Article Text

Abstract
Background: Neuropathological studies have reported varying amounts of amyloid pathology in dementia with Lewy bodies (DLB) and Parkinson’s disease dementia (PDD). [11C]PIB positron emission tomography (PET) is a marker of brain amyloid deposition. The aim of this study was to quantify in vivo amyloid load in DLB and PDD compared with control subjects and subjects with Parkinson’s disease (PD) without dementia.
Methods: 13 DLB, 12 PDD, 10 PD subjects and 41 age matched controls (55–82 years) were recruited. Each subject underwent clinical evaluation, neuropsychological assessment, T1 and T2 MRI, and [11C]PIB PET. The amyloid load was estimated from 60–90’ target region:cerebellar [11C]PIB uptake ratios. Object maps were created by segmenting individual MRIs and convolving them with a probabilistic atlas. Cortical [11C]PIB uptake was assessed by region of interest analysis.
Results: The DLB cohort showed a significant increase in mean brain [11C]PIB uptake and individually 11 of the 13 subjects with DLB had a significantly increased amyloid load. In contrast, mean [11C]PIB uptake was normal for the PDD group although two of 12 patients with PDD individually showed a raised amyloid load. Where significant increases in [11C]PIB uptake were found, it was increased in cortical association areas, cingulate and striatum. None of the subjects with PD showed significantly raised cortical [11C]PIB uptake.
Conclusion: This study suggests that amyloid load is significantly raised in over 80% of subjects with DLB, while amyloid pathology is infrequent in PDD. These in vivo PET findings suggest that the presence of amyloid in DLB could contribute to the rapid progression of dementia in this condition and that anti-amyloid strategies may be relevant.
Statistics from Altmetric.com
Parkinson’s disease (PD) is the second most common neurodegenerative disorder, affecting approximately 1% of the population over the age of 60 years. It is associated with bradykinesia, rigidity and rest tremor but a significant number of patients with PD also develop either mild cognitive impairment or frank dementia. The reported prevalence of dementia in PD varies from 4% to 93%, averaging around 40%.1 2 PD is associated with a sixfold higher risk of developing dementia compared with healthy age matched controls.
The dementia associated with PD is characterised by impairment of short term recall, attention, visuospatial and executive functions such as decision making. Unlike Alzheimer’s disease (AD), language and praxis are relatively preserved although fluency of speech and language can be reduced. In addition to cognitive impairment, patients with PD can manifest personality and behavioural changes along with fluctuating confusion and visual hallucinosis. The pathophysiological basis of the cognitive impairment and dementia in PD is probably multifactorial.1 Possibilities include the presence of cortical Lewy bodies, concomitant Alzheimer amyloid plaque (Aβ) and tangle pathology, degeneration of subcortical nuclei including the dopaminergic medial substantia nigra, the cholinergic nucleus basalis of Meynert, the noradrenergic locus coeruleus and serotonergic median raphe, along with other brainstem nuclei, or a combination of all of these processes. The presence of Aβ has occasionally been reported in idiopathic PD3 although this is more commonly a feature in patients with PD who have developed later dementia (PDD).4–6
Dementia with Lewy bodies (DLB) is the second most prevalent neurodegenerative dementia and its clinical diagnosis is based on revised “consensus” criteria.7 The central feature essential for the diagnosis of DLB is dementia—defined as progressive cognitive decline of sufficient magnitude to interfere with normal social or occupational function. Prominent or persistent memory impairment may not necessarily occur in the early stages but is usually evident with progression. Deficits on tests of attention, executive function and visuospatial ability may be especially prominent. The core features to make a diagnosis of DLB are (1) fluctuating cognition with pronounced variations in attention and alertness; (2) recurrent visual hallucinations that are typically well formed and detailed; and (3) spontaneous features of parkinsonism.7 Two of three core features are sufficient to make a diagnosis of probable DLB and one core feature to make a diagnosis of possible DLB. Onset of the above dementia syndrome should occur before or within 12 months of parkinsonism.
Consensus clinical diagnostic criteria for PDD have been published recently.8 The core features of PDD are a diagnosis of PD according to the UK Brain Bank criteria followed by a dementia syndrome, 1 or more years later with insidious onset, slow progression and impairment in more than one domain, representing a decline from the premorbid level and deficits severe enough to impair daily life.
The pathological diagnosis of DLB requires demonstration of cortical Lewy bodies, and its staging is determined by the density and distribution of these inclusions although in reality this staging correlates only weakly with severity or duration of dementia during life.9 10 In addition to Lewy body pathology, a significant number of patients with DLB have shown concomitant AD pathology (amyloid plaques and neurofibrillary tangles) at post mortem11 12 and many meet the CERAD (Consortium to Establish a Registry for Alzheimer’s Disease13) criteria for AD. It has also been reported that the majority of subjects with DLB show significant amyloid deposition in the striatum.14
In contrast, cortical Aβ is less frequently seen in patients with PDD.3 15 Neuropathological studies by Ballard et al noted that 66% of patients with DLB had significant amyloid pathology compared with 22% of subjects with PDD.16 It appears that the longer the duration of PD prior to onset of dementia the less severe the cortical alpha-synuclein pathology and the lower the CERAD plaque scores that are found at post mortem.16 In PDD, alpha-synuclein rather than Alzheimer pathology is most likely to determine the severity of the dementia.6
Until recently, we were unable to measure in vivo amyloid load in dementia but radiotracer markers are now available. In AD the positron emission tomography (PET) thioflavin based radiotracer [11C]PIB [N-methyl-[11-C]2-(4′-methyl amino phenyl)-6-hydroxy benzothiazole], binds to the Aβ deposits found as plaques in the cortex and more diffusely in striatum.17 Patients with AD have now been widely studied with [11C]PIB PET and twofold increases in cortical uptake of this radiotracer have been reported compared with healthy controls.18–27 The metabolic pathway of beta-amyloid has become an important therapeutic target in AD28–30 and similar treatments could be applicable to PDD and DLB if it were possible to demonstrate in vivo the presence of a raised amyloid load in these conditions.
In this current [11C]PIB PET study, our intention was to assess in vivo the regional cerebral amyloid load in patients with PDD and DLB and to compare this with non-demented PD and age matched healthy control subjects. We hypothesised that amyloid pathology would be uncommon in PD without dementia, an occasional feature of PDD and present in the majority of DLB cases.
METHODS
Subjects were recruited from the Hammersmith Hospitals, Kings College Hospital and Lewisham Hospital Trusts, London, UK; Austin Health, University of Melbourne, Australia; and the University Hospital of Turku, Finland. Thirteen subjects with DLB (10 from Melbourne, three from Turku), 12 subjects with PDD (six from London and six from Turku), 10 subjects with PD without dementia (seven from London and three from Turku) and 41 age matched healthy control subjects (17 from London, 12 from Melbourne and 12 from Turku ) had [11C]PIB PET. The 10 patients with DLB from Melbourne were scanned in a previous study examining beta-amyloid loads in aging and dementia.31 Six additional healthy controls who were found to have increased [11C]PIB uptake were not included in our study as its aim was to examine patterns of raised [11C]PIB distribution in DLB, PDD and PD. Diagnosis of DLB was based on the revised consensus criteria for DLB7 while diagnosis of PDD was based on the diagnostic algorithm for PDD,32 where patients had a diagnosis of PD for at least 1 year before the onset of dementia. All subjects had detailed neurological assessments, including taking a history from a close relative, examination and routine blood analysis. They also had detailed neuropsychometry including a Mini-Mental State Examination (MMSE),33 and specific tests of immediate and delayed verbal and visual memory, attention, executive functions, verbal fluency, naming and visuoconstruction.
Other inclusion criteria for patients were: (1) age 55–82 years, (2) clinical diagnosis of DLB, PDD or PD without dementia before they enrolled in the study, (3) adequate visual and auditory acuity to complete the psychological testing, (4) a reliable caregiver who could provide information about the patient’s clinical symptoms and (5) ability to provide informed consent. Exclusion criteria were the presence of: (1) extensive white matter microvascular disease on MRI which, in the opinion of a consultant radiologist, was over and above the few lacunes associated with normal aging, (2) major depression based on DSM-1V criteria, (3) a current or recent history of drug or alcohol abuse/dependence, (4) any significant disease or unstable medical condition that could influence neuropsychological testing, (5) pregnancy, (6) participants in whom MRI was contraindicated, (7) a history of schizophrenia, schizoaffective disorder, bipolar disorder or any history of ECT and (8) history of cancer within the past 5 years except localised skin and prostate cancer. Dementia was excluded in control subjects by detailed clinical examination and neuropsychometric tests. Permission to perform the study was obtained from the relevant ethics committees and regulatory bodies.
MRI
All subjects had T1 weighted volumetric MRI for co-registration of anatomical structures and T2 weighted MRI to exclude the presence of significant white matter disease.
[11C]PIB-PET
[11C]PIB was manufactured by: (1) Hammersmith Imanet, GE Healthcare, at the Cyclotron Building, Hammersmith Hospital; (2) the Centre for PET, Austin Health, Melbourne and (3) The Turku PET Centre, Finland. Subjects and controls were scanned using a Siemens ECAT EXACT HR+ scanner (London, UK),34 Phillips Allegro whole-body PET scanner (Melbourne, Australia)35 and a GE Advance scanner (Turku, Finland). Transmission scans were performed to measure tissue attenuation of 511 keV radiation. Dynamic emission scans were acquired in three-dimensional mode. All subjects had an intravenous bolus injection of [11C]PIB. The mean injected dose was 370 (±25) MBq and mean specific activity of 20235 (±6240) MBq/μmol. PET emission scans were acquired over 90 min. All data processing and image reconstruction was performed using standard software which included scatter correction.
Analysis of [11C]PIB-PET data
Creation of object maps
This was performed centrally for all scan data by one centre (Hammersmith Imanet). We used statistical parametric mapping software (SPM99; Wellcome Department of Imaging Neuroscience, UCL, London, UK; http:www.fil.ion.ucl.ac.uk/spm) to perform the following image preprocessing steps. MRIs were segmented into grey matter, white matter and CSF, and the grey matter images were thresholded at 50% probability. These grey matter images were then spatially transformed into MNI space. We convolved this binarised grey matter map with the latest version of a probabilistic brain atlas36 to create individualised object maps.
Target region to cerebellum ratios (RATIO)
The target region to cerebellar [11C]PIB uptake ratio image was created by dividing the integral 60–90 min tracer uptake image by the integral 60–90 min uptake value of cerebellar grey matter. Initially, a 60–90 min uptake image was created by integrating the activity collected from 60–90 min in Matlab 6. This image was coregistered to the individual’s MRI using SPM 99. This coregistered image was then spatially transformed into the MNI space. Cerebellar tracer uptake was then calculated by sampling the 60–90 min image using the cerebellar grey matter object map in Analyze AVW 6.1. The 60–90 min image was then divided by the cerebellar uptake value to create a 60–90 min ratio (RATIO) image using image calculator in Analyze AVW 6.1. Target to cerebellar ratios at these later times provide a blood flow independent measure of [11C]PIB retention that is easy to calculate, and rests on minimal assumptions and does not require arterial sampling. This approach has been previously validated.37 38 We then sampled [11C]PIB uptake RATIO images using Analyze AVW 6.1 in the following regions: frontal, temporal and parietal association cortices, anterior and posterior cingulate gyrus, striatum and thalamus.
Statistical parametric mapping (SPM)
Clusters of significant differences in mean 60–90 min [11C]PIB region:cerebellar uptake ratios for 13 patients with DLB compared with control subjects were localised at a voxel level using SPM99. Variance introduced by the sites of scanning was estimated using sites as linear factors. Spatially normalised RATIO images were interrogated using a voxel threshold of p<0.001 with an extent threshold of 100 voxels to detect significant change without normalising global [11C]PIB-uptake with ANCOVA or proportional scaling.
Statistical analysis
Statistical interrogations of ROI data were performed using SPSS for Windows V.14 (SPSS, Chicago, Illinois, USA). When comparing individual data against the control mean, each subject was compared against the control from the same site. Values outside control mean +2 SDs were taken as statistically significant. We calculated the percentage increase for individual subjects using the following formula:
((Rp − Rmc) × 100) / Rmc
where Rp denotes RATIO for individual subjects and Rmc denotes the mean of the control in the corresponding site. Since we combined the data from the three sites, control data from individual sites were compared to see whether they were comparable.
RESULTS
Table 1 shows the demographic characteristics of the subjects and table 2 outlines the mean [11C]PIB uptake in the DLB, PDD, PD and control groups.
Individually, 11 of the 13 patients with DLB had significantly increased (>2 SD) amyloid load in one or more cortical regions compared with the corresponding control mean from the relevant centre. Nine of the 13 subjects with DLB had [11C]PIB levels in the AD range (an [11C]PIB uptake RATIO >1.5) in either the anterior or posterior cingulate gyrus and/or cortical regions. Two of the 13 subjects with DLB had [11C]PIB uptake similar to that of control subjects. These two subjects were not taking any medications to improve their cognition and both fulfilled consensus criteria for DLB. One of these subjects with DLB who had no raised [11C]PIB uptake had been diagnosed for 7 years, had an MMSE of 26 and a Clinical Dementia Rating score of 1, while the other subject had been diagnosed with DLB for 8 years, had an MMSE of 20 and a Clinical Dementia Rating score of 2.
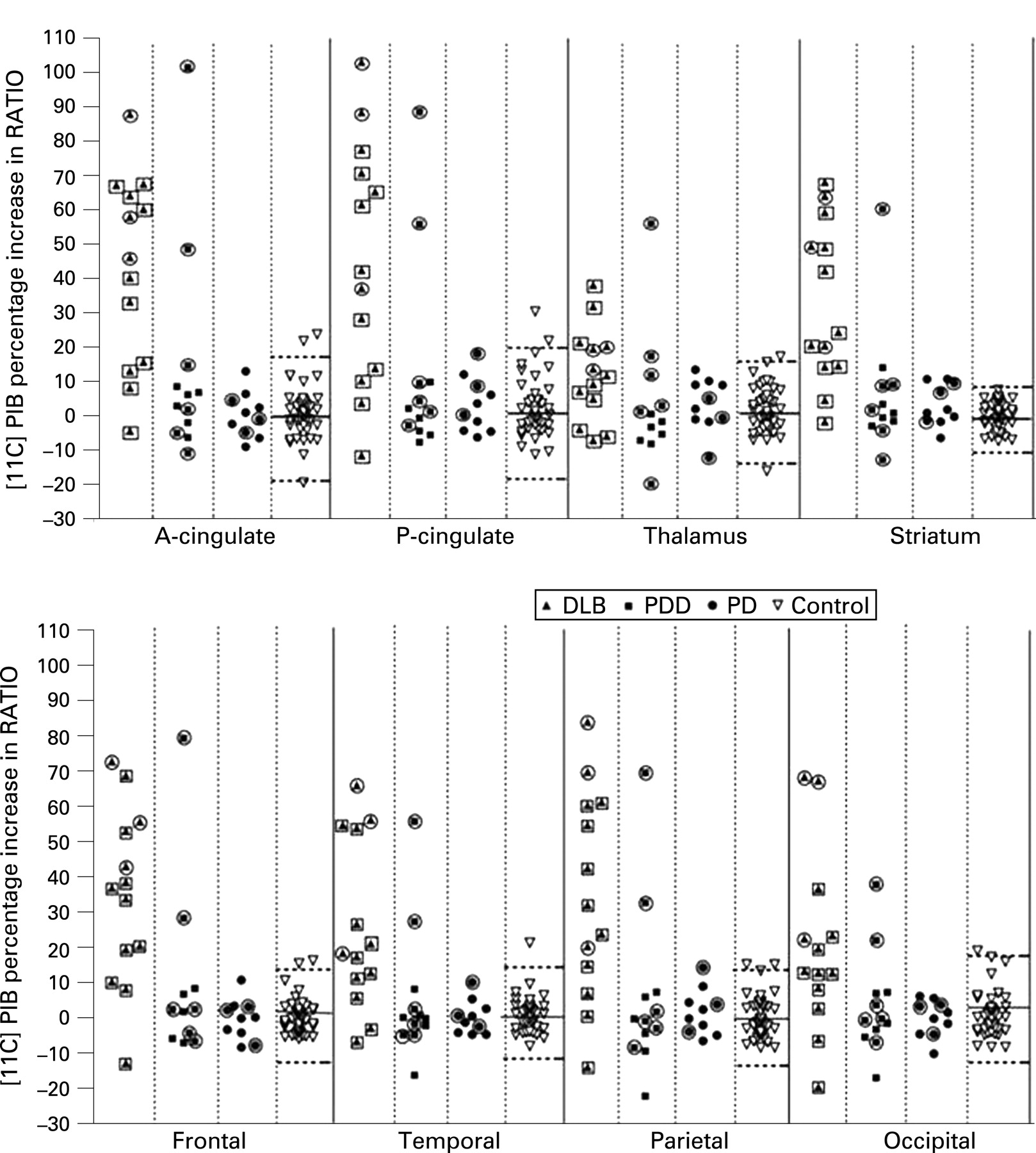
When there was increased [11C]PIB uptake in DLB, the maximum mean increases were seen in the anterior or posterior cingulate followed by the frontal, parietal, temporal and occipital cortex. Two patients with DLB, however, showed parietal and occipital rather than frontal amyloid increases. Figure 1 shows the uptake RATIOs in subjects with DLB, PDD and PD. As the data are combined from three sites, we have reported the percentage increases in the individual subjects relative to the control means for the site. Figure 2 shows the individual percentage increases compared with the corresponding control mean from the relevant PET centre.
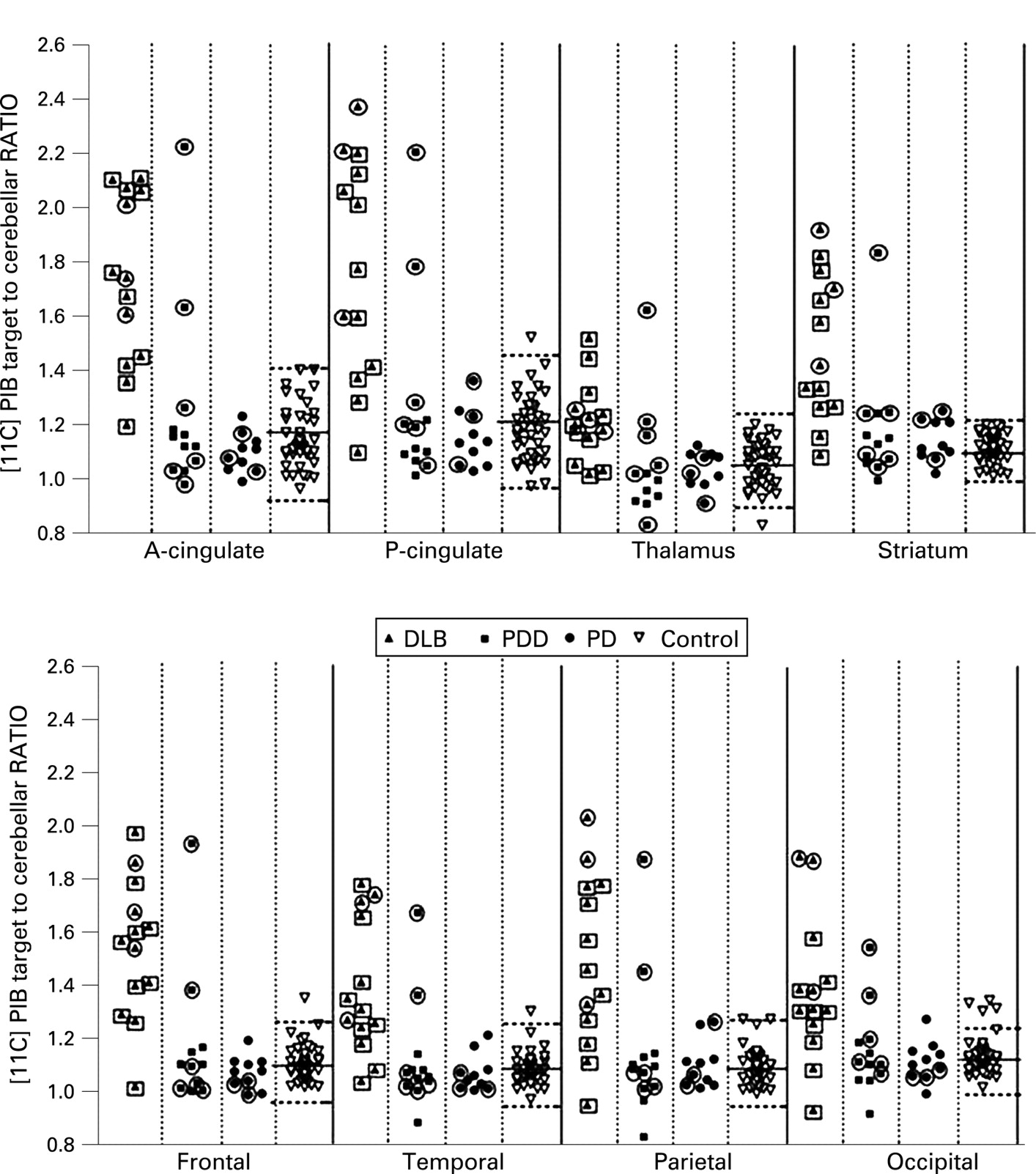

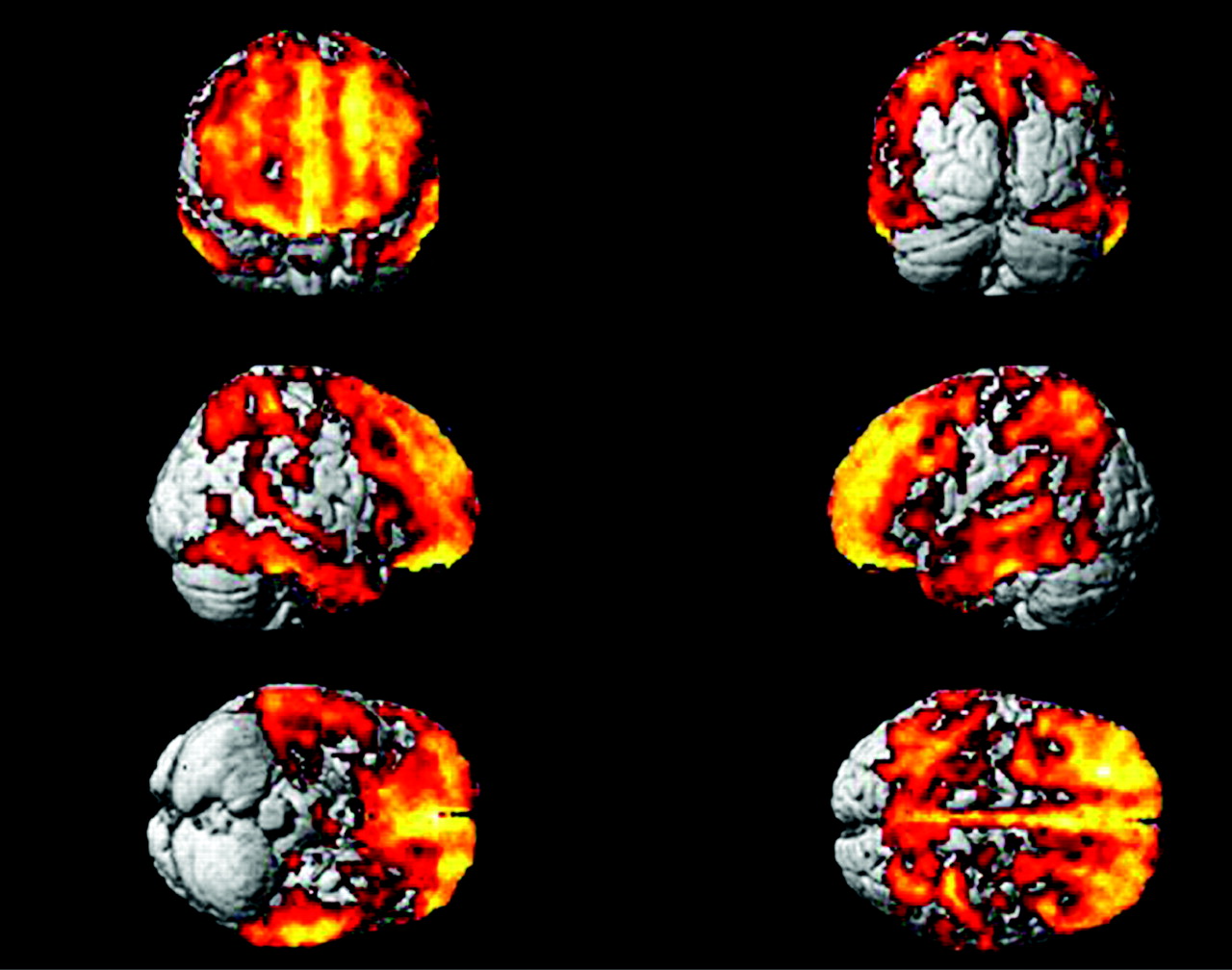
Ten of the 12 patients with PDD had normal [11C]PIB uptake while two patients with PDD showed a similar pattern of increased amyloid load to the majority of the patients with DLB. In these two subjects with PDD, striatal uptake of [11C]PIB was also increased. The two subjects with PDD who had high [11C]PIB uptake did not differ clinically from other subjects with PDD. None of the 10 non-demented PD patients showed any significant increase in [11C]PIB uptake compared with control subjects but two of them showed marginal increases in striatal uptake compared with the controls. Figure 3 shows one subject with DLB with significant amyloid load and one subject with PDD without significant amyloid load. Table 3 and fig 4 show mean [11C]PIB uptake in controls from the three sites.


There were marginal differences in the uptake RATIOs between the control groups but all controls included in this study group had an uptake RATIO of less than 1.4 in their cortical regions.
SPM localised significant increases in frontal, temporal and parietal cortical amyloid in DLB compared with controls, as shown in fig 5 (p<0.001 with an extent threshold of 100 voxels). The pattern of increase was similar to that reported for AD.24–26 31

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
In this in vivo [11C]PIB-PET study we have detected that over 80% of patients with clinically probable DLB show a significantly raised amyloid load in at least one cortical region, while this is true of only 15% of patients with PD who develop later dementia (PDD). Our patients with non-demented PD showed no significant amyloid load. The pattern of distribution of raised amyloid when present in PDD is similar to that in DLB, targeting association cortical areas with a frontal and cingulate emphasis and is consistent with the previously reported pattern of [11C]PIB-uptake in AD.18 25 31 39 40 Increased [11C]PIB uptake in DLB has previously been reported by one of our centres,31 however, by combining data from three different centres and employing a central analysis we were able to demonstrate the difference in pattern of distribution of amyloid in parkinsonian conditions. Whether a combination of amyloid and Lewy body pathology exacerbates the memory and cognitive problems in DLB is unclear but it is likely it accelerates the dementia process whereas Lewy body pathology alone leads to a slower dementing process in PDD.16 In both DLB and PDD, loss of cholinergic and monoaminergic projections will also contribute to onset of cognitive difficulties. Demonstration of amyloid pathology in vivo in the majority of clinically diagnosed DLB cases provides a rationale for targeting both this group and patients with AD with emerging anti-amyloid agents.
Most of our cases of PDD had suffered from parkinsonism for several years (mean 10.6 (4.8) years) before they developed dementia, while the patients with DLB had dementia either from the beginning of their disease or became demented within 1 year of the development of parkinsonism. Post-mortem studies have shown that PDD and DLB share common pathological features.9 There is already doubt about the notion that DLB is a distinct clinicopathological entity from PDD.6 41 42 However, demonstration of significant amyloid pathology in the majority of cases of DLB might explain the rapid clinical deterioration of these patients compared with patients with PDD. We have noticed that when amyloid is present, the pattern of distribution is similar to that of AD. The two patients with PDD with significantly increased levels of amyloid did not differ clinically from other patients with PDD without raised [11C]PIB uptake.
Recent neuropathological studies have shown that in DLB brains both α-synuclein and Aβ plaques are frequent whereas less than 20% of cases of PDD show Aβ plaque pathology.14 43 Interestingly, those subjects with PDD and DLB showing a significant cortical amyloid load also showed significant increases in the striatum.
The mild increase in striatal [11C]PIB uptake in the absence of cortical amyloid in subjects with PD without dementia is an interesting observation. Recently it has been reported that higher [11C]PIB retention can be seen in the striatum compared with the cortex in some asymptomatic presenilin-1 (PS1) mutation carriers.44 This would suggest that the striatum may be one of the first sites for amyloid deposition in both AD and PD. Longitudinal and neuropathological studies will be necessary to examine this more fully. In vitro studies have shown that [11C]PIB binds to α-synuclein fibrils, but with a lower affinity than that demonstrated for Aβ42 fibrils. In one study it has been reported that [11C]PIB failed to bind to DLB homogenates that were Aβ plaque free. This suggests that the increased [11C]PIB retention observed in the majority of subjects with DLB is largely attributable to Aβ plaques.45
Recently it has been shown that [11C]PIB binds avidly to both fibrillar and diffuse amyloid plaques.46 Diffuse amyloid deposits are found in the striatum of cases of AD and DLB but are also seen surrounding blood vessels in DLB47 and amyloid angiopathies.48 Given this, raised [11C]PIB uptake can clearly be a feature of several different types of dementia and more studies are needed to understand the usefulness of [11C]PIB as a diagnostic agent.
We did not find a correlation between amyloid load and MMSE ratings in DLB. However, the MMSE has limitations in that ratings do not reflect executive function. While it was initially reported in the Uppsala series that amyloid load correlated with cognitive performance in AD, this correlation was no longer found to be present on 2 year follow-up.40 In our AD study, no correlation between cortical amyloid load and MMSE was seen if [11C]PIB negative cases were excluded from the analysis.24 31 These findings suggest that in both DLB and AD, cognitive dysfunction is not directly related to amyloid plaque load. However, it has been shown that there is a correlation between cortical [11C]PIB uptake and the time interval between first sign of cognitive impairment recalled by the caregiver and development of diagnostic clinical features of DLB.31
A recent neuropathological study has shown that there is an inverse correlation between the duration of parkinsonism prior to dementia and the density of amyloid plaques, whereas there is a positive correlation with severity of cortical α-synuclein pathology and severity of cortical cholinergic deficits.16 In our PET study the three different centres involved used varying batteries of behavioural tests and so we were not able to correlate executive and visuospatial function tests with amyloid load.
In the present study, we combined data from three PET centres. [11C]PIB uptake in DLB and more recently in PDD has already been reported.31 49 By combining PIB PET data from three centres, we have had an opportunity to examine [11C]PIB uptake in PDD and PD in comparison with DLB. Using a target region:cerebellar [11C]PIB uptake ratio approach provides an internal reference to minimise between centre variability, as does a central analysis. In this study we have reported individual rises in [11C]PIB uptake compared with the mean of control subjects from the corresponding site. Individually, the control subjects included from the three centres all had a cortical uptake RATIO of less than 1.4 although there were marginal differences in mean cortical uptake RATIOs between the different sites. One of the criticisms of the RATIO method is that it could underestimate [11C]PIB uptake if there is specific tracer binding in the cerebellar reference. In the PDD subgroup, we had arterial tracer input functions available and failed to find any evidence of significant cerebellar [11C]PIB retention. (Results not discussed in this paper). Thus the finding of unchanged [11C]PIB uptake ratios in most PDD cases is likely to be representative and not artificially caused by the presence of amyloid in the cerebellum.
In summary, our in vivo [11C]PIB PET findings suggest that PDD and DLB may be differentiated by the relatively lower amyloid plaque load in the former. This study shows there is a significant difference in the proportion of patients having amyloid in PDD and DLB and also suggests that in the future, [11C]PIB PET will allow us to specifically target appropriate subjects with DLB and PDD with novel anti-amyloid strategies.
Acknowledgments
The authors thank the staff of the PET Centres for technical assistance and Hammersmith Imanet, GE Healthcare for provision of the radiotracers and scanning facilities. The authors also thank Hope McDevitt, Stella Ahier, Andreana Williams and Andrew Blyth for help with scanning, Safiye Osman for blood analysis and Dr Federico Turkheimer for advice on statistical analysis.
REFERENCES
Footnotes
-
Funding: This study was financially supported by EVO grants from Turku University Hospital, and by grants from the Research Council for Health of the Academy of Finland (project # 205954) and the Sigrid Juselius Foundation.
-
Competing interests: This study was financially supported by the Medical Research Council, UK, Turku University Hospital, Research Council for Health of the Academy of Finland and the Sigrid Juselius Foundation. PE is a Medical Research Council clinical research fellow. JOR is the consulting scientific advisor for Turku Imanet and DJB is the chief medical officer for Imanet, GE Healthcare.
-
Ethics approval: Permission to perform the study was obtained from the relevant ethics committees and regulatory bodies.