
Abstract
Background: Positron emission tomography (PET) is a noninvasive imaging modality that can detect malignant lymph nodes. This study determined the sensitivity, specificity, predictive values, and likelihood ratios of PET scanning compared with standard axillary lymph node dissection (ALND) and sentinel lymph node biopsy (SLNB) in staging the axilla in women with early stage breast cancer.
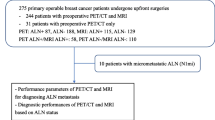
Methods: Women with clinical stage I or II breast cancer had whole body PET scanning before ALND and SLNB, in a prospective, blinded protocol. ALND were evaluated by standard hematoxylin and eosin (H&E) staining techniques, while sentinel nodes were also examined for micrometastatic disease.
Results: A total of 98 patients were recruited. PET compared with ALND demonstrated sensitivity of 0.40 (95% CI, 0.16, 0.68), specificity 0.97 (CI, 0.90, 0.99), positive likelihood ratio 14.4 (CI, 3.21, 64.5), positive predictive value 0.75 (CI, 0.35, 0.97), and false–negative rate of 0.60 (CI, 0.32, 0.84). Test properties were similar for PET compared with sentinel nodes positive by H&E staining. A few false–positive scans (0.028, CI, 0.003, 0.097) were seen. Multiple logistic regression analysis found that PET accuracy was better in patients with high grade and larger tumors. Increased size and number of positive nodes were also associated with a positive PET scan.
Conclusions: The sensitivity of PET compared with ALND and SLNB was low, whereas PET scanning had high specificity and positive predictive values. The study suggests that PET scanning cannot replace histologic staging in early stage breast cancer. The low rate of false–positive findings suggests that PET can identify women who can forego SLNB and require full axillary dissection.
Similar content being viewed by others


REFERENCES
Taneja C, Gardner B. Complications of axillary dissection. In: Bland K, E Copeland, eds. The Breast: Comprehensive Management of Benign and Malignant Disease. WB Saunders: New York, 1998;954–61.
Gross P, Hack T, Cohen L. Long-term morbidity of axillary dissection in patients with breast cancer. Breast Cancer Res Treat 1997;41:271.
Liljegrem F, Holenberg L and the Uppsala-Orebro breast cancer study group. Arm morbidity after sector resection and axillary dissection with or without post-operative radiotherapy in breast cancer. Eur J Cancer 1997;33:193–9.
Ververs JM, Roumen RM, Vingerhoets AJ, et al. Risk, severity and predictors of physical and psychological morbidity after axillary lymph node dissection for breast cancer. Eur J Cancer 2001;37:991–9.
Hack TF, Cohen L, Katz J, Robson LS, Goss P. Physical and psychological morbidity after axillary lymph node dissection for breast cancer. J Clin Oncol, 1999;17:143–9.
Cohen L, Hack TF, de Moor C, Katz J, Goss PE. The effects of type of surgery and time on psychological adjustment in women after breast cancer treatment. Ann Surg Oncol 2000;7:427–34.
Velanovich V, Szymanski W. Quality of life of breast cancer patients with lymphedema. Am Surg 1999;177:184–7, discussion 188.
Chadha M, Axelrod D. Is axillary dissection always indicated in invasive breast cancer?. Oncology 1997;11:1463–76.
Haffty BG, Ward B, Pathare P, et al. Reappraisal of the role of axillary lymph node dissection in the conservative treatment of breast cancer. J Clin Oncol 1997;15:691–700.
Cedt B. Is ALND necessary in routine management of breast cancer? Imp Adv Onc 1996;251–6.
Giuliano AE, Barth AM, Spivak B, et al. Incidence and predictors of metastasis in T1 carcinoma of the breast. J Am Coll Surg 1996;183:262–4.
Singhal H, O’Malley FP, Tweedie E, Stitt L, Tonkin KS. Axillary dissection in patients with breast cancer diagnosed through Ontario breast screening program: a need for minimally invasive techniques. Can J Surg 1997;40:377–82.
Temple LK, Baron R, HS Cody 3rd, et al. Sensory morbidity after sentinel lymph node biopsy and axillary dissection: a prospective study of 233 women. Ann Surg Oncol 2002;9:654–62.
Roumen RM, Kuijt GP, Liem IH, van Beek MW. Treatment of 100 patients with sentinel node-negative breast cancer without further axillary dissection. Br J Surg 2001;88:1639–43.
Schrenk P, Rieger R, Shamiyeh A, Wayand W. Morbidity following sentinel lymph node biopsy versus axillary lymph node dissection for patients with breast carcinoma. Cancer 2000;88:608–14.
Giuliano AE, Haigh PI, Brennan MB, et al. Prospective observational study of sentinel lymphadenectomy without further axillary dissection in patients with sentinel node-negative breast cancer. J Clin Oncol 2000;18:2553–9.
Giuliano AE. Current status of sentinel lymphadenectomy in breast cancer. Ann Surg Oncol 2001;8:52–5.
Coleman ER. Clinical PET in oncology. Clin Pos Imag 1998;1:15–30.
Wahl RL. Current status of PET in breast cancer imaging, staging, and therapy. Semin Roent 2001;36:250–60.
Guller U, Nitzsche E, Moch H, Zuber M. Is positron emission tomography an accurate non-invasive alternative to sentinel lymph node biopsy in breast cancer patients?. J Natl Cancer Inst 2003;95:1040–3.
Skehan SJ, Coates G, Otero C, O’Donovan N, Pelling M, Nahmias C. Visual and semiquantitative analysis of 18F-fluorodeoxyglucose positron emission tomography using a partial-ring tomography without attenuation correction to differentiate benign and malignant pulmonary nodules. Can Assoc Radiol J 2001;52:259–65.
Bass SS, Cox CE, Ni KN, Berman C, Reintgen DS. The role of sentinel lymph node biopsy in breast cancer. J Am Coll Surg 1999;189:183–94.
Archibald S, Bhandari M, Thoma A. Users’ guides to the surgical literature: how to use an article about a diagnostic test. Can J Surg 2001;44:17–23.
Jaeschke R, Guyatt G, Sachett DL. Users’ guides to the medical literature: how to use an article about a diagnostic test. B. What are the results and will they help me in caring for my patients?. JAMA 1994;271:703–7.
Wahl RL, Cody RL, Hutchins GD, Mudgett EE. Primary and metastatic breast carcinoma: initial clinical evaluation with PET with the radiolabeled glucose analogue 2-[F-18]-fluoro-2-deoxy-D-glucose. Radiology 1991;179:765–70.
Adler LP, Crowe JP, al-Kaisi NK, Sunshine JL. Evaluation of breast masses and axially lymph nodes with [F-18] 2-deoxy-2-fluoro-D-glucose PET. Radiology 1993;187:743–50.
Utech CI, Young CS, Winter PF. Prospective evaluation of fluorine-18 fluorodeoxyglucose positron emission tomography in breast cancer for staging of the axilla related to surgery and immunocytochemistry. Eur J Nucl Med 1996;23:1588–93.
Adler LP, Faulhaber PF, Schnur KC, Al-Kasi NL, Shenk RR. Axillary lymph node metastases: screening with [F-18]2-deoxy-2-fluoro-D-glucose (FDG) PET. Radiology 1997;203:323–7.
Smith IC, Ogston KN, Whitford P, et al. Staging of the axilla in breast cancer: Accurate in vivo assessment using positron emission tomography with 2-(fluorine-18)-fluoro-2-deoxy-D-glucose. Ann Surg 1998;228:220–7.
DN Danforth Jr., Aloj L, Carrasquillo JA, et al. The role of 18F-FDG-PET in the local/regional evaluation of women with breast cancer. Breast Cancer Res Treat 2002;75:35–46.
Greco M, Crippa F, Agresti R, et al. Axillary lymph node staging in breast cancer by 2-fluoro-2-deoxy-D-glucose-positron emission tomography: clinical evaluation and alternative management. J Natl Cancer Inst 2001;93:630–5.
Schirrmeister H, Kuhn T, Guhlmann A, et al. Fluorine-18 2-deoxy-2-fluoro-D-glucose PET in the preoperative staging of breast cancer: comparison with the standard staging procedures. Eur J Nucl Med 2001;28:51–8.
Guller U, Nitzsche EU, Schirp U, et al. Selective axillary surgery in breast cancer patients based on positron emission tomography with 18F-fluoro-2-deoxy-D-glucose: not yet!. Breast Cancer Res Treat 2002;71:171–3.
Kelemen PR, Lowe V, Phillips N. Positron emission tomography and sentinel lymph node dissection in breast cancer. Clin Breast Cancer 2002;3:73–7.
van der Hoeven JJ, Hoekstra OS, Comans EF, et al. Determinants of diagnostic performance of [F-18] fluorodeoxyglucose positron emission tomography for axillary staging in breast cancer. Ann Surg 2002;236:619–24.
Avril N, Rose CA, Schelling M, et al. Breast imaging with positron emission tomography and fluorine-18 fluorodeoxyglucose: use and limitations. J Clin Oncol 2000;18:3495–502.
Rostom AY, Powe J, Kandil A, et al. Positron emission tomography in breast cancer: a clinicopathological correlation of results. Br J Radiol 1999;72:1064–8.
Bleckmann C, Dose J, Bohuslavizki KH, et al. Effect of attenuation correction on lesion detectability in FDG PET of breast cancer. J Nucl Med 1999;40:2021–4.
Nakamoto Y, Chang AE, Zasadny KR, Wahl RL. Comparison of attenuation-corrected and non-corrected FDG-PET images for axillary nodal staging in newly diagnosed breast cancer. Mol Imaging Biol 2002;4:161–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lovrics, P.J., Chen, V., Coates, G. et al. A Prospective Evaluation of Positron Emission Tomography Scanning, Sentinel Lymph Node Biopsy, and Standard Axillary Dissection for Axillary Staging in Patients with Early Stage Breast Cancer. Ann Surg Oncol 11, 846–853 (2004). https://doi.org/10.1245/ASO.2004.11.033
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1245/ASO.2004.11.033