


Abstract
Posttreatment surveillance for the recurrence of head and neck squamous cell carcinoma (HNSCC) is a diagnostic challenge. Tissue distortion from radiation and surgery can obscure early detection of recurrence by conventional follow-up approaches such as physical examination, CT, and MRI. Several studies have shown that 18F-FDG PET may be an effective technique for the detection of persistent, recurrent, and distant metastatic HNSCC after treatment. The aim of this prospective study was to determine the benefits of hybrid 18F-FDG PET/CT in detecting a subclinical locoregional recurrence of HNSCC and distant metastases. The study patients were considered cured of HNSCC on the basis of 12 mo of negative findings on conventional follow-up. We also assessed the diagnostic accuracy of 18F-FDG PET/CT in these patients. Methods: Ninety-one patients cured of HNSCC without any clinical evidence of recurrence were included. Whole-body 18F-FDG PET/CT examination was performed 11.6 ± 4.4 mo after the end of the treatment. The gold standard was histopathology or 6 mo of imaging follow-up. Results: The whole-body 18F-FDG PET/CT examinations had negative results in 52 patients and positive results in 39. Nine of these patients who exhibited abnormal 18F-FDG uptake in the head and neck area did not have recurrent HNSCC (false-positive). Thirty had proven recurrence. The sensitivity and specificity of 18F-FDG PET/CT in this study for the diagnosis of HNSCC recurrence were 100% (30/30) and 85% (52/61), respectively. The positive predictive value was 77% (30/39). The negative predictive value was 100% (52/52). The overall accuracy was 90% (82/91). Conclusion: The results of our study confirm the high effectiveness of 18F-FDG PET/CT in the assessment of HNSCC recurrence and suggest that 18F-FDG PET/CT is more accurate than conventional follow-up physical examination alone in the assessment of recurrence after previous curative treatment for HNSCC and could be proposed systematically at 12 mo of the usual follow-up.
Head and neck squamous cell carcinoma (HNSCC) is the eighth most common malignancy worldwide and refers to a group of malignancies involving the upper aerodigestive tract including the oral cavity, oropharynx, nasopharynx, hypopharynx, and larynx. Patients with head and neck tumors raise many diagnostic and therapeutic challenges. Their disease course is often complicated by recurrent disease, regional lymphatic spread, synchronous primary tumors, and distant metastases. Despite aggressive combined-modality treatment regimens, there remains a high rate (up to 40%) of locoregional recurrences (1). Moreover two thirds of locoregional recurrences and lymph node metastases occur within the first 2 y (2).
Posttreatment surveillance of HNSCC recurrence is a diagnostic challenge. Tissue distortion from radiation and surgery can obscure early detection of residual tumor and recurrence by the conventional follow-up approaches such as physical examination, CT, and MRI (3).
The usual follow-up consists of periodic standard examinations of the head and neck during the 5 y after treatment, including inspection and palpation of all anatomic subsites of the head and neck (oral cavity, nasopharynx, oropharynx, hypopharynx, and larynx) and examination of internal structures by a mirror and a flexible endoscope (4).
18F-FDG PET may be an effective technique for the detection of residual tumor recurrence and distant metastases after treatment. Through the identification of metabolic changes, clinicians may be able to overcome the limitations that posttreatment tissue changes bring to conventional anatomy-oriented surveillance.
Several retrospective (5–8) and prospective (9–11) studies have shown that 18F-FDG PET may be useful in detecting posttreatment recurrent HNSCC and be more effective than physical examination, CT, or MRI in doing so. However, in prior tumor recurrence studies, patients were commonly enrolled if recurrence was suspected. The advantage of a test that can detect subclinical recurrence was thereby unlikely to be demonstrated. We previously reported in a retrospective study (12) that 18F-FDG PET truly found unsuspected recurrence in 8 of 30 patients considered cured of HNSCC with negative findings on the usual follow-up.
The aim of this prospective study was to determine the benefits of hybrid 18F-FDG PET/CT in detecting a subclinical locoregional recurrence of HNSCC and distant metastases. The study patients were considered cured of HNSCC on the basis of 12 mo of negative findings on conventional follow-up. We also assessed the diagnostic accuracy of 18F-FDG PET/CT in these patients.
MATERIALS AND METHODS
Inclusion Criteria
All patients treated for histologically proven HNSCC from September 2005 to January 2008 at the University Hospital of Brest and at the Regional Hospital of Quimper and who did not show any findings suggestive of recurrence at 12 mo of their usual follow-up (consisting of a standard whole-body examination including inspection and palpation of all anatomic subsites of the head and neck [oral cavity, nasopharynx, oropharynx, hypopharynx and larynx] and an examination of internal structures by a mirror and a flexible endoscope) were included in the study. Patients with distant metastasis at the initial staging and with a previous history of recurrence were excluded.
Whole-Body 18F-FDG PET/CT
Scans were performed on a Gemini GXLi PET/CT scanner (Philips). Patients fasted 4 h before PET acquisitions, and the blood glucose level had to be less than 7 mmol/L before injection of 370 MBq (5 MBq/kg) of 18F-FDG. Intravenous injection was followed by a period of approximately 60 min when the patients remained in a quiet room. No muscle relaxants were administered. The patients were allowed to breathe normally during the PET and CT acquisitions. PET data were acquired in the 3-dimensional mode and, for attenuation correction, were reconstructed using CT data and a row-action maximum-likelihood iterative algorithm. The Gemini scanner consists of a 6-slice multi–detector-row spiral CT scanner with a transverse field of view of 600 mm. The CT parameters—a collimation of 6 × 5 mm, tube voltage of 120 kV, and effective tube current of 100 mAs—are standard for PET/CT studies and permit differentiation between tissues with good spatial resolution while ensuring that the patient does not receive a high radiation dose.
Image Interpretation
All 18F-FDG PET/CT images were interpreted qualitatively by 2 nuclear medicine physicians without prior knowledge of the follow-up status of these patients. Any initial difference of interpretation was resolved by consensus. For each 18F-FDG PET/CT scan report, the results were divided into 3 regions: primary, neck, and distant. The primary region included any sites along the aerodigestive tract from the nasal cavity and oral cavity to the trachea. The neck included the lymph node areas, soft tissues of the neck surrounding (but not including) the trachea, larynx cartilages, hyoid bone, and cervical spine. The distant regions included the brain, skeleton, thorax, mediastinum, and abdomen.
Outcome Determination and Data Analysis
18F-FDG PET/CT image findings were correlated with histopathology for locoregional findings and with radiography, CT, or MRI for distant findings. PET/CT findings of disease were considered true-positive if they correlated with histopathology findings positive for locoregional recurrence or with follow-up morphologic imaging findings positive for progression or distant metastasis. Each patient with negative 18F-FDG PET/CT results was seen clinically 6 mo after the PET/CT examination for the usual follow-up. Absence of evidence of recurrence at that time was considered a reference for determining that no true disease was present at the time of the 18F-FDG PET/CT examination.
The sensitivity, specificity, positive predictive value, negative predictive value, and overall accuracy of 18F-FDG PET/CT and the prevalence of malignancy in the asymptomatic patient sample were determined. The calculations were performed separately for each of the 3 anatomic regions (primary, neck, and distant), the head and neck region (primary and neck regions together), and the whole body (primary, neck, and distant regions together).
RESULTS
Ninety-one patients, 13 women and 78 men, with a mean age of 57.4 ± 9.4 y were included in the study. Patient characteristics and pathologic status are summarized in Table 1.
Patient and Disease Characteristics According to 18F-FDG PET/CT Results
The whole-body 18F-FDG PET/CT results were negative in 52 patients and positive in 39. For 30 of 39 patients with positive findings, recurrence was confirmed. Fourteen patients had only local recurrence (Fig. 1) (6 in the oral cavity, 1 in the hypopharynx, 6 in the oropharynx, and 1 in the laryngeal area); for 2, an associated cervical lymph node extension was confirmed by biopsy. Twelve had distant metastasis confirmed on the basis of progression seen on CT or histologically. Among them, 2 had both local recurrence confirmed by biopsy and distant metastases (1 in the oral cavity and 2 in the larynx, both with a lung metastasis) confirmed by CT, and 1 had local recurrence, a neck lymph node extension, and distant metastasis. For 17 patients, salvage surgery was performed; 10 patients underwent chemotherapy or palliative treatment; 2 patients refused therapy; and for 1 patient nothing was done. Nine of the 39 patients who exhibited abnormal 18F-FDG uptake in the laryngeal area did not have recurrent HNSCC despite many biopsies (false-positive; Figs. 2 and 3). The detailed results of these patients are shown in Table 2.
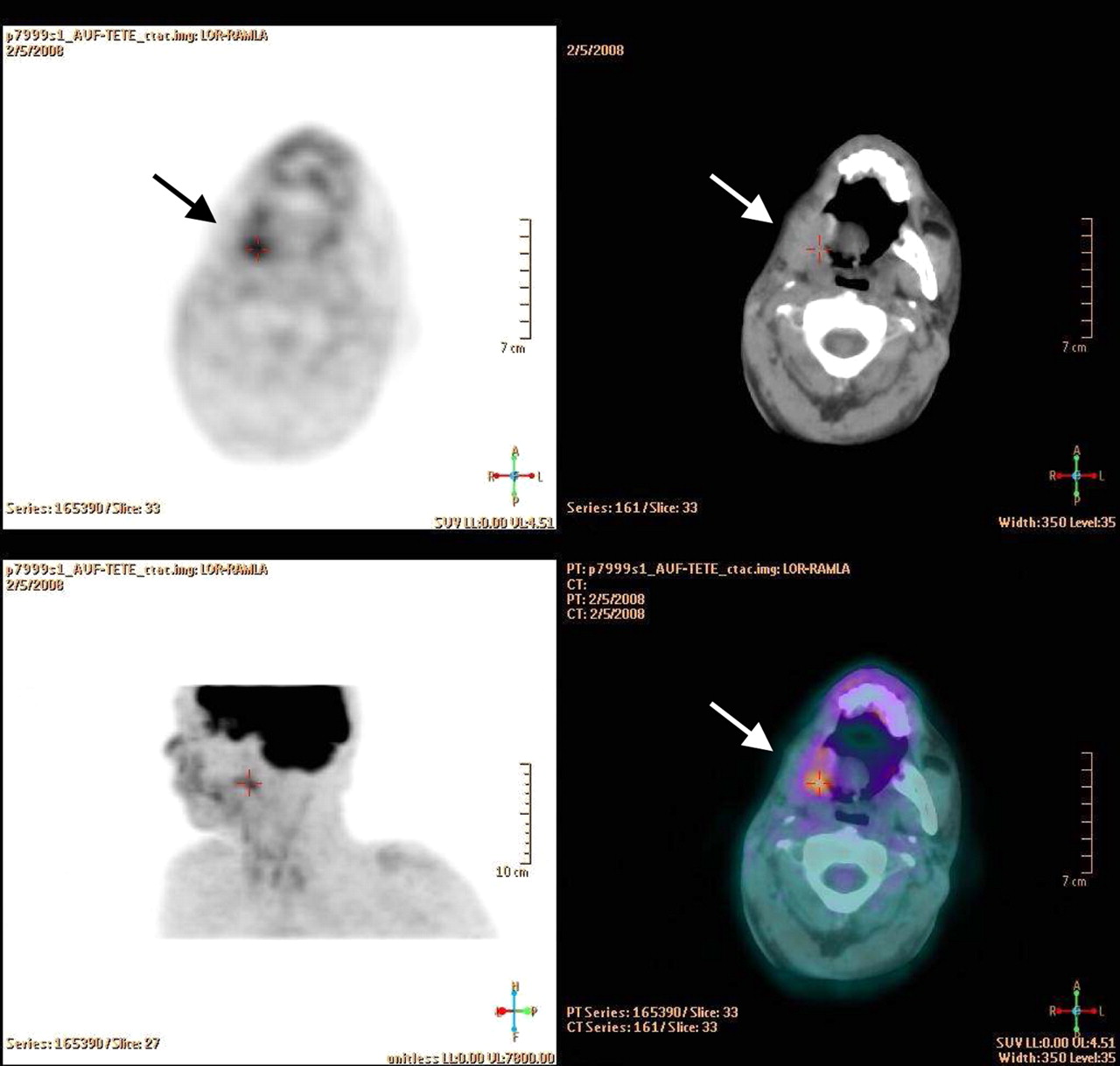
Transaxial 18F-FDG PET/CT images demonstrate true-positive focus (arrow) representing recurrent oral cavity carcinoma 12 mo after surgery.
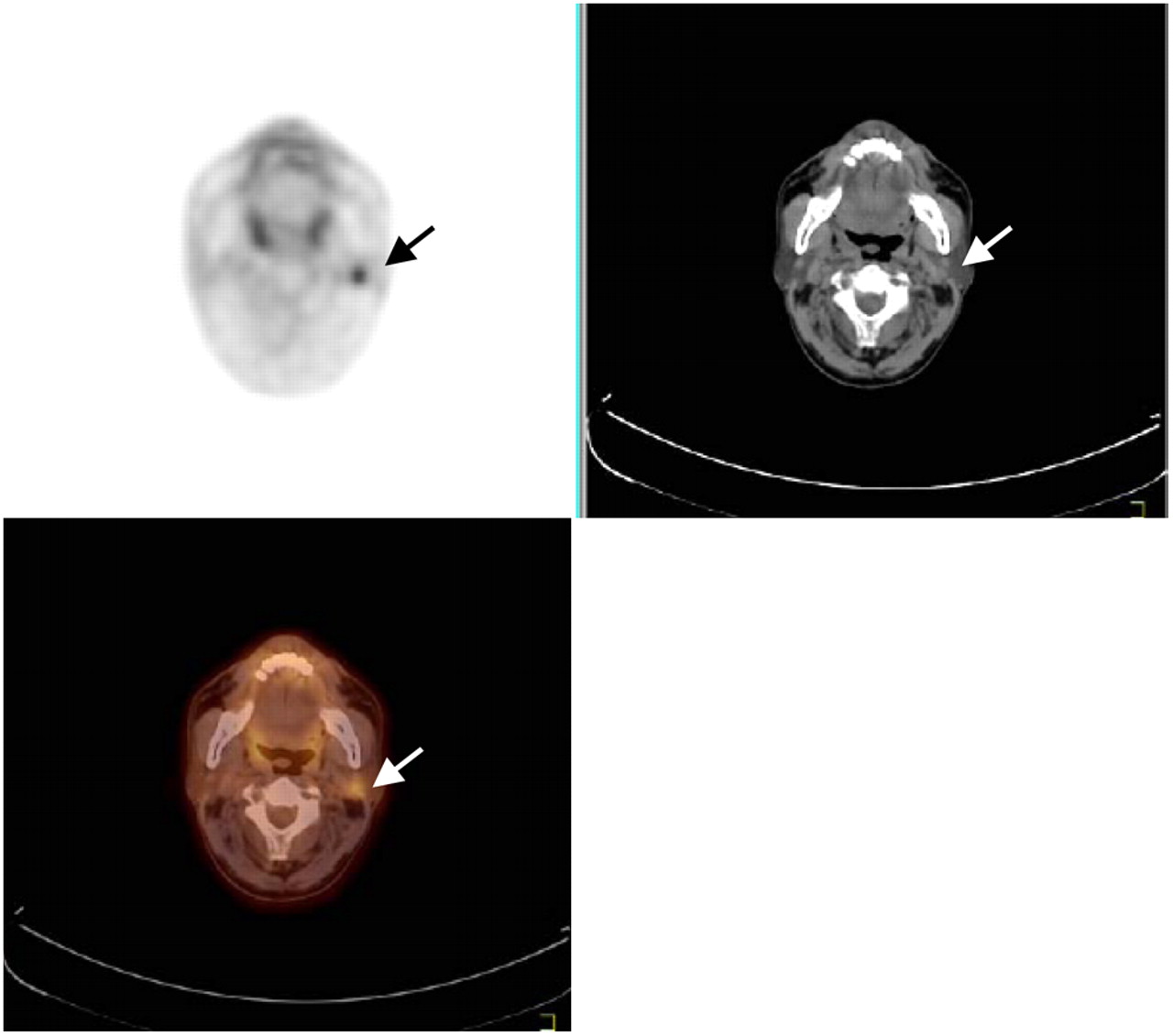
Transaxial 18F-FDG PET/CT images demonstrate false-positive focus (arrow) not confirmed by ultrasonography and follow-up of oral cavity carcinoma 12 mo after surgery.

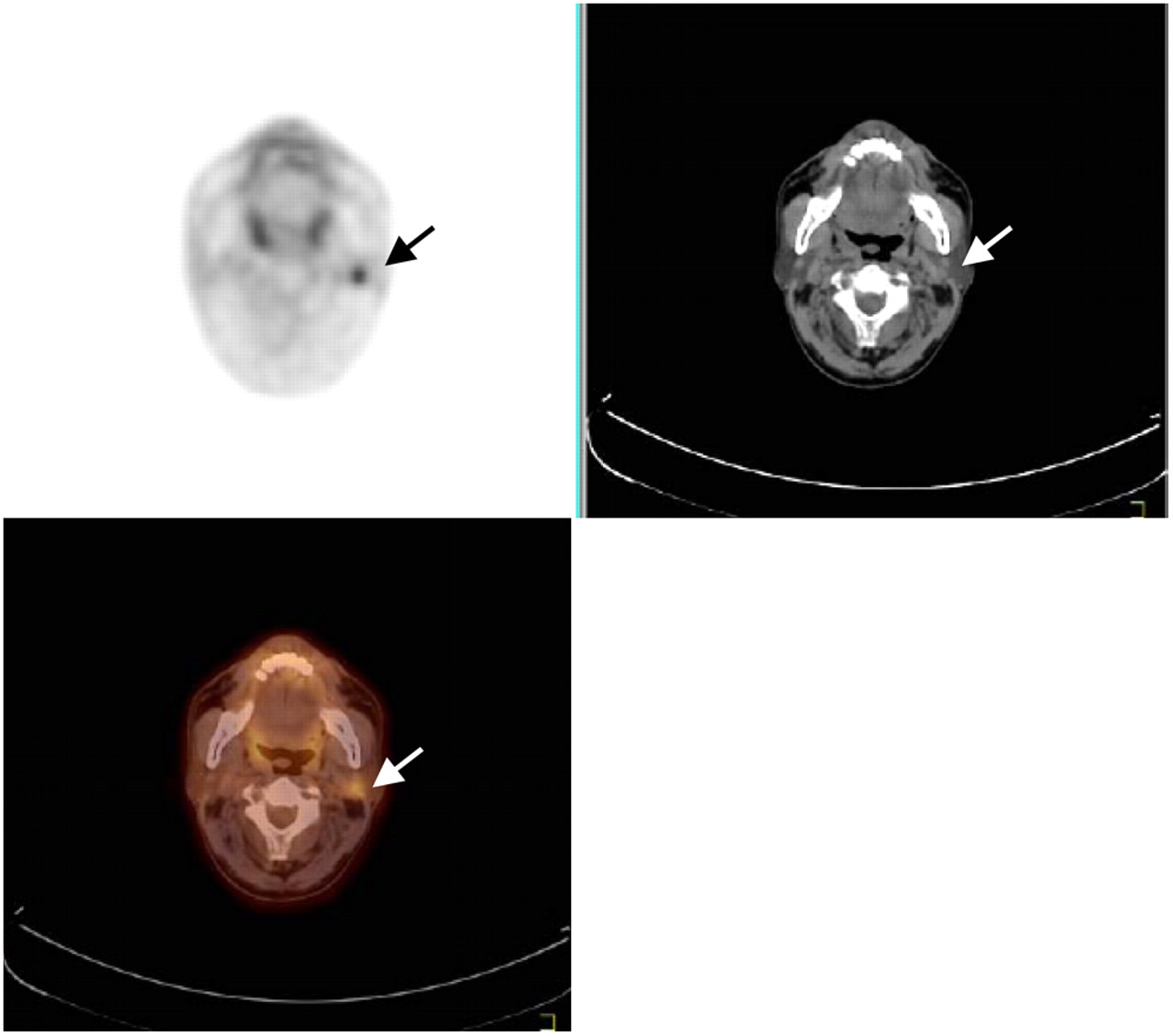
Transaxial 18F-FDG PET/CT images demonstrate false-positive focus (arrow) corresponding after biopsy to Bartonella henselae infection 12 mo after surgery and radiochemotherapy of oral cavity carcinoma.
Patients with Positive 18F-FDG PET/CT Data
All 52 patients with negative findings on18F-FDG PET/CT remained free of disease at 3 mo after each PET/CT examination, and for no one was evidence of malignancy on physical examination found during this period.
As shown in Table 3, the sensitivity and specificity of 18F-FDG PET/CT in this study for the diagnosis of HNSCC recurrence were 100% (30/30) and 85% (52/61), respectively. The positive predictive value was 77% (30/39). The negative predictive value was 100% (50/50). The overall accuracy was 90% (82/91).
Diagnostic Value of 18F-FDG PET/CT in Detection of Recurrence for 91 HNSCC Asymptomatic Patients
DISCUSSION
A delay in the detection of recurrent HNSCC has been shown to be deleterious to clinical outcome after treatment. Patients with recurrent, early-stage HNSCC who undergo salvage surgery have a 70% 2-y relapse-free survival, whereas those with recurrent, advanced-stage HNSCC undergoing surgical salvage have just a 22% 2-y relapse-free survival (13). Early diagnosis and accurate identification of recurrent HNSCC are therefore critically important for successful treatment. Sequential physical examinations are generally accepted for posttherapy follow-up of patients with head and neck cancer. The National Comprehensive Cancer Network panel suggests a general consensus surveillance schedule: physical examination every 1–3 mo during the first year, every 2–4 mo during the second year, every 4–6 mo during the next 3 y, and every 6–12 mo thereafter (14,15). However, physical examination can be compromised by granulation, fibrosis, tissue edema, and necrosis. 18F-FDG PET can identify viable tumor on the basis of higher glycolytic rates in neoplasm than in necrotic or reactive tissues (16).
Our study showed that 18F-FDG PET/CT is a useful tool in detecting recurrent HNSCC during posttreatment surveillance despite negative findings on follow-up physical examinations. In addition to its ability to detect the presence of locoregional disease in these patients, 18F-FDG PET/CT provided significant additional information. Thirty of 91 patients had a proven recurrence that was not discovered by the usual sequential physical examinations. This high level of recurrence agrees with the usual recurrence rates (>30% during the first 3 y (4,17), even in asymptomatic patients (18)). The study suggests an earlier detection of the recurrence that probably will be found later during the usual follow-up. For 9 patients, 18F-FDG PET/CT had positive results despite the absence of recurrent disease. These patients probably had local inflammation, and one had mandibular osteoradionecrosis, which is known to cause false-positive results. This is in agreement with many studies that have proven the need to delay imaging after the end of radiotherapy to minimize persistent inflammatory changes (19,20). Moreover, false-positive results may occur with 18F-FDG PET because of infections; physiologically increased uptake in structures such as the palatine tonsils and salivary glands (salivary gland cancers are typically not 18F-FDG–avid) and the masticator, oral cavity, neck, and laryngeal muscles; uptake in reactive nonneoplastic lymph nodes; uptake after surgery; and uptake in noninfectious inflammation and granulation at the surgical site (flare phenomenon). Uptake in muscles may be asymmetric and is usually due to anxiety, with laryngeal and masticator activity after 18F-FDG injection. Coregistered images with 18F-FDG PET/CT allow a direct correlation between 18F-FDG uptake and anatomic structures, thus reducing false-positive results. Attenuation-correction artifacts result from erroneous overcorrection of PET emission data by software that uses CT transmission data for attenuation correction. These artifacts occur in areas that have a high attenuation on corresponding CT images (e.g., metallic implants) but can usually be detected by evaluating the uncorrected emission 18F-FDG PET data (21).
When the results of 18F-FDG PET are negative, the likelihood of recurrent malignancy is low (at least at 6 mo of follow-up), but it should not underestimate a possible false-negative, as when malignancy is present in structures with a physiologically elevated metabolism (e.g., tonsillar carcinoma), when the tumor is smaller than the resolution of current PET/CT scanners (typically 10 mm for PET scanners), or when the tumor is not 18F-FDG–avid. Therefore, careful surveillance and continued follow-up are still probably needed in those patients with a high risk of recurrence (21). A negative predictive value of 100% gives clinical confidence that a false-negative result is unlikely. Moreover, with a sensitivity of 100%, if malignancy is present, 18F-FDG PET will produce positive findings. Nevertheless, with a specificity of 85%, unnecessary explorations are performed in less than 15%.
Few other studies have evaluated other imaging modalities such as CT and MRI in such treated and asymptomatic patients. However, in a recent review of trials evaluating PET for detecting residual or recurrent HNSCC in undifferentiated patients treated by radiotherapy or chemoradiotherapy, among 27 of 1,871 identified studies the pooled sensitivity and specificity of PET for detecting residual or recurrent HNSCC were 94% and 82%, respectively, whereas the CT mean pooled sensitivity and specificity were lower (67% and 78%, respectively), as were the sensitivity and specificity of MRI (81% and 46%, respectively) (22). In another recent review of 21 articles comparing 18F-FDG PET, CT, and MRI for the diagnosis of local residual or recurrent nasopharyngeal carcinoma, the pooled sensitivity estimates for PET (95%) were significantly higher than those for CT (76%) (P < 0.001) or MRI (78%) (P < 0.001) and the pooled specificity estimates for PET (90%) were significantly higher than those for CT (59%) (P < 0.001) or MRI (76%) (P < 0.001) (23). Moreover, in a prospective study comparing 18F-FDG PET, CT, and MRI for the initial evaluation of 134 oral SCC patients with a palpably negative neck, Ng et al. found 18F-FDG PET to have a sensitivity 2-fold higher than CT or MRI in the detection of nodal metastases (41.2% vs. 21.6%, respectively; P = 0.021) (24). These data confirm the possible superiority of PET in detecting asymptomatic recurrences.
Several posttreatment studies found 18F-FDG PET to have a similar accuracy for the detection of locoregional and distant recurrence of HNSSC. In these studies, sensitivities ranged from 92% to 100%, specificities from 64% to 100%, PPVs from 64% to 100%, NPVs from 92% to 100%, and overall accuracy from 88% to 91% (5–11). The lowest specificities are explained by false-positive findings in irradiated regions within 6 mo after therapy. Radiotherapy-induced inflammatory processes may lead to a transient increase in 18F-FDG uptake (25). In our study, the specificity was high because we performed, as proposed by Greven et al., the 18F-FDG PET at least 3 mo after the completion of treatment (26). However, in the recurrence studies, patients were commonly enrolled if recurrence was suspected. Lowe et al. and Ryan et al. have shown that 18F-FDG PET may be useful, too, in asymptomatic patients (18,27). Our results confirmed these data and the conclusion of our preliminary study (12).
CONCLUSION
The results of our study confirmed the high effectiveness of 18F-FDG PET/CT in assessing for recurrence of HNSCC in patients who have been considered cured of the disease. Our findings suggest that 18F-FDG PET/CT is more accurate than conventional follow-up physical examinations alone in such patients. The systematic use of PET/CT at 12 mo of the usual follow-up could be proposed, but cost-effectiveness and an evaluation of the survival impact remain to be evaluated.
Footnotes
-
COPYRIGHT © 2009 by the Society of Nuclear Medicine, Inc.
References
- Received for publication July 9, 2008.
- Accepted for publication September 16, 2008.





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Preliminary Results from Retrospective Correlation of Circulating Tumor DNA (ct-DNA) with Imaging for HPV-Positive Oropharyngeal Squamous Cell Carcinoma
- Diagnostic Performance of 18F-FDG PET/CT According to Delay After Treatment to Detect Subclinical Recurrence of Head and Neck Squamous Cell Carcinoma
- PET/CT Versus Standard Imaging for Prediction of Survival in Patients with Recurrent Head and Neck Squamous Cell Carcinoma
- Guideline Familiarity Predicts Variation in Self-Reported Use of Routine Surveillance PET/CT by Physicians Who Treat Head and Neck Cancer
- Head and Neck Cancers, Version 2.2014
- Osteoradionecrosis after Radiation Therapy for Head and Neck Cancer: Differentiation from Recurrent Disease with CT and PET/CT Imaging
- PET/CT Imaging and Human Papilloma Virus-Positive Oropharyngeal Squamous Cell Cancer: Evolving Clinical Imaging Paradigm
- Addition of 18F-FDG PET/CT to Clinical Assessment Predicts Overall Survival in HNSCC: A Retrospective Analysis with Follow-up for 12 Years
- Early Detection of Recurrent Disease by FDG-PET/CT Leads to Management Changes in Patients With Squamous Cell Cancer of the Head and Neck
- The Lack of Evidence for PET or PET/CT Surveillance of Patients with Treated Lymphoma, Colorectal Cancer, and Head and Neck Cancer: A Systematic Review
- Performance of Whole-Body PET/CT for the Detection of Distant Malignancies in Various Cancers: A Systematic Review and Meta-Analysis
- The role of positron emission tomography/CT imaging in head and neck cancer patients after radical chemoradiotherapy
- Head and Neck Cancers
- Innovations in Radiotherapy Planning of Head and Neck Cancers: Role of PET
- 18F-FDG PET as a Routine Posttreatment Surveillance Tool in Oral and Oropharyngeal Squamous Cell Carcinoma: A ProspectiveStudy