such as CT and MRI, have been shown to be of little value in detecting recurrent lesions of prostate cancer (6). RIS with 111In-capromab pendetide has been used to detect prostate cancer. Murphy et al. performed RIS on 100 patients after failure of primary radical prostatectomy or radiation therapy (20). They found a high percentage of patients with persistent 111In-capromab pendetide uptake in the prostate bed (43%), as well as in regional nodes (20%) and distant nodes (32%). The sensitivity of RIS for detection of recurrent prostate cancer was also good, although the average PSA was 40.5 ng/mL, indicating a patient population with a high likelihood of extraprostatic disease.
Recently, PET using the radiopharmaceutical 11C-acetate has been introduced for imaging of tumors. Shreve et al. reported that renal cell carcinomas showed high uptake of 11C-acetate (21). AC PET also has high sensitivity for detection of prostate cancer (12, 13). The University of Michigan group studied 18 patients with rising PSA and evidence of local, recurrent, or regional metastatic disease by bone scintigraphy or CT (12). They showed AC PET to have high sensitivity for detecting primary tumors and nodal metastases. In a recent report from Japan, Oyama et al. performed AC PET on 22 patients with untreated prostate cancer, with positive findings in all patients (13). In both studies, prostatic cancer lesions exhibited moderately high uptake of 11C-acetate, greater than that of 18F-FDG. AC PET had higher sensitivity for detecting tumor than did 18F-FDG PET, without confounding bladder activity. Workers at the University of California at Los Angeles (6) and in Germany (22,23) have also reported favorable results with AC PET.
The mechanism of high 11C-acetate uptake in cancer tissue is uncertain but is thought to be different from that of myocardial uptake of this tracer. Yoshimoto et al. (24) studied the uptake of 14C-acetate in 4 different tumor cell lines and in a fibroblast cell line. They showed that 14C accumulation in each of the tumor cell lines was higher than that in fibroblasts, and they found that the accumulation in tumor cells was due to enhanced lipid synthesis. Given the highly active basal lipid metabolism in the cell membrane associated with tumor growth, 11C-acetate may be an important probe of this anabolic lipid pathway.
11C-choline (25,26) and 18F-fluoroethylcholine (27,28) have also been studied as possible radiopharmaceuticals for PET imaging in prostate cancer. These tracers are incorporated into cell membrane phospholipids, with uptake possibly increased by upregulation of choline kinase. Results of studies with these tracers in prostate cancer are encouraging, but only small numbers of patients have been evaluated. A disadvantage of 18F-fluoroethylcholine is its rapid excretion into urine, leading to significant bladder uptake that could potentially obscure disease in the prostate bed. Urinary excretion was not seen with AC PET in this study, although mild bladder-wall uptake was occasionally noted that did not interfere with image interpretation.
In this study, we evaluated 46 patients with PSA recurrence after radical prostatectomy or radiation therapy. Imaging findings indicating a high probability of recurrent prostate cancer were identified in 14 patients (30%) by AC PET, versus only 4 patients (9%) by 18F-FDG PET. Although the yield of AC PET is relatively low compared with that reported for RIS with 111In-capromab pendetide (20), there is a large difference in the serum PSA level among our patients (mean, 5.2 ng/mL) and those studied by Murphy et al. (mean, 40.5 ng/mL). Our study was designed to evaluate patients with AC PET as soon as PSA recurrence was recognized, at which time the PSA is relatively low. In such patients, there is a greater possibility that recurrent disease will be detected by imaging before it has spread to regional or distant lymph nodes or other organs, and there is thus a greater possibility for cure by salvage therapy.
PET may play a significant role in the management of patients with PSA recurrence after definitive local therapy. PET findings of distant metastases would lead to androgen ablation therapy or systemic chemotherapy rather than radiation therapy with its associated morbidity. In patients for whom radiation therapy is planned to treat local recurrence, positive PET findings would prompt further evaluation or alteration of the radiation fields. In patients whom the radiation oncologist is reluctant to treat because of an uncertain outlook for the patient, negative PET findings would increase confidence that radiation therapy is warranted because such treatment would more likely lead to a favorable outcome. In our study, 12 of 30 patients (40%) after radical prostatectomy were diagnosed to have lymph node metastases or bone metastases with high or intermediate probability using AC PET.
As reported here, AC PET has high sensitivity for detection of recurrent prostate cancer, and as reported elsewhere (13), AC PET has high sensitivity for identification of primary disease before therapy. However, a limitation of PET for early detection of disease is its relatively low spatial resolution of approximately 8 mm. As shown in Figure 4, we found that AC PET findings were positive in 59% of patients with a serum PSA level > 3 ng/mL but in only 4% of patients with a serum PSA level ≤ 3 ng/mL. It is known that the serum PSA level correlates with tumor volume in prostate cancer; hence, AC PET will be difficult in patients with low serum PSA levels.
A limitation of this study is that the majority of lesions found by PET were not confirmed by objective reference standards. Thus, some of the additional yield of AC PET could represent false-positive findings. Further studies are needed to accurately determine lesion-by-lesion and patient-by-patient sensitivity.
CONCLUSION
We evaluated AC PET for detection of prostate cancer recurrence. The results of our study demonstrated uptake in the prostate bed as well as in lymph nodes more often for 11C-acetate than for 18F-FDG. This study showed that 11C-acetate is a promising tracer for imaging patients with recurrent prostate cancer. Further studies with a larger number of patients and in different clinical settings will be necessary to determine its ultimate clinical utility.
Acknowledgments
The authors thank Helen Kaemmerer, Jennifer Frye, Linda Becker, and Lori Strong for their support with the PET imaging, and Sally Schwarz and other staff members of the Cyclotron Facility for supplying 11C-acetate and 18F-FDG. This study was supported by a research development award from the Siteman Cancer Center at Washington University and by a research award from the CaP CURE Foundation, Santa Monica, CA.
Footnotes
Received Jul. 15, 2002; revision accepted Sep. 25, 2002.
For correspondence or reprints contact: Tom R. Miller, MD, PhD, Mallinckrodt Institute of Radiology, Washington University School of Medicine, Campus Box 8223, 510 S. Kingshighway Blvd., St. Louis, MO 63110.
E-mail: MillerT{at}mir.wustl.edu
REFERENCES
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Detection Efficacy of 18F-PSMA-1007 PET/CT in 251 Patients with Biochemical Recurrence of Prostate Cancer After Radical Prostatectomy
- Metabolic Vulnerabilities of Prostate Cancer: Diagnostic and Therapeutic Opportunities
- Prospective Evaluation of 68Ga-RM2 PET/MRI in Patients with Biochemical Recurrence of Prostate Cancer and Negative Findings on Conventional Imaging
- Anatomic and Molecular Imaging in Prostate Cancer
- Evaluation of Prostate Cancer with 11C-Acetate PET/CT
- Bombesin-Targeted PET of Prostate Cancer
- Pilot Comparison of 68Ga-RM2 PET and 68Ga-PSMA-11 PET in Patients with Biochemically Recurrent Prostate Cancer
- Evaluation of Hybrid 68Ga-PSMA Ligand PET/CT in 248 Patients with Biochemical Recurrence After Radical Prostatectomy
- Dosimetry and First Clinical Evaluation of the New 18F-Radiolabeled Bombesin Analogue BAY 864367 in Patients with Prostate Cancer
- In Vivo Imaging of Prostate Cancer Using [68Ga]-Labeled Bombesin Analog BAY86-7548
- 11C-Acetate PET/CT Before Radical Prostatectomy: Nodal Staging and Treatment Failure Prediction
- An NMR Metabolomics Approach for the Diagnosis of Leptomeningeal Carcinomatosis
- 11C-Acetate PET/CT in Localized Prostate Cancer: A Study with MRI and Histopathologic Correlation
- Prostate Cancer: PET with 18F-FDG, 18F- or 11C-Acetate, and 18F- or 11C-Choline
- Functional Imaging of Localized Prostate Cancer Aggressiveness Using 11C-Acetate PET/CT and 1H-MR Spectroscopy
- Radiopharmaceuticals in Preclinical and Clinical Development for Monitoring of Therapy with PET
- Tumor Cell Metabolism Imaging
- Small-Cell Carcinoma of the Prostate
- 1-11C-Acetate Kinetics of Prostate Cancer
- 1-11C-Acetate as a PET Radiopharmaceutical for Imaging Fatty Acid Synthase Expression in Prostate Cancer
- The Role of Indium-111 Radioimmunoscintigraphy in Post-Radical Retropubic Prostatectomy Management of Prostate Cancer Patients
- 18F-Fluoroacetate: A Potential Acetate Analog for Prostate Tumor Imaging--In Vivo Evaluation of 18F-Fluoroacetate Versus 11C-Acetate
- Initial Experience with the Radiotracer Anti-1-Amino-3-18F-Fluorocyclobutane-1-Carboxylic Acid with PET/CT in Prostate Carcinoma
- 11C-Acetate Positron Emission Tomography Imaging and Image Fusion With Computed Tomography and Magnetic Resonance Imaging in Patients With Recurrent Prostate Cancer
- Parameters for Treatment Decisions for Salvage Radiation Therapy
- 2-[18F]Fluoro-2-Deoxyglucose Positron Emission Tomography for the Detection of Disease in Patients with Prostate-Specific Antigen Relapse after Radical Prostatectomy
- microPET and Autoradiographic Imaging of GRP Receptor Expression with 64Cu-DOTA-[Lys3]Bombesin in Human Prostate Adenocarcinoma Xenografts
- Radiation Dose Estimates in Humans for 11C-Acetate Whole-Body PET
- PET Imaging of Prostate Cancer with 11C-Acetate