Article Text

Abstract
Objective To investigate the extrastriatal dopaminergic neural changes in relation to the medication-related impulse control disorders (ICD) in Parkinson's disease (PD).
Method A total of 31 subjects (11 and 11 drug-treated PD patients with and without medication-related ICDs and 9 healthy controls) having no other co-morbid psychiatric disorders participated in this study. Each subject underwent dynamic N-(3-[18F]fluoropropyl)-2-carbomethoxy-3-(4-iodophenyl) nortropane (FP-CIT) positron emission tomography scans. Binding potentials (BP) at nucleus accumbens, amygdala, orbitofrontal and ventromedial prefrontal cortex (VMPFC), putamen and caudate nucleus were estimated, and whole brain parametric maps of [18F]-FP-CIT binding were analysed by original and putaminal normalised manners.
Results Compared with the healthy controls, BPs at both VMPFCs were significantly high and the extrastriatal to putaminal BP ratios at all regions were approximately three times higher in both PD groups. The PD ICD patients showed significantly higher BPs at the right VMPFC and tendency to lower BPs at the left nucleus accumbens compared with those free of ICD. The ICD subjects also showed reduced uptakes at both ventral striatal regions in the original parametric analysis and higher uptakes at the left insular and right posterior cingulate cortex and lower uptakes at both ventral pallidums in the putaminal normalised parametric analysis compared with the non-ICD subjects.
Conclusions A great gap in extrastriatal versus striatal dopaminergic fibre degenerations is an intrinsic condition predisposing to ICD in PD. Distinct pattern of extrastriatal changes between the ICD and non-ICD patients could provide a further insight into a mechanism of ICD in PD.
- Movement Disorders
- Parkinson's Disease
- Pet, Functional Imaging
Statistics from Altmetric.com
Introduction
Impulse control and repetitive behaviour disorders in patients with Parkinson's disease (PD) is one of the treatment-related complications of long-term dopamine replacement therapy, of which the prevalence has been reported to be 10.1% in north-east Asia1 as well as 13.6% in north America2 and up to 30% with punding and compulsive medication use included.3 These behavioural disturbances resemble impulse control disorder (ICD) and drug addiction in nature; thus, studies regarding its pathophysiology have focused on the role of mesolimbic dopamine and its related frontostriatal circuitry in reward, reinforcement and addiction formation.4–7 In patients with PD, exogenously administered dopaminergic drugs may disturb normal physiologic release of dopamine in the mesolimbic region.5 ,6 ,8 Dopamine agonists have high affinity to limbic dopamine receptors such as D3 and do more tonic stimulation of postsynaptic receptors than levodopa would potentiating this disturbance.9 Epidemiological studies support this hypothesis, in that ICD is highly related to the use of dopamine agonists rather than levodopa9 and that it can be resolved by cessation of dopamine agonists or reduction of their dosages.6 ,10 ,11 ICD is also reported in patients with restless leg syndrome, progressive supranuclear palsy and fibromyalgia treated with dopamine agonists with high affinity to D3.12–14 In addition to ‘hyperstimulation’ theory of mesolimbic dopamine system, recent functional imaging studies showed impairments in ‘top-down’ frontostriatal control of behaviours causing negative consequences in PD patients with pathological gambling.15 ,16
Mesolimbic and mesocortical pathway is one of the main dopaminergic projections in human brain, and dopamine transporter (DAT) imaging for the extrastriatal dopaminergic system has showed mild degree reduction in drug-naïve PD patients.17 Thus, it can be hypothesised that intrinsic changes related to PD pathology or dopaminergic treatment-related changes in this system may be associated with the risk of ICD in PD. In order to investigate extrastriatal fibre changes, we obtained dynamic N-(3-[18F]fluoropropyl)-2-carbomethoxy-3-(4-iodophenyl) nortropane ([18F]FP-CIT) positron emission tomography (PET) scans in patients with PD on chronic dopamine replacement therapy and age-matched healthy controls, and then quantitatively analysed DAT bindings in the extrastriatal versus striatal regions. Since unbalanced stimulation of the extrastriatal versus striatal regions by dopamine replacement therapy in PD may depend on the differences between the two system changes, we also analysed putaminal normalised whole brain parametric [18F]FP-CIT binding maps to evaluate possible association between the changes in the extrastriatal versus striatal systems and the appearance of ICD in PD.
Methods
Subjects
This study was approved by the Institutional Board of Seoul National University Hospital, and informed consent was obtained from all subjects according to the Declaration of Helsinki.
A total of 26 consecutive patients with PD (13 with ICD and 13 without ICD) and 10 age-matched healthy controls were enrolled in this study. The PD subjects were diagnosed according to the criteria of the UK PD Brain Bank Society,18 and the patients had been treated with dopaminergic drugs for at least 5 years. The PD ICD group was identified during routine follow-up examinations by interviewing patients and their caregivers on whether they had medication-related ICDs composed of pathologic or compulsive gambling, shopping, binge eating and hypersexuality as previously proposed.6 Those with current ICD behaviours were enrolled in this study only if they fulfilled the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders Text Revision criteria (DSM-IV-TR, American Psychiatric Association, 1994) for ICD and had no prior history of ICD before developing PD. The PD non-ICD group was also identified during routine follow-up examinations by interviews with no symptoms suggestive of ICD and no prior history of ICD. Those who had cognitive impairment (mini-mental status examination (MMSE) score <24), history of depression or other psychiatric illness, alcohol dependence or substance use disorders, and neurological diseases other than PD and those who had neurosurgical procedures were all excluded from this study. Those who were taking anti-psychotics, anti-depressants and various drugs affecting dopamine and serotonin systems except for anti-parkinsonian drugs were excluded due to the possibility of alterations in DAT uptake.
All subjects underwent evaluations at their medication-on state by means of the Unified Parkinson's Disease Rating Scale (UPDRS), the MMSE, the Geriatric Depression Scale 30 items (GDS), Hoehn and Yahr (HY) stage and the modified version of Minnesota Impulsive Disorders Interview (mMIDI) which was used for assessing the four ICD behaviours and punding (see details published elsewhere19). Subjects having only punding behaviours but without ICDs were not considered into this study. Clinical information such as age, gender, duration of PD and daily dosages of dopaminergic drugs was collected, and total daily levodopa equivalent dose (total LED) and agonist daily levodopa equivalent dose (agonist LED) were calculated as previously described.1
Acquisition of PET data
Each subject underwent a 90-min dynamic [18F]FP-CIT PET scan (Siemens Biograph 40 Truepoint PET/CT, Knoxville, Tennessee, USA) after at least a 12-h withdrawal of all anti-parkinsonian medications including levodopa, dopamine agonist, amantadine and monoamine oxidase inhibitors. For each subject, 185 MBq (5.0 mCi) [18F]FP-CIT was administrated with an intravenous bolus injection, and the emission data were then acquired over 90 min with 50 frames of progressively increasing durations (15 s×8 frames, 30 s×16 frames, 60 s×10 frames, 240 s×10 frames and 300 s×6 frames). The dynamic PET data were collected in three-dimensional mode, which provides 148 slices with an image size of 256×256, a pixel size of 1.3364×1.3364 mm2 and a slice thickness of 1.5 mm. After applying routine corrections such as normalisation, decay, dead time, random and scatter corrections, the dynamic images were reconstructed with filtered back projection using a Gaussian filter.
MR image acquisition and processing
High-resolution brain MRI scans for each subject (repetition time=1600 ms; echo time=1.91 ms; 3 T T1-weighted images with an image matrix of 256×256, a pixel size of 0.9375×0.9375 mm2 and a slice thickness of 1 mm) were acquired using a Siemens Magnetom Trio, a Tim system for co-registration and spatial normalisation of the reconstructed dynamic PET and parametric images. The mean image of all dynamic frames in the individual PET data was co-registered to the corresponding T1-weighted MRI scan using the normalised mutual information-based registration technique.20 ,21 Then, all the dynamic frames of each subject were also co-registered using the resulting nine-parameter rigid-body transformation. After the individual MR images were spatially normalised to the MNI152 template using the nonlinear registration with basis functions22 in SPM8 (Statistical Parametric Mapping, University College of London, UK), the original reconstructed dynamic images were also transformed into standardised stereotaxic space using the co-registration and resulting normalisation transformations together.
Quantitative estimation of [18F]FP-CIT binding potentials in volumes of interest
Anatomical boundaries of putamen (PUT), caudate nucleus (CAU), nucleus accumbens (NAC), amygdala (AMG) and cerebellum (CB, used as a reference region) were determined on the MR images of each subject using the FMRIB Integrated Registration and Segmentation Tool (FIRST, FSL V4.0, Oxford University, Oxford UK, http://www.fmrib.ox.ac.uk/fsl). Volumes of interest (VOI) time activity curves (TACs) were extracted from the co-registered dynamic images by averaging the TACs of voxels spanning those VOIs. The TACs in the ventromedial prefrontal and orbitofrontal cortex (VMPFC and OFC) were extracted by delineating the VOIs using the MRI statistical probabilistic anatomy map (SPAM) data (see online supplementary figure S1, details published elsewhere).23 For the quantification of [18F]FP-CIT binding in VOIs, we applied the Logan plot.24
Voxel-wise analysis of [18F]FP-CIT BPs in a whole brain
To generate parametric mapping of binding potential (BP), the Logan method was applied to the voxel TACs on original dynamic images. For a subsequent between-group comparison, each individual parametric image was normalised into the stereotaxic space by recycling the transformation parameters previously computed for the dynamic images. To investigate BP changes in the extrastriatal regions relative to the striatal regions, the spatially normalised parametric images were transferred to the MNI space and normalised in terms of the intensity to their own putaminal BPs which was obtained by SPAM.
Statistical analysis
In the comparisons between the groups by clinical characteristics, the Mann–Whitney test was used for continuous variables and Fisher's exact test was used for categorical variables. For the comparisons of VOI BPs, Mann–Whitney test was used for comparison between PD as a whole group and normal controls, and the analysis of variance test was used for three group comparisons with fulfilment of equal variance assumption. Then, a post hoc analysis was conducted for the difference between the PD ICD and PD non-ICD groups. The correlations between the BP ratios of the extrastriatal versus putaminal VOIs were examined by Spearman’s correlation analysis. The statistical analyses were conducted using the SPSS software (V.19.0; SPSS Inc., Chicago, Illinois, USA), with the limit of significance set at 0.05 (two-tailed).
In the parametric image analyses, the original and the putaminal normalised images on the stereotaxic space underwent a Gaussian smoothing with 12-mm FWHM kernel to reduce the image registration error. Statistical inference was subsequently done at each voxel; for each voxel, we tested whether both groups show the same average BP values through analysis of covariance, while adjusting for the age effect. The test was performed using SPM8, and the reported MNI coordinates of significant regions were converted into the Talairach coordinates using the icbm2tal software (http://www.brainmap.org/icbm2tal).
Results
Among the 36 subjects, the image quality was insufficient in two and acquisition of a PET scan was not completed in 3 subjects; thus, the data from 22 subjects with PD (11 ICD and 11 non-ICD) and 9 normal controls were used in the analyses. Demographic and clinical characteristics of the subjects are presented in table 1. There was no difference in age and sex distributions between PD and healthy controls (p=0.515 and 0.696, respectively). There were no differences in age, sex, age at PD onset, duration of PD, HY stage, total and agonist LEDs, and UPDRS scores between the PD ICD and non-ICD groups (table 1). Among the 11 PD ICD subjects, eight patients had two or more kinds of behaviours and three had one type of behaviour (gambling for two and hypersexuality for one). The characteristics of the ICD behaviours in our subjects are summarised in the online supplementary table.
Characteristics of the subjects finally included in the analysis
Comparisons of [18F]FP-CIT BPs at VOIs in the extrastriatal versus striatal regions
The [18F]FP-CIT BPs in the PUT and CAU were significantly low in PD as expected (table 2). BPs at NAC, AMG and OFC were not different between the PD and normal controls, whereas BPs at both VMPFCs were significantly higher in the PD group (table 2). To estimate the difference between the extrastriatal versus striatal FP-CIT binding, we compared the BP ratios of NAC/PUT, AMG/PUT, OFC/PUT and VMPFC/PUT, which were found to be about three times higher for NAC, AMG and OFC and five to six times higher for VMPFC in the PD group compared with those in the healthy controls (all p<0.001, figure 1).
Comparisons of [18F]FP-CIT binding potentials between PD and healthy subjects
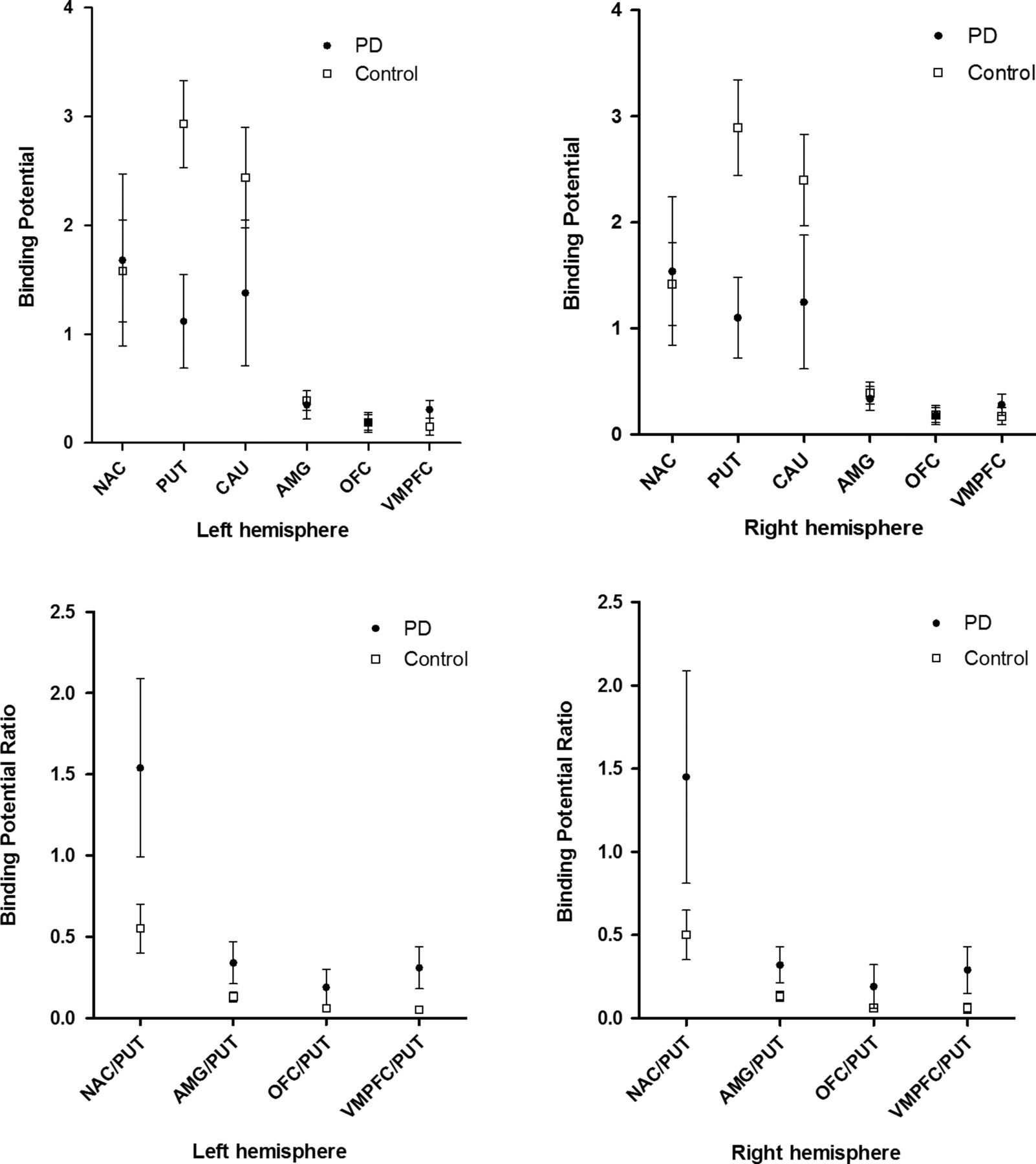
Estimated [18F]FP-CIT binding potentials at the volumes of interests in subjects with PD and in normal controls. Dark circle=PD, empty square=normal control. Symbols represent mean values, and error bars, mean SDs. AMG, amygdala; CAU, caudate nucleus; NAC, nucleus accumbens; OFC, orbitofrontal cortex; PD, Parkinson's disease; PUT, putamen; VMPFC, ventromedial prefrontal cortex.
In the three group comparisons, there were significant BP differences in PUT, CAU and VMPFC, and a tendency of difference but no significance in NAC. The post hoc analysis comparing the PD ICD and non-ICD groups, revealed no statistical significance in PUTs and CAUs, but a significant difference in the right VMPFC where PD ICD subjects had higher BP (p=0.033), and a marginal difference in the left NAC where PD ICD subjects had lower BP than the non-ICD subjects (p=0.049). Regarding extrastriatal VOI changes, there was a tendency of low [18F]FP-CIT bindings in the mesolimbic (NAC and AMG) and high bindings in the mesocortical (VMPFC and OFC) areas in the PD ICD group compared with those in the non-ICD group, although statistical significance was only seen at the left NAC and the right VMPFC as above (table 3).
Comparisons of [18F]FP-CIT binding potentials among the three groups and between the PD ICD and the PD non-ICD groups
In the correlation analysis between the BP ratios and the modified MIDI scores which represents the magnitude and frequency of ICD behaviours, the right VMPFC/PUT BP was significantly correlated with them in PD patients (p=0.016, r2=0.508, see online supplementary figure S2). The BP ratios at other regions showed no significant correlations.
Parametric analysis of [18F]FP-CIT bindings between PD as a whole group and healthy controls
In the original parametric analysis of the whole brain comparing PD and normal controls, reduced uptake was seen in the bilateral basal ganglia, hypothalamus, superior colliculus and periaqueductal midbrain tegmental areas containing locus ceruleus in PD (figure 2A, p<0.001).
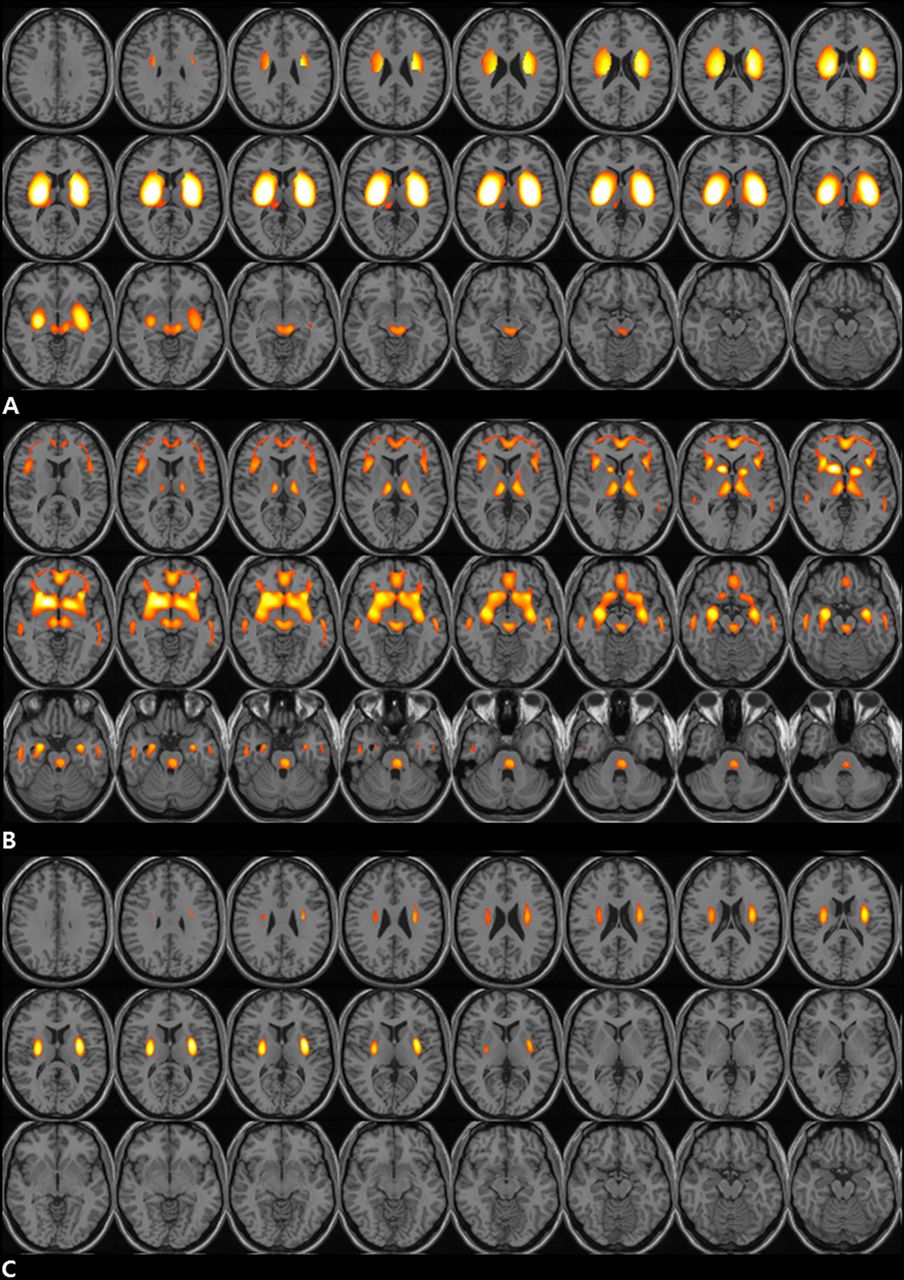
Parametric maps of dynamic N-(3-[18F]fluoropropyl)-2-carbomethoxy-3-(4-iodophenyl) nortropane ([18F]FP-CIT) bindings comparing between patients with Parkinson's disease (PD) and normal controls. (A) In the original parametric image, normal control >PD (p<0.001) (B) In the putaminal normalised parametric image, PD >normal control (p<0.001) (C) In the putaminal normalised parametric image, normal control >PD (p<0.001). Access the article online to view this figure in colour.
In the putaminal normalised parametric maps of PD>healthy controls, we obtained a well-separated image of mesolimbic and mesocortical systems. The highlighted areas included bilateral VMPFC, OFC, insular cortex, ventral striatum (VS) containing NAC and ventral pallidum (VP), AMG, thalamus, midbrain and pontine periaqueductal grey regions covering rostral and caudal dorsal raphe nucleus, and parahippocampal regions, to which serotonergic as well as mesolimbic and mesocortical dopaminergic projections were innervated (figure 2B, p<0.001). On the other hand, in the parametric maps of healthy controls >PD subjects, there were higher uptakes at the bilateral dorsal and posterior putamens representing the motor parts of the nigrostriatal dopaminergic projections (figure 2C, p<0.001).
Parametric analysis of [18F]FP-CIT binding between PD ICD and PD non-ICD groups
On the original parametric images, significantly lower uptakes were seen in both VS extending to VP in PD ICD group (p<0.005, figure 3A). On the putaminal normalised parametric analysis, significant higher uptakes were seen at the left insular and right dorsal posterior cingulate cortex (DPCC) in the PD ICD group (figure 3B, p<0.01), whereas a significantly lower uptake was seen at the bilateral VPs in the PD ICD compared with the non-ICD groups (figure 3C, p<0.005).

{kind=link}
{kind=link}
{kind=link}
Comparisons between subjects with Parkinson's disease having impulse control disorders (PD ICD) and those free of ICD (PD non-ICD) by the parametric analysis. (A) In the original parametric analysis, PD ICD<PD non-ICD. Significant uptakes are seen at the bilateral ventral striatum and ventral pallidum. (A) (p<0.005). (B) In the putaminal normalised parametric analysis, PD ICD>PD non-ICD. Significant uptakes are seen at the left insular area and right posterior cingulate cortex (p<0.01). (C) In the putaminal normalised parametric analysis, PD non-ICD>PD ICD. Significant uptakes are seen at the bilateral ventral pallidum (p<0.005). Talairach coordinates for the regions with significant difference are presented with the responsible Broadmann area (BA). Access the article online to view this figure in colour.
Discussions
This study investigated the extrastriatal versus striatal dopaminergic neural changes in PD by VOI-based and whole brain parametric analysis of dynamic [18F]FP-CIT PET scans. Since extrastriatal bindings were not significantly reduced in PD, there was a significant gap between the extrastriatal versus striatal DAT bindings by approximately three times higher in PD compared with normal controls (figure 1). This unique pathological condition in PD can be linked to hyperstimulation of extrastriatal system by dopamine replacement therapy. The DAT binding in the extrastriatal system is very weak relative to the striatal system; thus, we conducted dynamic [18F]FP-CT PET scans to calculate BPs in these regions. In addition, to enhance visualisation of extrastriatal DAT bindings, we made each individual’s whole brain maps to be normalised to their own putaminal bindings. The putaminal normalised parametric analysis made visualisation of the mesolimbic and mesocortical systems. This image contained serotonergic fibres in addition to the extrastriatal dopaminergic fibres especially in the regions such as the VMPFC, OFC, insular cortex, anterior and posterior cingulate cortex, AMG, thalamus, and midbrain and pontine raphe nucleus, which may be due to the cross-affinity of FP-CIT to the serotonin transporters. Comparisons of these parametric maps between the two PD groups suggested distinct extrastriatal fibre changes may be associated with ICD in PD although it is not known whether these changes are primary or secondary to the ICD.
There has been only one study investing presynaptic dopaminergic changes by DAT imaging regarding ICD in PD.25 By means of [123I]FP-CIT SPECT, it showed reduced DAT bindings in the VS in PD patients with pathological gambling.25 The extrastriatal areas were not fully investigated in that study probably due to methodological limitation, inferior spatial resolution and sensitivity of SPECT compared with those of PET to demonstrate extrastriatal FP-CIT bindings. Moreover, in that study an in-house [11C]raclopride PET template was used instead of the subjects own MRI templates, which made it more difficult to estimate BPs at extrastriatal areas as well as to identify anatomical structures precisely. We found low DAT binding density at bilateral VS (which contains NAC region) in the parametric analysis in the PD ICD group. Thus, our observation was in part consistent with the previous DAT study results.25 Some studies have suggested that dopamine receptor availability at VS may be reduced in ICD subjects26 ,27 while others did not.28 The low postsynaptic receptor availability may result from synaptic hyperdopamine content which is also exacerbated by low DAT at VS, which supports ‘hyperdopamine’ theory in the mesolimbic region in PD-ICD patients. VS is important in reward reinforcement learning, and studies on VS dopamine release in response to reward-related stimuli showed sensitised and enhanced release of dopamine in PD patients with ICD.26 ,28 ,29 A similar pattern has been reported in cocaine abusers30 and the enhancement of dopamine release in VS was well explained by the incentive salience model26–29 in both conditions. Thus, downregulation of DAT at VS may be a plastic change as a sensitisation to reward-related behaviours, which is an early event of addiction formation.31
In the VOI analysis, the right VMPFC binding was significantly higher in the PD ICD group despite more loss of putaminal bindings than that in the non-ICD group. It is possibly related to the upregulation of DAT to maintain synaptic dopamine homeostasis32 or to the less degeneration of dopaminergic fibres in this region since BPs at the VMPFC in our PD subjects were higher than those in age-matched healthy controls. The prefrontal cortex including the OFC, the VMPFC and anterior cingulate area is a well-known region for mediating reward related behaviours; the VMPFC is more specifically processing of diverse and abstract rewards (such as money) whereas lateral part of the OFC is activated to punishment rather than to rewards.33 Based on our study results, dopaminergic activation of reward processing area rather than those of punishment might be more important in PD ICD. A recent [18F] fluorodopa PET study also showed enhanced activity at the medial part of the OFC in PD patients with ICD,34 which supports our observations.
In the putaminal normalised parametric analysis, there were two areas with enhanced DAT bindings in PD ICD subjects; DPCC and anterior insular cortex. The DPCC is reported to be functionally connected to VMPFC and medial OFCs in drug addicts.35 ,36 The insular cortex is involved in conscious urges (craving for addictive behaviours),37 and lesions on the insular cortex diminished the urge for smoking in stroke patients.38 Since modification of craving is important from a therapeutic aspect, this finding is worth replicating by other studies.
The VP is known to receive convergent signals of all kinds of rewards, and activation of VP is essential for reward-related and affective behaviours.39 VP receives projections from multiple regions including ventral tegmental area (VTA) and NAC. Dopaminergic transmission to VP is probably from VTA as nigropallidal fibres. The action of the dopaminergic projection to VP is not clearly known, but it may transmit a modulatory signal over reward-related behaviours as nigropallidal fibres are thought to be involved in tuning of voluntary movements.40 ,41 Lower DAT binding in VP in PD ICD subjects might be from a plastic change with a sensitised response to rewards, similar to low DAT binding in VS in them.25
Recent studies on the functional network in PD patients with pathological gambling showed that the connectivity between the striatum and anterior cingulate cortex (ACC) was reduced,15 and there was deactivation of the rostral cingulate zone (RCZ) during a gambling task following dopamine agonist administration.16 The ACC/RCZ is known to play a controlling part over behaviours causing negative consequences; thus, hypoactivation of the inhibitory system is another common mechanism of ICD in PD.15 ,16 However, significant dopaminergic neural change in ACC/RCZ was not observed in the present parametric analysis; thus, this hypoactivation may not seem to be directly mediated by changes in the dopaminergic fibres.
However, the results of the present study need to be interpreted with caution. First, this is rather a pilot investigation of extrastriatal system with a small sample size, and the result cannot be generalised to all kinds of ICD behaviours observed in PD. Thus, replication studies with larger sample sizes are warranted to prove our findings. Second, the [18F]FP-CIT ligand used in this study has cross-affinity to serotonin transporter; thus, studies with more specific ligand than FP-CIT or those with two PET scans for DAT and serotonin transporters would be better show more specific changes in the extrastriatal dopaminergic neural fibres in relation to ICD in PD. Third, the mMIDI used in our analysis has not been validated. This study began before publishing of the QUIP-rating scale, a validated tool in PD; thus, we were not able to use it in the current study. Last, we did analyse only neuroanatomical changes but functional consequences of it as well as the precise actions of extrastriatal dopaminergic systems on causing ICD in PD were not investigated in the present work.
For all that, a great gap in extrastriatal versus striatal dopaminergic fibre degenerations is an intrinsic pathological condition in PD. Extrastriatal dopaminergic changes, specifically those seen as activation of areas regarding reward-sensitive decision-making and interoceptive urges and those seen through less dopaminergic modulation to areas receiving convergent signals from diverse rewards, could provide a further insight into a mechanism of medication-related ICD in PD.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figures
- Data supplement 2 - Online table
Footnotes
-
Contributors JYL: research project: conception, organisation, execution; statistical analysis: design, execution; manuscript: writing of the first draft. SHS: research project: execution; statistical analysis: design, execution; manuscript: writing of the first draft. HBY: research project: organisation, execution; statistical analysis: review and critique; manuscript: review and critique. YEK: research project: execution; statistical analysis: review and critique; manuscript: review and critique. YKK: statistical analysis: execution, review and critique; manuscript: review and critique. ICS: research project: organisation; statistical analysis: review and critique; manuscript: review and critique. JSL: research project: conception, organisation; statistical analysis: design, review and critique; manuscript: writing of the first draft, review and critique. BSJ: research project: conception, organisation; statistical analysis: review and critique; manuscript: review and critique.
-
Funding This study was supported by a grant of National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (2011-0014451).
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was approved by the Institutional Board of Seoul National University Hospital (H-1009-100-333).
-
Provenance and peer review Not commissioned; externally peer reviewed.