
Abstract
Background:
The aim of this prospective study was to examine whether discontinuation of proton pump inhibitors (PPIs) or replacement by H2-receptor antagonists (H2RA) resulted in a decrease of chromogranin A (CgA) levels in 196 patients with well-differentiated neuroendocrine tumours (NETs).
Methods:
Patients with an unexpectedly high CgA level not connected with NET disease discontinued PPIs, or used H2RA instead; 2 weeks later CgA level was measured again.
Results:
In all, 19 out of 196 (10%) patients showed unexpected elevated CgA levels, they all used PPI. In 11 out of 19 patients with no evidence of the disease, median CgA decreased from 390 μg l−1 during PPI treatment to 56 μg l−1 after discontinuation (P=0.003). In 8 out of 19 patients with stable disease, median CgA decreased from 618 to 318 μg l–1 (P=0.012). In 12 out of 19 patients who ceased all acid inhibition, CgA levels decreased by 82%, while in the seven patients who replaced PPI by H2RA, CgA decreased by 77% (P=0.967).
Conclusion:
Proton pump inhibitor use causes falsely elevated CgA levels in patients with NET. We recommend to stop, or replace PPI by H2RA, to obtain a reliable CgA value.
Similar content being viewed by others


Main
Well-differentiated neuroendocrine tumours (NETs) are rare, slow-growing tumours. Chromogranin A (CgA) has replaced the 24-h urine collection of 5-hydroxyindoleacetic acid and has become the most important tumour marker in the monitoring of NET during and after treatment and is recommended by the European NeuroEndocrine Tumor Society (Korse et al, 2009; O'Toole et al, 2009). Chromogranin A is localised in the secretory granules of the neuroendocrine cells. Chromogranin A levels may also be elevated in other disease processes, such as prostate cancer, liver failure, cardiovascular diseases and renal failure (Tramonti et al, 2001; Modlin et al, 2010; Vezzosi et al, 2011). However, the use of proton pump inhibitors (PPIs) is the most important reason for an elevated CgA level, not caused by NET (Modlin et al, 2010). Thus far, the effect of discontinuation of PPI therapy was not investigated. This study examines whether discontinuation of PPI treatment, or replacement by H2-receptor antagonist (H2RA) therapy, decreases or even normalises the unexplained elevation of CgA levels in patients with well-differentiated NET.
Materials and methods
For this prospective study, all patients diagnosed with well-differentiated NET visiting the Netherlands Cancer Institute between 2007 and 2009 with at least two available CgA measurements, were examined. Clinical data and medication were retrieved from medical records. Stage of disease was based on CT scans, or somatostatin receptor scintigraphy. Chromogranin A was determined with the CGA-RIA, a solid-phase, two-site immunoradiometric (CIS bio International, Gif-sur-Yvette, France) (Degorce et al, 1999; Korse et al, 2009). The reference value in our laboratory was established as <120 μg l−1.
All patients with a normal CgA level during the study period were excluded from further examination. Patients with elevated CgA levels showing metastases or tumour progression were also excluded from further observation; these elevated CgA levels were attributed to tumour activity only. If patients showed elevated or increasing CgA levels that could not be attributed to the status of NET, the gastric acid inhibition treatment was registered. Those patients with unexpected elevated CgA levels and using PPI were asked to (temporarily) discontinue the PPI or to (temporarily) replace the PPI by H2RA treatment. After 2 weeks, the CgA level was measured again.
Wilcoxon paired tests and Mann–Whitney tests were applied to compare the CgA levels just before and 14 days after PPI discontinuation, and to compare change in CgA levels between patients who discontinued any acid suppressing therapy and patients who replaced PPI by H2RA. A change of >40% was considered as a significant change in the comparison of serial measurements (Dittadi et al, 2004).
Results
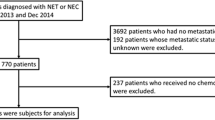
Table 1 presents the characteristics of 196 patients at the time of the first CgA measurement: a total of 55 patients showed normal CgA levels and 122 patients had at least one elevated CgA level that was attributed to the status of the disease, according to imaging; these patients were not monitored longer for this study.
The remaining 19 patients had elevated CgA levels that could not be attributed to the disease status: 11 patients with no evidence of disease (NED) after surgery and eight patients with stable metastatic disease (SD) (Table 2). All these patients used PPI (omeprazole 20–40 mg daily) for dyspepsia or pyrosis, mainly prescribed by their general practitioner. In case of severe pyrosis, PPI was replaced by H2RA (ranitidine 300 mg daily, n=7). The remaining patients discontinued the acid inhibition completely (n=12). All 19 patients experienced no discomfort from this temporary cease of PPI use.
In the 11 patients with NED, the median CgA level decreased from 390 μg l–1 during PPI treatment to 56 μg l–1 after discontinuation of PPI (P=0.003). At that time, nine patients showed normal CgA levels, while in two patients (patients 6 and 7), the CgA levels decreased by 81% and 89%, respectively. The eight patients with SD according to imaging, showed unexpected increase of CgA levels. After discontinuation of PPI, the median CgA level decreased from 618 μg l–1 during PPI use to 318 μg l–1 (P=0.012). In two patients (patients 16 and 19), CgA levels even normalised.
All patients except two (patients 15 and 18) reached the critical difference of CgA change of >40% (33% and 35%, respectively). In 12 of the 19 patients with unexpected positive CgA levels who stopped all acid inhibition completely, CgA levels decreased by (median) 82% (range 33–89%). A similar trend was found in the seven patients who replaced PPI by H2RA: their CgA levels decreased by 77% (range 72–86%) (P=0.967).
Discussion
In this study, we investigated the association of CgA levels and use of PPIs in patients treated for NET. High CgA levels were observed in 19 of the 196 (10%) patients, which could not be explained by tumour recurrence or progressive disease. All these patients were PPI users. An association between CgA levels and the use of PPI has already been described: a Dutch group published a cross-sectional study of 114 dyspeptic patients and showed that CgA levels were higher during long-term PPI treatment than during H2RA treatment, or no treatment (Sanduleanu et al, 1999). Giusti et al (2004) observed in six of seven patients a significant decrease of CgA levels after discontinuation of omeprazole. These studies suggested that decrease in acidity leads to release of gastrin. Elevated gastrin leads to hyperplasia of ECL cells and, subsequently, to an increase in CgA levels (Waldum et al, 1996; Sanduleanu et al, 1999). However, longitudinal studies investigating the effect of PPIs on CgA levels in patients with NET are lacking. In our group of NET patients, the elevated CgA levels significantly decreased, or even returned to normal, after discontinuation of gastric acid inhibition completely. A similar decrease was observed after replacement of PPI by H2RA.
A discontinuation of PPI of 2 weeks seemed a reasonable period in which to expect a decrease, similar to the report of Giusti et al. However, two patients (patients 6 and 7) with CgA levels >10 times the upper limit of normal showed an 81–89% decrease, but did not reach the normal range. Possibly, in patients with such extreme high values, a longer discontinuation is needed. It has also been suggested that cytochrome P450 2C19 (CYP2C19) might have a role in the metabolising of PPI. Even a five-fold higher exposure to PPIs has been observed in poor metabolisers (PMs) than in extensive metabolisers of CYP2C19 (Desta et al, 2002; Giusti et al, 2004). As the prevalence of PMs in Caucasian people is 1–3%, in some cases, the CgA could still be false positive after 2 weeks of discontinuation.
The two patients (patients 15 and 18) achieved a decrease <40%. Their CgA levels returned back to the precious levels (data not shown). Apparently, the CgA results were explained by both NET disease and PPI use. Since both the biological and assay variation of CgA, NET disease and PPI use might affect the CgA concentration, it is of crucial importance to stop PPI, to exclude the PPI influence on CgA levels. Patient 18 with liver metastases suffered also from renal failure (glomerular filtration rate=36 ml per minute per 1.73 m2), but even then the CgA level decreased with 35% (Modlin et al, 2010).
Of the 122 patients, 24 (20%) with high CgA levels used PPI. Examination of the medical reports showed that the concentration of CgA levels was fully attributed to the disease. In the group of 55 patients with normal CgA levels, 5 (9%) were PPI users. The duration of PPI use of these patients was unknown, but Sanduleanu et al (1999) suggested that the longer the use of PPI, the higher the CgA levels will be. In the future, all patients should discontinue PPI use in order to obtain a reliable CgA level, irrespective of tumour activity or duration of PPI use.
In our study population, there was no difference in CgA (percentage) decrease between patients who stopped acid inhibition completely and patients who replaced their PPI by H2RA. The use of H2RA did not affect the CgA levels, in contrast to PPI use. Proton pump inhibitor is a therapy that almost completely suppresses gastric acid. This is achieved by influencing the enzyme H+/K+-ATP-ase of the parietal cells (gastric proton pump). This acid suppression leads to an increase of gastrin, which is a trophic factor for hyperplasia of ECL cells. Apparently, the use of H2RA did not cause such hyperplasia of the ECL cells in this group of patients that it may lead to an increase of CgA. Although our H2RA group is relatively small, this finding confirms the results of Driman et al (1996) who reported increased parietal cell height, mass and number in omeprazole-treated patients compared with ranitidine-treated patients.
In conclusion, we recommend to cease or replace PPI by H2RA, to obtain a reliable value of CgA. A discontinuation of 2 weeks is usually sufficient.
Change history
29 March 2012
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Degorce F, Goumon Y, Jacquemart L, Vidaud C, Bellanger L, Pons-Anicet D, Seguin P, Metz-Boutigue MH, Aunis D (1999) A new human chromogranin A (CgA) immunoradiometric assay involving monoclonal antibodies raised against the unprocessed central domain (145-245). Br J Cancer 79: 65–71
Desta Z, Zhao X, Shin JG, Flockhart DA (2002) Clinical significance of the cytochrome P450 2C19 genetic polymorphism. Clin Pharmacokinet 41: 913–958
Dittadi R, Meo S, Gion M (2004) Biological variation of plasma chromogranin A. Clin Chem Lab Med 42: 109–110
Driman DK, Wright C, Tougas G, Riddell RH (1996) Omeprazole produces parietal cell hypertrophy and hyperplasia in humans. Dig Dis Sci 41: 2039–2047
Giusti M, Sidoti M, Augeri C, Rabitti C, Minuto F (2004) Effect of short-term treatment with low dosages of the proton-pump inhibitor omeprazole on serum chromogranin A levels in man. Eur J Endocrinol 150: 299–303
Korse CM, Bonfrer JM, Aaronson NK, Hart AA, Taal BG (2009) Chromogranin A as an alternative to 5-hydroxyindoleacetic acid in the evaluation of symptoms during treatment of patients with neuroendocrine tumors. Neuroendocrinology 89: 296–301
Modlin IM, Gustafsson BI, Moss SF, Pavel M, Tsolakis AV, Kidd M (2010) Chromogranin a-biological function and clinical utility in neuro endocrine tumor disease. Ann Surg Oncol 17: 2427–2443
O'Toole D, Grossman A, Gross D, Delle Fave G, Barkmanova J, O′Connor J, Pape UF, Plockinger U (2009) ENETS Consensus guidelines for the standards of care in neuroendocrine tumors: biochemical markers. Neuroendocrinology 90: 194–202
Sanduleanu S, Stridsberg M, Jonkers D, Hameeteman W, Biemond I, Lundqvist G, Lamers C, Stockbrugger RW (1999) Serum gastrin and chromogranin A during medium- and long-term acid suppressive therapy: a case-control study. Aliment Pharmacol Ther 13: 145–153
Tramonti G, Ferdeghini M, Annichiarico C, Norpoth M, Donadio C, Bianchi R, Bianchi C (2001) Relationship between renal function and blood level of chromogranin A. Ren Fail 23: 449–457
Vezzosi D, Walter T, Laplanche A, Raoul JL, Dromain C, Ruszniewski P, d′Herbomez M, Guigay J, Mitry E, Cadiot G, Leboulleux S, Lombard-Bohas C, Borson-Chazot F, Ducreux M, Baudin E (2011) Chromogranin A measurement in metastatic well-differentiated gastroenteropancreatic neuroendocrine carcinoma: screening for false positives and a prospective follow-up study. Int J Biol Markers 26: 94–101
Waldum HL, Arnestad JS, Brenna E, Eide I, Syversen U, Sandvik AK (1996) Marked increase in gastric acid secretory capacity after omeprazole treatment. Gut 39: 649–653
Acknowledgements
We thank Dr H Boot and Dr JMG Bonfrer (both from the Netherlands Cancer Institute) for their critical review of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Korse, C., Muller, M. & Taal, B. Discontinuation of proton pump inhibitors during assessment of chromogranin A levels in patients with neuroendocrine tumours. Br J Cancer 105, 1173–1175 (2011). https://doi.org/10.1038/bjc.2011.380
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2011.380
Keywords
This article is cited by
-
Predictive Value of Chromogranin A and a Pre-Operative Risk Score to Predict Recurrence After Resection of Pancreatic Neuroendocrine Tumors
Journal of Gastrointestinal Surgery (2019)
-
Serum chromogranin-A-based prognosis in metastatic castration-resistant prostate cancer
Prostate Cancer and Prostatic Diseases (2018)
-
Advances in the diagnosis and treatment of pancreatic neuroendocrine neoplasms in Japan
Journal of Gastroenterology (2017)
-
Italian Association of Clinical Endocrinologists (AME) position statement: a stepwise clinical approach to the diagnosis of gastroenteropancreatic neuroendocrine neoplasms
Journal of Endocrinological Investigation (2014)
