Article Text

Abstract
Background Contrast-enhanced ultrasound (CE-US), contrast CT scan and gadolinium dynamic MRI are recommended for the characterisation of liver nodules detected during surveillance of patients with cirrhosis with US.
Aim To assess the sensitivity, specificity, diagnostic accuracy and economic impact of all possible sequential combinations of contrast imaging techniques in patients with cirrhosis with 1–2 cm liver nodules undergoing US surveillance.
Patients/methods 64 patients with 67 de novo liver nodules (55 with a size of 1–2 cm) were consecutively examined by CE-US, CT, MRI, and a fine-needle biopsy (FNB) as diagnostic standard. Undiagnosed nodules were re-biopsied; non-malignant nodules underwent enhanced imaging follow-up. The typical radiological feature of hepatocellular carcinoma (HCC) was arterial phase hypervascularisation followed by portal/venous phase washout.
Results HCC was diagnosed in 44 (66%) nodules (2, <1 cm; 34, 1–2 cm; 8, >2 cm). The sensitivity of CE-US, CT and MRI for 1–2 cm HCC was 26, 44 and 44%, with 100% specificity, the typical vascular pattern of HCC being identified in 22 (65%) by a single technique versus 12 (35%) by at least two techniques carried out at the same time point (p=0.028). Compared with the cheapest dual examination (CE-US+CT), the cheapest single technique of stepwise imaging diagnosis of HCC was equally expensive (€26 440 vs €28 667), but led to a 23% reduction of FNB procedures (p=0.031).
Conclusions In patients with cirrhosis with a 1–2 cm nodule detected during surveillance, a single imaging technique showing a typical contrast pattern confidently permits the diagnosis of HCC, thereby reducing the need for FNB examinations.
- Cirrhosis
- hepatocellular carcinoma
- imaging technique
- screening
Statistics from Altmetric.com
Introduction
The treatment outcome of hepatocellular carcinoma (HCC) has significantly improved following standardisation of surveillance with abdominal ultrasound (US) of patients at risk, owing to an increased detection of small, potentially curable tumours confined to the liver.1–5 According to the American Association for the Study of the Liver Diseases (AASLD),3 contrast enhanced-US (CE-US), CT scan and gadolinium dynamic MRI allow for the correct classification of a liver nodule detected during surveillance, with a predicted sensitivity and specificity of >89% and 95%, respectively.5 6 While HCC can be confidently diagnosed in >2 cm nodules by a single contrast technique showing early arterial hypervascularisation and portal/venous washout, two imaging techniques at the same time point are required to achieve the diagnosis of nodules <2 cm, leaving either a US-guided fine needle biopsy (FNB) or repeat examinations with imaging techniques at strict intervals necessary for nodules with discrepant contrast imaging results.3 To date, there is no established priority and sequence of imaging techniques to be applied in the evaluation of liver nodules, although the aforementioned radiological procedures differ in terms of applicability and cost, and may impact on treatment outcome depending on their diagnostic accuracy. Using explanted livers as a diagnostic gold standard, MRI appeared to be more accurate than CT scan for the diagnosis and staging of small HCC nodules,7–10 while in one study the combined application of CE-US and gadolinium MRI showed absolute specificity for 0.5–2 cm liver nodules; however, at the expense of sensitivity.11 In another study, the combination of CE-US and CT scan resulted in high rates of specificity; however, leaving the issue of diagnostic accuracy unsolved.12 Unfortunately, there are no studies in patients with cirrhosis that prospectively assess the diagnostic accuracy and the economic impact of contrast imaging techniques in any combination in the evaluation of 1–2 cm nodules detected during surveillance. In the present study, we evaluated these aspects of the recall policy in comparison with the performance of the AASLD algorithm. A secondary end point was to assess the diagnostic performance and economic costs of all possible sequential combinations of the three contrast imaging techniques.
Patients and methods
This is an independent investigator-driven, prospective study designed to assess the diagnostic accuracy of CE-US, CT and MRI in the evaluation of liver nodules detected in patients with compensated cirrhosis under surveillance with US. Starting in April 2006, all patients with a Child–Pugh A or B cirrhosis and a de novo liver nodule detected during US surveillance were consecutively included. Excluded were patients with a pre-existing nodule, poor liver function (Child–Pugh C) indicating liver transplantation independently of HCC, or an echo-coarse US pattern of the liver without a well-defined nodule. Surveillance with US was performed at 6-month intervals by two experienced echographists (MF and SM) in all patients who gave informed consent in the presence of an independent witness. Patient evaluation included a detailed medical history, a physical examination, complete blood count and biochemical tests, including serum alpha-fetoprotein (AFP) and markers for viral hepatitis and autoimmunity. In all patients, examinations with abdominal CT scan, MRI, CE-US and US-guided FNB were carried out within 2 months from detection of a liver nodule.
Characterisation of the liver nodules
The diagnostic gold standard was histology through an FNB performed within the nodule and the surrounding liver parenchyma. The procedure was repeated in all patients with unsolved histological diagnosis—ie, patients showing similar histological features within and outside the liver nodule. All patients with nodules lacking histological features of malignancy underwent a repeat US every 3 months and an abdominal CT/MRI every 6 months to assess changes in size and in the vascular pattern of the nodule at imaging. All nodules either enlarging or showing changes in the vascular pattern underwent a further FNB.
Definition of the vascular pattern of the nodules
Arterial hypervascularisation was seen as an increased contrast enhancement of the nodule (hyperechogenicity on US, hyperdensity on CT and hyperintensity on MRI), taking place during the arterial phase of examination, as compared with the surrounding liver parenchyma. Portal/venous contrast washout was seen as a hypoenhanced pattern of the nodule (hypoechogenicity on US, hypodensity on CT and hypointensity on MRI) with respect to the surrounding liver parenchyma taking place during the portal/venous phase. The typical radiological pattern of HCC was arterial hypervascularisation followed by portal/venous contrast washout of the nodule.
Liver histology
The FNB procedure was performed using a 21-gauge trenchant needle for microhistology (Biomol, HS Hospital Service, Italy) to examine both intranodule and extranodule liver parenchyma tissue. The diagnosis was made according to the International Working Party criteria.13 Formalin-fixed paraffin-embedded liver sections were examined by an experienced liver pathologist (GR) who was unaware of the result of the clinical and radiological examinations. The hospital reimbursement of a FNB procedure was €236, including the histological report and the cost of day-hospital admission.
MRI
MRI was performed with a 1.5 T system (Avanto, Siemens Medical Systems, Erlangen, Germany) using a phased-array torso coil for signal detection. All patients underwent transverse T1-weighted and T2-weighted MRI and multiphasic contrast-enhanced dynamic 3-dimensional MRI of the whole liver with fat suppression. T1-weighted imaging included breath-hold in-phase gradient echo (175/5 resolution time (TR)/echo time (TE), 256×112 matrix, 70° flip angle) and out-of-phase gradient echo (175/2.38 TR/TE, 256×112 matrix, 70° flip angle). T2-weighted imaging included fat suppression sequences (1310/70 TR/TE, 320×192 matrix). Dynamic MRI was performed with a 3-dimensional volumetric interpolated breath-hold examination (VIBE) sequence in the axial plane by using the following parameters: 4.7/2.3, 10° flip angle, 320×157 matrix, slice thickness of 3 mm. Gadolinium (gadobenate dimeglutamine 0.5 mmol/l, Multihance, Bracco, Milan, Italy) was injected at a dose of 0.2 ml/kg at a rate of 2 ml/s. Arterial phase, portal venous and delayed venous phase images were acquired ∼30, 80 and 180 s from the start of contrast injection, respectively. A breath-hold T1-weighted 2-dimensional gradient echo with fat suppression MRI (4.7/2.3 TR/TE, 256×157 matrix) and 3-dimensional VIBE sequences were performed 2 h after contrast injection (hepatocyte phase). Images were read blindly by one experienced radiologist (LVF) unaware of the liver biopsy results. The National Health System reimbursement of an abdominal contrast-enhanced MRI examination was €265.
CT scan
CT scan was performed with a 64-multidetector row CT (MDCT; Definition Siemens, Erlangen, Germany), 2.5 mm slice thickness, rotation time 0.5 s. A 1.5 mg/kg dose of iodinated contrast medium (Iomeron 400, Bracco, Milan, Italy) was injected with a 4.0 ml/s flow. In all patients, the acquisition time from the start of contrast injection and the start of acquisition sequences was 40 s for the arterial phase, 80 s for the portal venous phase and after 180 s for the delayed phase. Patients with an unsatisfactory acquisition of the arterial phase were to repeat the exam using the bolus tracking technique. Images were read blindly by one experienced radiologist (LVF) who was unaware of the liver biopsy results. The reimbursement of an abdominal contrast-enhanced CT scan examination was €168.
CE-US
US studies were performed with a Philips iU22 system (Philips Ultrasound, Bothell, Washington, USA), using a multifrequency (5–2 MHz) convex transducer (C5-2). A preliminary grey-scale US examination of the upper abdomen was performed. On identifying the nodule, CE-US was performed with up to two bolus injections of 2.4 ml of second-generation contrast agent (SonoVue, Bracco, Milan, Italy), having 8 μm microbubbles and stability for 6–8 min. The bolus was followed by a 10 ml saline flush. A low mechanical index (MI <0.1) was set for CE-US examination. Enhancement patterns were studied during the vascular phase for up to 3 min, including the arterial (0–35 s), portal (35–120 s) and late phase (120–180 s). The typical vascular pattern of HCC on CE-US is characterised by hyperenhancing in the arterial phase, followed by washout in the portal/venous phase.14 15 All examinations were obtained and evaluated in real time by two expert echographists (MF and SM) and digitally stored and documented by a commercially available system or videotapes. Patients with a discrepant result were re-evaluated in a dedicated reading session by the two echographists, who were unaware of the liver biopsy results. The reimbursement of a CE-US examination was €78, including the cost of contrast.
Routine chemistries
Patients were classified according to the following nosological categories for the cause of cirrhosis: (1) hepatitis B virus—this category only included patients with a positive serum test for hepatitis B surface antigen; (2) hepatitis C virus (HCV)—patients positive only for the antibody to hepatitis C virus and HCV RNA; (3) alcohol abuse—only those with a daily intake of >60 g of ethanol in women or >80 g in men, for >10 years; (4) multiple causes—this category included patients with a combination of two or more of the above factors and patients with hepatitis delta virus (HDV); and (5) other causes—all patients with none of the above factors. Routine exams included serum AFP performed within 2 weeks from enrolment in the study (AFP, immunoradiometric assay (IRMA), Abbott, North Chicago, Illinois, USA; normal, ≤20 ng/ml).
Diagnosis modality and cost analysis of the diagnostic procedures
The cost of the diagnostic procedures was calculated by the Italian National Health System charges, adding up the cost of each procedure performed to obtain the final diagnosis. The cost of all possible sequential algorithms of examinations and combinations of diagnostic procedures was stratified by nodule size. The diagnosis modality and cost assessment of diagnosis of 1–2 cm nodules were done as follows: (1) since the AASLD endorses two contrast imaging techniques for the diagnosis of HCC, the costs were calculated for each possible pair of exams among the three techniques available, the third imaging procedure being calculated only in patients with discordant results. The incremental cost of FNB was calculated only in patients lacking a matching typical vascular pattern with two imaging techniques. We calculated the aggregate and per patient mean cost of the radiological and histological procedures for all patients who underwent examination to obtain a final diagnosis of the liver nodule. (2) The diagnosis of HCC and related costs were also calculated considering the possibility of obtaining the diagnosis of HCC by a single imaging technique showing the typical vascular pattern, considering additional techniques and FNB only in the case of an unsolved diagnosis. Costs were calculated for all possible technique combinations. The costs for a final diagnosis with each possible combination of imaging techniques were calculated and compared.
Statistical analysis
The baseline characteristics of the patients are expressed as median and range or count and proportion. Comparison of patients with a HCC nodule and patients with non-HCC nodules was done by the Student t test or the Mann–Whitney test for continuous variables, and Fisher exact test for categorical variables. Cost analyses of imaging techniques and FNB were compared by Student t test. A conventional p value <0.05 was considered statistically significant. Calculations were done with the Stata 10.0 statistical package (Stata, College Station, Texas, USA).
Results
Diagnosis of the liver nodules
Sixty-nine patients had abnormal findings at US, that is a defined liver nodule or a coarse pattern of liver parenchyma. Five (7%) with a coarse echo pattern of the liver with no defined liver nodule were excluded. Sixty-four patients were shown to have a total of 67 liver nodules (table 1). Liver nodules size ranged from 0.8 to 2.7 cm (mean 1.6 cm) in size. Two (3%) were <1 cm, 55 (82%) were 1–2 cm in size and 10 (15%) were >2 cm. By histology, 44 (66%) nodules were classified as HCC, 2 (3%) as cholangiocarcinomas (CCCs) and 21 (31%) as either macroregenerative nodules (MRNs) or low grade dysplastic nodules (LGDNs) (table 2). Patients with MRNs or LGDNs had repeated imaging techniques during a median of 18 months (range 6–32) to exclude HCC. HCC and non-HCC nodules were similar in terms of patient age, aetiology, routine laboratory parameters and size, but not for AFP, which was higher in the former patients (17 ng/ml vs 6 ng/ml, p=0.002). At baseline US, three patients had two nodules, including one with two LGDNs, and two with an HCC and an MRN. An FNB was successfully carried out in all patients, including two out of 44 with a final diagnosis of HCC, who showed histological features similar within and outside the nodule at first biopsy, who required a repeat FNB, corresponding to a total of 5% false-negative results at the first biopsy.
Demography of patients with compensated cirrhosis and a de novo liver nodule detected during surveillance with abdominal ultrasound
Final diagnosis of the liver nodules detected during surveillance stratified by size
De novo 1–2 cm liver nodules
Radiological investigations
Table 3 shows the vascular pattern of 1–2 cm liver nodules with each imaging technique. Two patients with an HCC could not undergo MRI because of claustrophobia and a metallic plate in the skeleton, respectively. Nine nodules (26%) had the typical vascular pattern of HCC demonstrated by CE-US, 16 (47%) by CT and 14 (44%) by MRI. None of the nodules histologically classified as non-HCC had the typical vascular pattern of HCC. Table 4 shows the sensitivity, specificity, positive and negative predictive values and likelihood ratios of the arterial hypervascular pattern, portal/venous washout and typical vascular pattern for each imaging technique in patients with 1–2 cm nodule. Figure 1A–C reports the HCC typical vascular pattern detected by CE-US, CT and MRI in the same patient. Combining two imaging techniques, the sensitivity of CE-US+CT, CE-US+MRI and CT+MRI was 21, 18 and 26%, respectively. The rates of positive findings with two coincidental techniques in patients with 1–2 cm liver nodules showed the comparable sensitivity, specificity and accuracy of the three imaging techniques either alone or in combination. In 1–2 cm nodules, the typical radiological vascular pattern for HCC was more often obtained by CT and MRI alone than by combined CE-US+MRI (p=0.027 and p=0.031, respectively) or CE-US+CT (p=0.038 and p=0.043, respectively). Table 5 shows the rates of typical vascular pattern of HCC by US, CT and MRI in patients with 1–2 cm liver nodules. In 11 patients, 13 additional nodules that were missed by US were subsequently detected by either CT scan or MRI. All these nodules were 1–2 cm in size: three of these nodules showed the typical HCC vascular pattern by either MRI+CT (n=1) or MRI alone (n=2), and were histologically classified as HCC as soon as the nodules became detectable by enhanced follow-up with US, and could therefore be investigated by an FNB. The remaining eight patients had 10 nodules lacking the typical HCC vascular pattern at MRI (n=8) and CT scan (n=6): these nodules showed similar sizes and vascular patterns and remained undetected by US during 18 (6–32) months of follow-up. While the rates of benign liver nodules did not change during follow-up, additional tumour nodules were detected in other segments of the liver in three patients with a single HCC, 2–3 months after initial tumour detection.
Vascular pattern in 55 nodules of 1–2 cm including 34 HCCs
Rates of sensitivity and specificity of arterial hypervascularisation, portal vein washout in the late venous phase and typical vascular pattern for the diagnosis of 34 HCCs detected in 55 patients with 1–2 cm nodules

{kind=link}
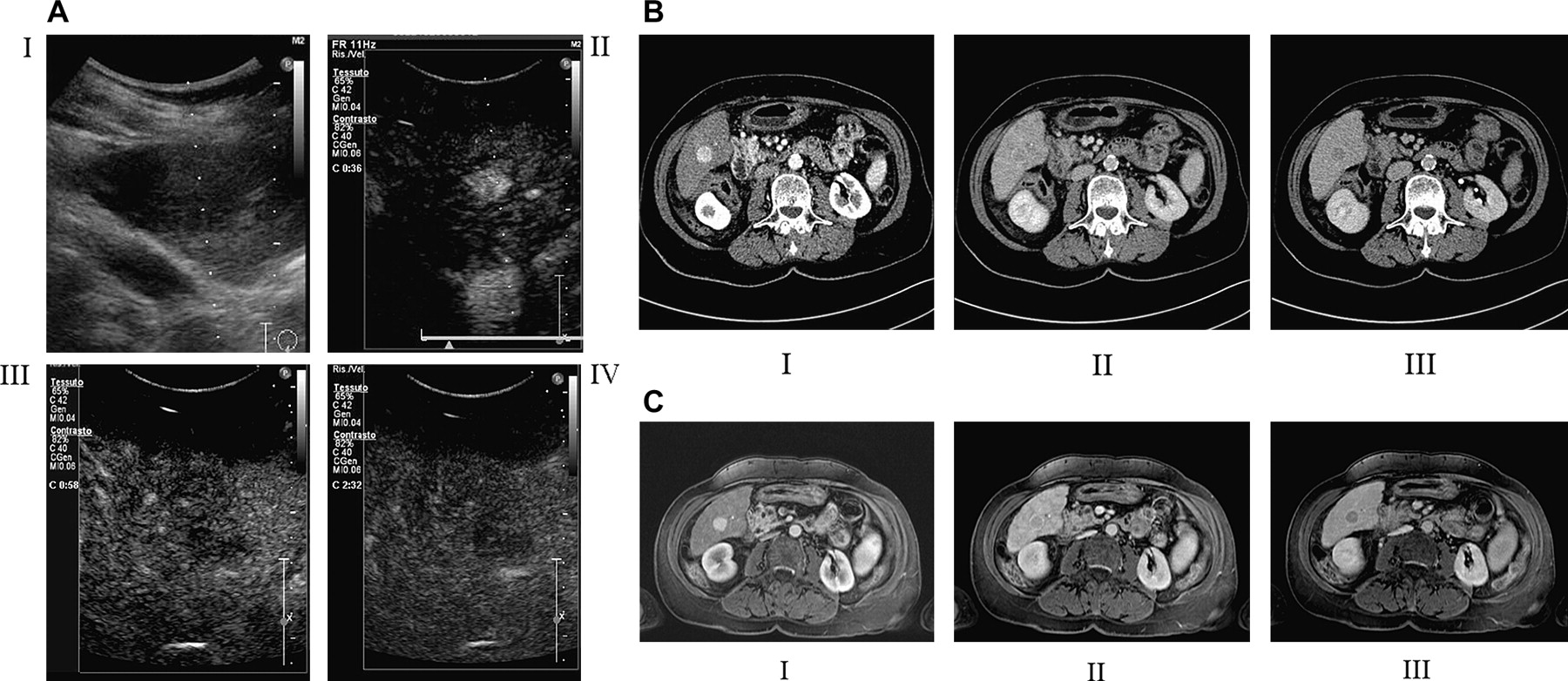
The typical contrast behaviour on imaging in a hepatocellular carcinoma (HCC) nodule. The same patient examined by: (A) contrast-enhanced ultraound (CE-US): preliminary grey-scale US examination of the nodule (I), arterial hypervascularisation of the liver nodule (II) followed by washout in the portal/venous (III) and late phase (IV). (B) CT scan: arterial hypervascularisation of the liver nodule (I), followed by washout in the portal/venous (II) and late phase (III). (C) MRI: arterial hypervascularisation of the liver nodule (I), followed by washout in the portal/venous (II) and late phase (III).
Rates of typical vascular pattern at each imaging technique at examination with combined techniques
Diagnostic performance
Among 44 patients with an HCC nodule, 20 (45%) fulfilled the AASLD criteria for radiological diagnosis of HCC, including 12 (35%) with a 1–2 cm nodule. The eight HCC nodules >2 cm were all correctly identified by at least one imaging technique, with absolute specificity. Among the 34 patients with a 1–2 cm HCC nodule, 22 (65%) had the typical HCC pattern detected by at least a single radiological technique compared with 12 (35%) who were diagnosed by AASLD criteria—that is, by at least two concordant imaging techniques (p=0.028). In the latter scenario, 43 (78%) patients with 1–2 cm nodules required an FNB to obtain the final diagnosis whereas in the single imaging technique scenario the diagnosis of HCC required an FNB in 33 (55%) patients only (p=0.031).
Cost analysis
Table 6 shows the aggregate and per patient cost estimates referred to the Italian National Health System for the diagnosis of 1–2 cm liver nodules, after stratification for all the possible combinations of the radiological investigations. According to AASLD criteria, CE-US+CT followed by MRI and FNB in the case of unsolved diagnosis was the cheapest combination to obtain the diagnosis of HCC (table 6). Considering the diagnosis of HCC made by a single imaging technique showing a typical vascular pattern, the cost was similar for any possible sequence of imaging technique, the cheapest being CE-US followed by CT, MRI and FNB (table 6). This sequence had comparable cost to the cheapest sequence obtained applying the AASLD criteria.
Model representing the number and the estimated aggregate and per patient cost of the radiological and histological procedures utilised for the assessment of the 55 nodules 1–2 cm in size in 54 patients with cirrhosis, stratified by the different diagnostic protocols based on different sequences of investigations
Discussion
This is the first study to compare prospectively the sensitivity, specificity and diagnostic accuracy of the three leading imaging techniques endorsed by the AASLD for the radiological diagnosis of a small HCC in patients with cirrhosis. Based on the prospective and consecutive evaluation of all patients with a de novo liver nodule detected during surveillance with US, the study compared the accuracy of the imaging investigations according to the nodule size, with a specific focus on those of 1–2 cm in size. Interestingly, the rates of de novo HCC nodules in patients with cirrhosis under surveillance were similar to those reported in previous studies, while the study confirmed that HCC is the most common (66%) cause of de novo liver nodules in these patients.7 11 12 We acknowledge that the low prevalence (7%) of multinodular HCC in our cohort reflects the exclusion of patients with a coarse echo pattern of the liver, the use of a last-generation US scan and the involvement of expert dedicated hepatologists who are skilful at US scanning after long training periods.16
As expected, the vast majority (82%) of liver nodules detected by surveillance ranged between 1 and 2 cm in size, and therefore were difficult to diagnose according to AASLD radiological criteria, since two-thirds of the HCCs of this size will have either discrepant results with two imaging techniques or a lack of typical vascular pattern of HCC in both.11 With all the caveats due to the limited sample size of the study, CT scan and MRI had comparable sensitivity for the typical vascular pattern of HCC in 1–2 cm nodules (44% and 44%), whereas CE-US had appreciably, though not significantly, lower sensitivity (26%), as previously suggested by others.11 More challenging is a study in China that showed remarkably high diagnostic sensitivity of both CE-US and CT scan in patients with tumours <2 cm (91% and 81%, respectively).17 In that study, however, the background aetiology of cirrhosis was mainly hepatitis B (vs HCV and alcohol in the Western studies), and patients with a coarse echo pattern of the liver, who are at high risk of false-positive results with imaging, were not excluded as we did in our study.
In our patients with 1–2 cm HCCs, the three possible dual combinations of CE-US, CT scan and MRI showing a concordant vascular pattern for HCC had absolute specificity but low (18–26%) sensitivity. Our findings roughly reproduce the results of a prospective study with CE-US+MRI of patients with a liver nodule detected during surveillance, which, however, also included nodules <1 cm in size.11 Interestingly, we also demonstrated each independent technique to have absolute specificity for 1–2 cm HCC nodules, probably reflecting the strict criteria we adopted in the evaluation of the nodule vascularity and in the process of patient selection. We acknowledge, however, that MRI was somehow less applicable than CT scan, as two patients were excluded from MRI examination because of claustrophobia and a bone metallic plate, respectively.
If validated in a larger series of patients, our algorithm based on a single contrast imaging technique would probably make the management of patients with a 1–2 cm HCC nodule easier. The use of a single radiological examination of 1–2 cm nodules showing both early arterial and late portal/venous vascular changes is appealing, since it reduces the need for FNB procedures for the final diagnosis of HCC, without affecting the sensitivity and specificity rates of the recall policy. In fact, using a single contrast imaging technique an FNB was applied to 33 patients with a 1–2 cm nodule compared with 43 patients in the AASLD scenario of two imaging techniques at the same time point, with a total saving of 23% of FNB procedures. Although such a single technique “algorithm” showed absolute specificity for 1–2 cm HCC nodules, we acknowledge that both the diagnostic accuracy and cost–benefit ratios of the single imaging approach need to be validated prospectively for applicability, taking into account the different costs in each country. The AASLD algorithm for 1–2 cm HCCs also carries a substantial risk of false-negative radiological diagnosis, as indicated by the extra numbers of FNB procedures required to obtain a final diagnosis of HCC in patients with a radiologically unsolved diagnosis compared with the single technique approach. In a validation study of the original EASL (European Association for the Study of the Liver) criteria for the diagnosis of HCC, 56% of the 1–2 cm nodules showed arterial hypervascularisation only,18 which compares favourably with our rates of 78% based on the more stringent AASLD criteria of combined arterial hypervascularisation and portal washout. In our study, the numbers of false-negative results by imaging techniques in 1–2 cm nodules could be minimised by the comparative examinations of core biopsies and peritumoural tissue as well as by the use of the microhistological trenchant 21-gauge needles, endowed with better diagnostic performances compared with thinner needles. The latter, in fact, are reported to carry a significant risk (30%) of a false-negative diagnosis of HCC in small nodules detected during surveillance.11
As expected, the clinical benefit of investigations with contrast imaging techniques such as CT or MRI in patients with a liver nodule detected by US went far beyond the recall policy, since contrast imaging was able to detect additional nodules that escaped recognition by US. By CT scan and MRI, 19% more nodules were identified compared with US, including three HCC nodules.
In summary: (1) HCC is the most common diagnosis for de novo liver nodules detected during US surveillance of patients with cirrhosis; (2) in 1–2 cm nodules, the typical vascular pattern with the imaging techniques has absolute specificity for HCC; and (3) the radiological diagnosis by a single imaging technique showing the typical vascular pattern significantly reduces the need for FNB investigations (p=0.031) as compared with AASLD guidelines which require two techniques carried out at the same time point showing the typical vascular pattern for HCC, without modifying the costs calculated on the basis of the Italian National Health System.
In conclusion, our diagnostic algorithm allows for confident identification of patients with cirrhosis with a de novo 1–2 cm HCC detected during US surveillance by means of one contrast imaging procedure showing the typical HCC vascular pattern, with a significant saving of invasive FNB procedures and no increase in costs.
Significance of this study
What is already known about this subject?
The EASL and AASLD endorse a similar protocol for the diagnosis of small HCC in patients with cirrhosis under surveillance.
In patients with cirrhosis with 1–2 cm liver nodules, the diagnosis of HCC requires either echo-guided histological examination by FNB or two contrast imaging exams providing the typical vascular pattern of HCC—that is, hypervascularisation in the arterial phase with washout in the portal/venous phase. The contrast imaging technique of choice are CE-US, CT, and dynamic MRI.
Since the radiological diagnosis of 1–2 cm HCC is possible in a minority of cases, FNB examination still has an important role in the diagnosis of HCC.
What are the new findings?
The study provides head-to-head comparative figures of sensitivity, specificity and accuracy of CE-US, CT and MRI for the diagnosis of 1–2 cm HCC. Specificity was absolute for all the imaging techniques whenever nodules show the typical vascular pattern of HCC.
The application of a single contrast imaging technique provided figures of sensitivity for nodules of 1–2 cm that were similar to those provided by two contrast imaging techniques according to the AASLD, however, with a significant saving in terms of invasive liver biopsy procedures.
The sequential application of CE-US, CT, MRI and FNB to obtain a final diagnosis of HCC is the cheapest stepwise diagnostic sequence of all possible combinations and as expensive as the CE-US plus CT followed by MRI and FNB, according to the AASLD.
How might this study impact on clinical practice in the forseeable future?
The proposed diagnostic algorithm in patients with 1–2 cm liver nodules should increase safety without increasing the cost of HCC diagnosis.
Acknowledgments
The authors thank Caterina M Puricelli for her expert secretarial assistance, and Professor Giorgio Rossi for his help in the management of the patients.
References
Footnotes
Linked articles 203257.
Funding The present study was supported by grant no. PUR 2008, University of Milan, and by a generous contribution from Dr Aldo Antognozzi.
Competing interests None.
Ethics approval This study was conducted with the approval of the Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico Milan.
Provenance and peer review Not commissioned; externally peer reviewed.