





Abstract
Positron emission tomography is a three-dimensional imaging technique that measures physiological effects, including metabolism. 18Fluorodeoxyglucose has been extensively used as a tracer of cellular energy metabolism in the brain and in tumour detection. As neutrophils utilise glucose as an energy source during their respiratory burst, it was hypothesised that 18fluorodeoxyglucose uptake, by these cells, could be interpreted as a measure of neutrophil activation in cystic fibrosis (CF).
Ten adult CF patients were given a bolus intravenous injection of 18fluorodeoxyglucose, followed by a 90-min dynamic mid-lung acquisition scan. Right-lung 18fluorodeoxyglucose uptake was assessed using a Patlak plot and values were converted to glucose utilisation. Three clinically inactive pulmonary sarcoidosis patients served as controls.
From the 10 CF patients with baseline sputum neutrophils of 14×106 cells·mL−1 who were investigated, seven were found to have sputum at a normal or slightly depressed glucose utilisation rate (mean 1.33 µmol·g−1·h−1) compared with a mean of 2.82 µmol·g−1·h−1 for the sarcoidosis patients. In eight patients, receiving inhaled tobramycin therapy, no change in lung glucose utilisation or sputum neutrophil counts were found.
Despite high-sputum neutrophil levels, lung glucose utilisation was not elevated in patients with cystic fibrosis.
This study was funded by the Canadian Cystic Fibrosis Foundation (SPARX 2).
Positron emission tomography (PET) is a powerful, quantitative, nuclear medicine tomographic imaging technique. PET can be used to measure physiological effects such as blood flow, metabolism, ventilation, receptor occupancy, regional dose delivery and pharmacokinetics of radiolabelled drugs 1. It combines principles of image reconstruction from projections with the use of specific biological molecules labelled with positron-emitting radioisotopes (11C, 18F, 15O, 13N) allowing regional measurements of dynamic processes to be taken.
18F‐2‐fluoro‐2‐deoxy‐d‐glucose (18FDG) is a tracer of cellular energy metabolism. It has been used extensively to monitor the metabolic activity of cells in vivo in the brain 2–5 and to detect tumours 6–8. 18FDG differs from glucose by the substitution of the hydroxyl group with a fluorine atom on the second carbon of the glucose. When injected intravenously, 18FDG rapidly diffuses into the extracellular spaces throughout the body. It is transported into living cells by the same mechanism as glucose, via the d‐glucose transporter and is phosphorylated by hexokinase to fluoro-deoxyglucose‐6‐phosphate. The deoxy substitution at the second carbon position prevents further metabolism and the product accumulates in the cell at a rate that reflects glucose metabolism. Increased glucose consumption is assumed to lead to an increased rate of tracer uptake. The rate of accumulation of 18FDG in tissue after intravenous injection reflects the combined transport and hexokinase activity in the cells 9. 18FDG-PET studies of the lung are still relatively few compared with the number of oncological, neurological and cardiac studies.
The inflammatory process, in particular neutrophils, has been implicated in the pathogenesis of a variety of lung diseases including cystic fibrosis (CF), bronchiectasis, and chronic bronchitis. Neutrophils contribute to pulmonary destruction by production and release of cytotoxic enzymes (e.g. elastase, myeloperoxidase) and toxic oxygen metabolites 10. Markers of inflammation in blood, bronchoalveolar lavage (BAL), sputum and lung biopsy serve as indirect measurements of inflammation, making the detection of regional variation of inflammation in the lung impossible 11–14. 18FDG uptake is a well-validated in vivo measure of tissue glucose metabolism using PET. 18FDG preferentially accumulates in areas with increased metabolism, such as tumours, in which the rate of uptake is six to seven times higher than normal tissue 7, and sites of infection where the metabolic rate of glucose is elevated in activated inflammatory cells, such as neutrophils 15–17. It is hypothesised that 18FDG and PET could be used to measure and monitor the metabolic activity of neutrophils in neutrophil-dominated inflammatory diseases of the lung including CF. An increase in the 18FDG signal is detected in the presence of neutrophils, lymphocytes and macrophages. These cells have a high anaerobic to aerobic metabolic ratio due to a relative lack of oxidative enzymes. Compared with aerobic glucose degradation, anaerobic metabolism consumes considerably more glucose to produce equivalent amounts of adenosine triphosphate 9. Uptake of 18FDG reflects glucose metabolism, therefore, its uptake is accelerated in anaerobic glycolysis. Neutrophils utilise glucose as the main source of energy, deriving most of their energy supply from glycolysis 15, 18. Glucose utilisation in neutrophils is 10-times higher than that in lymphocytes 16. Although macrophages can use glycolysis, during phagocytosis, they rely more on oxidative phosphorylation in well-oxygenated areas such as the lungs 18. While the use of 18FDG-PET in detecting and monitoring inflammatory events in the lung is relatively new, studies have shown that an increase in 18FDG uptake indicates the presence of inflammatory activity, particularly neutrophil activation. In patients with acute lobar pneumonia, microautoradiography of 18F in lavage fluid showed radioactivity localised to >90% of the neutrophils 19. In an in vivo animal study using a rabbit model of acute (Streptococcal pneumonia) and chronic (bleomycin-induced injury) lung inflammation and autoradiography, Jones et al. 20 showed that 18FDG uptake was localised to neutrophils and not macrophages, which outnumbered neutrophils 5:1 in the case of bleomycin-induced lung injury.
Progressive respiratory disease is associated with significant morbidity and mortality in CF patients and is the leading cause for 80% of deaths each year 21, with the chronic neutrophil-dominated inflammatory process firmly implicated in the destruction of the lung in CF 22. Therefore, it is possible that the 18FDG-PET technique could be used to study the degree of lung inflammation, the progression of disease and to assess local tissue response to anti-inflammatory therapeutic interventions. The objectives of this study were as follows: 1) to determine the extent of inflammation in the lungs of patients with CF using 18FDG and PET imaging; 2) to ascertain if a correlation could be demonstrated between the degree of lung neutrophilia, as measured by the accumulation of 18FDG in the lung, with the neutrophil values obtained from sputum cytology; and 3) to determine if 18FDG and PET could detect changes in the degree of lung inflammation after a 28-day inhaled tobramycin treatment.
Methods
Subjects
Patients with CF, who were ≥16 yrs, chronically infected with Pseudomonas aeruginosa and in a stable clinical condition (defined as no acute exacerbations in the previous 4 weeks) were enrolled in the study. Subjects with nonactive sarcoidosis served as controls. The study was approved by the Hamilton Health Sciences Research Ethics Committee and written informed consent was obtained before the initiation of the study.
Study design
The study consisted of two PET scans of the lung, separated by 28 days of nebulised tobramycin therapy. Patients nebulised 160 mg of tobramycin (Eli Lilly, Scarborough, Canada) b.i.d. using a Pari LC Star nebuliser and ProNeb Turbo compressor (PARI Respiratory Equipment, Inc., Mississauga, Canada).
A spontaneously expectorated sputum specimen was obtained prior to each PET procedure. Sputum cytology was performed as described by Pizzichini et al. 23 with modifications for CF 24. Spirometry was measured at the beginning and end of each PET scan, according to American Thoracic Society standards 25.
18F‐2‐fluoro‐2‐deoxy‐d‐glucose and positron emission tomography methods
Patients were given a bolus intravenous injection of 1.0–1.5 mCi of 18FDG (50 µCi·kg body weight−1) into a vein in the hand or arm, while in the supine position on the scanner bed of the ECAT ART scanner (CPS Innovations, Knoxville, TN, USA) 26. A 90-min dynamic acquisition (18 frames, 5 mins per frame) was obtained over the mid-sternum region of the lung, followed by a 10 min acquisition at three bed positions: mid-sternum and sections immediately above and below. Using an external source of 137Cs, a transmission scan to correct for tissue attenuation was obtained at the end of imaging with the patient in the same supine position.
A region of interest (ROI) was drawn on the mid-transaxial slice, defining the right lung on the transmission scan. This ROI was then transferred to the emission scan, where the mean radioactivity in the area was calculated at 12 time points (over 0–60 mins, at 5‐min intervals) for all slices. A simple, noninvasive method, previously validated in the Department of Nuclear Medicine, McMaster University, ON, Canada, was used to determine plasma activity 27, 28. The plasma 18F levels were estimated by drawing an ROI around a vein in the shoulder region. As, 18FDG equilibrates instantaneously between the plasma and red blood cells, the distribution ratio is close to unity and the time-activity curves in whole blood and plasma are identical 28. Time activity-curves were constructed using these data.
The cumulative rate of 18FDG uptake in the extravascular tissue was calculated using all transaxial slices within the right lung. The serial measurements of the ratio of regional accumulation of 18F in the lung fields, compared with plasma 18F concentrations over the 90-min dynamic scan time, were used in a graphical analysis 29. The serial measurements of the ratio of regional lung tissue to plasma 18F concentration (normalised activity) were drawn in a Patlak plot against the ratio of cumulative to instantaneous plasma 18F over the 90-min period after the intravenous 18FDG infusion (normalised time) 29. The slope of this line is equal to the rate constant (ki) for the metabolic trapping of FDG in the lungs (mL·g−1·h−1); ki is converted to glucose utilisation (µmol·g−1·h−1) by multiplying it by the mean plasma concentration of stable glucose (representative value of 4.6 µmol·mL−1) 18.
Data analysis
The rate of accumulation of 18FDG was plotted and the ki were compared pre- and postantibiotic therapy for each subject using the paired t‐test. All statistical tests were two-sided and significance was accepted at the level of 95%. Sputum neutrophil counts are not normally distributed and were therefore expressed as median and interquartile range (IQR) and compared pre- and postantibiotic therapy using the nonparametric Wilcoxon signed-rank test. The correlation between the 18FDG uptake and neutrophil counts was calculated using Spearman's correlation coefficient (rs).
Results
The characteristics of the 10 CF patients and three control (clinically inactive sarcoidosis) subjects are presented in table 1⇓. Two CF patients had diabetes mellitus. In patients with diabetes, it has been shown that administration of 18FDG does not adversely affect their insulin therapy and neither does 18FDG uptake 30. A total of four CF patients were receiving inhaled steroid therapy, although no patients were prescribed recombinant human deoxyribonuclease treatment. From the 10 CF patients enlisted, two did not complete the study; one withdrew after their first visit and one had an acute exacerbation secondary to a respiratory infection.
Cystic fibrosis (CF) and control (sarcoidois) subject characteristics
Representative images for one transaxial tomographic slice in the thorax region of a CF patient are shown in figure 1⇓. Corresponding activity curves in the blood and the right lung are shown in figure 2⇓. The Patlak plot for the lung of the same patient is shown in figure 3⇓. There appears to be no significant accumulation of 18FDG in the lung regions, ki was calculated at 0.49 mL·g−1·h−1. Similar results were found in all CF patients.

Positron emission tomography scan in a female cystic fibrosis patient aged 26 yrs (patient 8). a) The transmission showing the density distribution within the thorax with the lung (low density) in contrast to the heart and chest wall (high density). Patchy areas of increased density are visible throughout the lung. b) The emission scan showing the distribution of radioactivity after intravenous infusion of 18F‐2‐fluoro‐2‐deoxy‐d‐glucose (18FDG). Despite the high-sputum neutrophil count (18.0×106 cells·mL−1 sputum), the image shows no significant accumulation of 18FDG in the lung region. Typical uptake of 18FDG is seen in the heart wall.

a) Representative time-activity curve during the 90-min positron emission tomography scan for a female cystic fibrosis patient aged 26 yrs (patient 8). •: activity in vein; ○: activity in right lung. b) Quantification of radioactive counts accumulated for 12 5-min frames in the regions of interest drawn over the right lung and vein are shown.
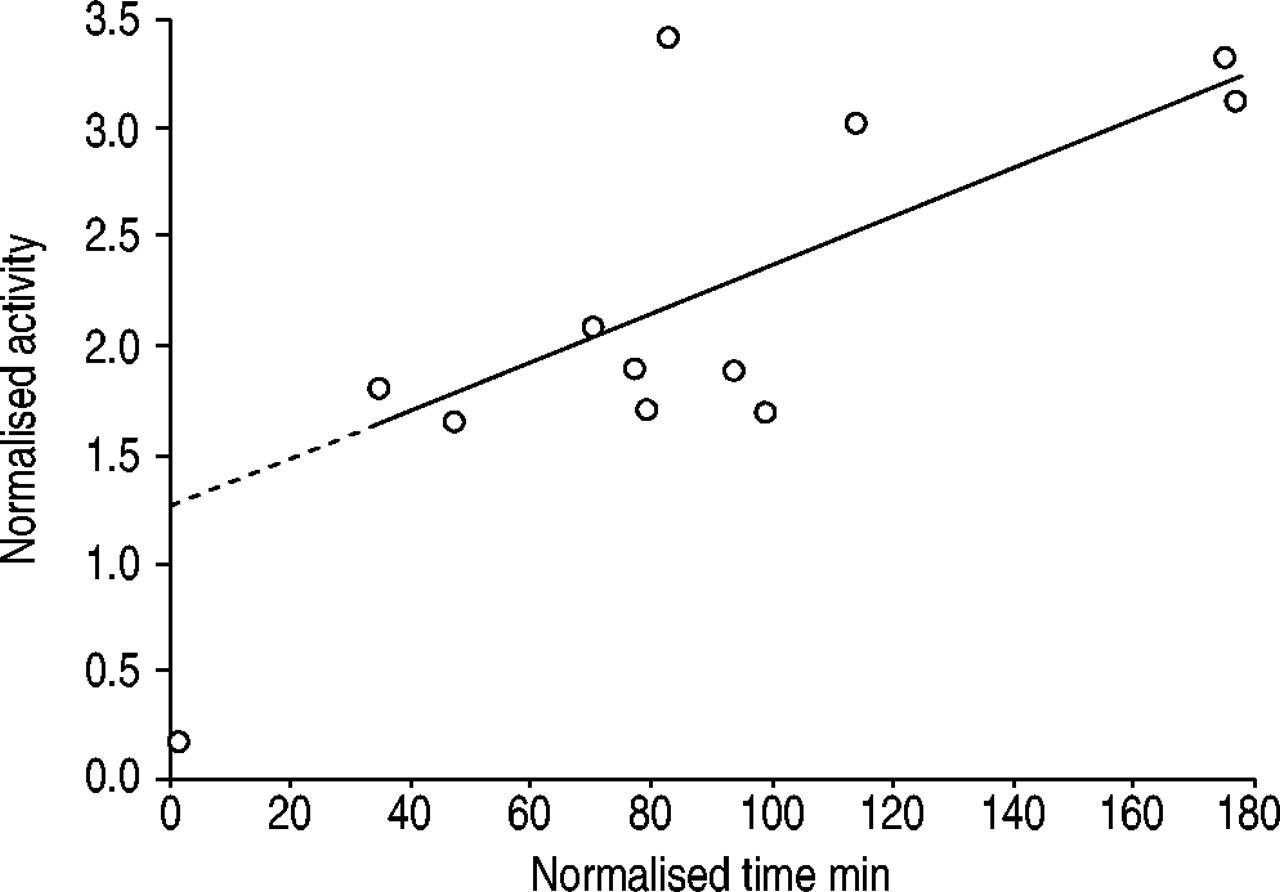
Example of the Patlak plots of the right lung reconstructed from the region of interest data for a female cystic fibrosis patient aged 26 yrs (patient 8). The slope of the curve represents a rate of 18F‐2‐fluoro‐2‐deoxy‐d‐glucose uptake (ki) of 0.49 mL·g−1·h−1. The dashed line shows the extrapolation.
Glucose utilisation in the lung is presented in table 2⇓. The mean rate of glucose utilisation was 1.33 µmol·g−1·h−1 (95% confidence interval (CI) 0.55–2.10) in CF. By comparison, the mean rate of glucose utilisation in the three sarcoidosis subjects was 2.82 µmol·g−1·h−1 (95% CI 2.65–2.99). The median sputum neutrophil count in CF was 13.5×106 cells·mL−1 sputum (IQR 16.1) or 96% of the total cell count (IQR 3.5). No correlation was found between the rate of glucose utilisation in the lung and sputum-neutrophil levels (rs=−0.15, p=0.70) and bacterial density (Pearson's correlation coefficient (r)=0.50, p=0.39) or between glucose utilisation and lung function (r=0.37, p=0.30) in CF patients. However, a negative correlation was found between glucose utilisation and disease severity (rs=−0.66, p=0.04) suggesting that patients with mild lung disease (forced expiratory volume in one second (FEV1) >60% predicted) have a higher rate of glucose utilisation than those with moderate/severe disease (FEV1 ≤60% pred).
18F‐2‐fluoro‐2‐deoxy‐d‐glucose (18FDG) uptake in the lungs of cystic fibrosis (CF) patients and control (sarcoidosis) subjects
There appeared to be no consistent change in 18FDG uptake after antibiotic treatment (fig. 4⇓). No correlation was found between the change in glucose utilisation rates and the change in sputum neutrophil values (rs=0.29, p=0.53; fig. 5⇓).

Glucose utilisation of the right lung, pre- and post-28 days of inhaled tobramycin therapy 160 mg b.i.d. (•). Cystic fibrosis mean glucose utilisation in the lung (♦: 1.3 µmol·g−1·h−1, 95% confidence interval (CI) 0.55–2.10; n=8), Sarcoidosis mean glucose utilisation in the lung (⋄: 2.8 µmol·g−1·h−1, 95% CI 2.65–2.99; n=3). The area between the dashed lines represents normal glucose utilisation in the lung of 1.2 µmol·g−1·h−1 (95% CI 0.94–1.46).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in glucose utilisation versus change in sputum neutrophil counts after 28 days of inhaled tobramycin 160 mg b.i.d. therapy. No correlation was found (rs=0.29, p=0.53).
Discussion
In CF, airway inflammation is characterised by a marked neutrophil influx, high concentrations of pro-inflammatory cytokines for example interleukin (IL)‐8 and proteases, such as neutrophil elastase 14. Neutrophils accounted for 96% of the sputum total cell count (TCC) of 106 cells·mL−1 sputum. These values are similar to the authors' previous findings, where the median sputum neutrophil level was 12.9×106 cells·mL−1 sputum, or 95% of TCC in adult CF patients 31, 32. Despite the presence of high levels of neutrophils in the airways of CF patients, the authors found that the majority of CF patients had normal or slightly depressed rates of glucose metabolism, with a mean metabolic rate for glucose (MRglu) of 1.33 µmol·g−1·h−1 (95% CI 0.55–2.10). In normal lung tissue, glucose utilisation is 1.2 µmol·g−1·h−1 (95% CI 0.95–1.46) 33. The rate of glucose utilisation did not correlate with lung function, lung inflammation or bacterial density.
A similar finding has been reported in patients with bronchiectasis who showed little increase in glucose metabolism. Bronchiectasis is analogous to CF in that patients are chronically infected with P. aeruginosa, produce copious amounts of mucopurulent sputum that are difficult to clear and have a persistent airway inflammatory response, which leads to a vicious cycle of inflammation, tissue destruction and respiratory infection 34. Jones et al. 19 examined the relation of metabolic activity to neutrophil emigration in pneumonia and bronchiectasis by measuring 111In-labelled granulocyte emigration into the lungs by γ‐scintigraphy. The group also measured neutrophil activity by PET and injected 18FDG. Neutrophil emigration was evident in four of the five bronchiectatic patients they examined, a finding similar to other studies 35, 36. Despite the ongoing neutrophil migration into the lungs, minimal neutrophil metabolic activity was detected by 18FDG-PET imaging in bronchiectatic patients.
Uptake of 18FDG has been shown to be above normal in sarcoidosis 37, cryptogenic fibrosing alveolitis 33, pneumonia 8, 20, 33, atopic asthma 9 and neonatal acute lung injury 38, 39. In patients with interstitial lung disease, the mean MRglu was 2.6 µmol·g−1·h−1, reflecting the metabolic activity of the cellular infiltrate associated with the disease 40. Similar data have been collected from patients with active sarcoidosis (mean MRglu 4.1 µmol·g−1·h−1) 37. In the present study's control group, subjects with clinically inactive sarcoidosis had a rate of glucose metabolism above normal (mean MRglu 2.82 µmol·g−1·h−1, 95% CI 2.65–2.99).
The authors' calculations for glucose utilisation were made on the entire right lung. It is possible, that areas of relatively high 18FDG uptake were present but not in high enough levels to influence the average value for the right lung. In three patients (one with severe lung disease, two with mild disease), small areas of high uptake (twice that of the surrounding lung tissue) were observed that corresponded to a dense area on the transmission scan, thought to be mucus. These localised areas were not present at the second PET scan performed following 28 days of antibiotic therapy, despite an insignificant change in the sputum neutrophil counts. The PET scans from the other CF patients did not exhibit this type of finding, indicating that the Patlak results were representative of the events in the entire lung.
Wide variations in 18FDG uptake were observed among CF patients and within patients that were not attributable to varying degrees of sputum neutrophilia, lung function or changes in inflammation. Although no correlation was found between lung function and glucose utilisation, a significant correlation was found with disease severity, suggesting patients with mild disease have an increased utilisation of glucose compared with those having moderate-to-severe disease. This is in contrast to the authors' hypothesis that 18FDG uptake is a measure of lung inflammation, specifically neutrophils, and therefore 18FDG uptake would be positively correlated with the degree of sputum neutrophilia. The authors have shown previously that disease severity correlates with the intensity of sputum neutrophilia 32. Patients with severe lung disease had a significantly higher number of neutrophils residing in their airways than those with mild disease. Several studies have found a similar negative correlation between FEV1 and neutrophil counts 41–43. Bacterial density did not correlate with 18FDG uptake, which was expected, since the authors' laboratory has also demonstrated no correlation between sputum neutrophil counts and P. aeruginosa density (unpublished data), a finding similar to BAL studies by Meyer et al. 42, 44.
There are several possible explanations for this observation in CF. Circulating 18FDG may have been prevented from penetrating into the airway lumen by the presence of increased secretions. The authors did not measure the presence of 18FDG in sputum postimaging. In bronchiectatic patients, Jones et al. 19 did find detectable levels of radioactivity in the sputum immediately following the PET scan. Since bronchiectactic patients have similar lung disease features to CF, it is likely that 18FDG also reaches the airway lumen in CF. The negative correlation between glucose utilisation and disease severity suggests that circulating 18FDG may not be able to penetrate into the airways of those patients with moderate-to-severe lung disease. However, FEV1 (% pred), a more objective measure than the categorical grouping of mild (FEV1 >60% of pred) and moderate-to-severe (FEV1 ≤60% of pred) disease severity did not significantly correlate with glucose utilisation.
Another possible explanation for this observation is that neutrophil activation, or their respiratory burst, is impaired in CF patients. P. aeruginosa persists in the lungs despite heavy accumulation of neutrophils in the airway walls and lumen. This suggests that P. aeruginosa may produce substances that suppress neutrophil activity. The bacteria produced two phospholipase‐C (PLC) molecules, haemolytic and nonhaemolytic. PLC is induced through phosphate starvation as it functions in phosphate-scavenging pathways. Gram-negative pathogens, for example P. aeruginosa, have suboptimal circulating phosphate levels, therefore, PLC is likely to be induced in the CF lung. Terada et al. 45 demonstrated that haemolytic PLC potently suppresses the neutrophil respiratory burst response to bacteria, measured as the rate and amount of oxygen produced. Large quantities of glucose are metabolised during the respiratory burst 46 and when the respiratory burst is inhibited, glucose uptake is also inhibited 47. Therefore, if the neutrophil respiratory burst is inhibited by haemolytic PLC, 18FDG accumulation in the lung would not occur.
A third hypothesis is that neutrophils are dying upon emigration into the lung. In vitro evidence suggests that P. aeruginosa induces neutrophil cell death differently from apoptosis. Dacheux et al. 48 showed that coincubation of neutrophils, isolated from human peripheral blood with a CF P. aeruginosa isolate, resulted in neutrophil death starting 30 min after infection with 80% of cell lysis occurring within 3 h. Cell death, referred to as oncosis, is characterised by cellular and nuclear swelling, blebbing, vacuolisation and disintegration of the cell membrane. The authors demonstrated that the cytotoxicity of P. aeruginosa requires a functional type-III secretion, Exo U‐independent system which delivers toxins directly into adjacent host cells. Type-III secretion systems are conserved in many Gram-negative organisms 49. An isogenic mutant of a CF P. aeruginosa isolate, in which the type-III secretion system was nonfunctional, was unable to induce cellular death of neutrophils suggesting oncosis is a type-III secretion-dependent event. If neutrophils are undergoing oncosis, their activation process would not be complete. As a result, glucose metabolism may not be increased. However, their cellular contents, including neutrophil elastase, would be released and available to cause lung damage but phagocytosis of P. aeruginosa would not occur, leading to the persistent respiratory infection that is seen in CF and in bronchiectactic patients.
In the eight patients that underwent a PET scan before and after 28 days of inhaled tobramycin, no change in glucose metabolism was observed. In addition no change in sputum inflammatory indices were found, indicating that this antibiotic therapy may not have an anti-inflammatory effect. As a result, the authors could not determine if 18FDG uptake was sensitive to changes in airway inflammation in CF. A previous study of patients with active sarcoidosis found a 69% reduction in MRglu from mean±sd 4.56±1.33 to 1.43±0.11 µmol·g−1·h−1, after treatment with high-dose prednisone 37. In a longitudinal study of patients with cryptogenic fibrosing alveolitis, MRglu appeared to be predictive of their clinical condition 33. The authors found that if MRglu remained high over the first year or rose from normal to the high range, the patient's clinical condition deteriorated. If MRglu remained in the normal range, the patient's condition remained stable or sometimes improved. These data suggest that 18FDG-PET imaging could be used to monitor disease progression and the efficacy of anti-inflammatory agents in respiratory diseases other than CF and bronchiectasis.
In summary, the results of this study showed that 18F‐2‐fluoro‐2‐deoxy‐d‐glucose positron emission tomography imaging is not useful for the detection and monitoring of lung inflammation in cystic fibrosis. However, the results raise interesting questions with regard to the effectiveness of the host immune system in the lungs of cystic fibrosis patients who are chronically infected with Pseudomonas aeruginosa. It is believed that the inflammatory response is defective and overwhelmed, however, this is the first observation in situ that suggests the lung neutrophils may not be functioning normally.
Acknowledgments
The authors would like to thank F.E. Hargreave and A. Efthimiadis for performing the sputum examination and their insightful comments on the results, and R. Hennessey and G. Cox for their help during patient recruitment.
- Received July 18, 2002.
- © ERS Journals Ltd









