
Abstract
Objective
The purpose of this study was to evaluate 18F-FDG-PET, PET/CT, and CT in the diagnosis of benign or malignant solitary pulmonary nodules (SPNs) in areas with a high incidence of TB.
Methods
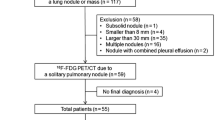
Ninety-six patients with a SPN smaller than 30 mm were studied prospectively. PET/CT images were obtained 60 min after intravenous injection of 18F-FDG. The data obtained for each patient were analyzed and the accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated and compared using χ2 test.
Results
The sensitivity, specificity, accuracy, PPV, and NPV in the diagnosis of SPN were 86.7, 72.2, 81.3, 83.9, and 76.5%, respectively, for CT and 88.3, 61.1, 79.1, 79.1, and 75.9%, respectively, for PET. Tuberculosis was responsible for 57.1% (8/14) of false-positives on PET. The sensitivity, specificity, accuracy, PPV, and NPV in the diagnosis of SPN were 96.7, 75.7, 88.5, 88.1, and 94.4% for PET/CT. The accuracy of PET/CT was higher than that of either CT or PET alone (P < 0.05).
Conclusion
PET has a high false-positive rate in areas with a high incidence of TB; combined PET and CT (PET/CT) can improve the diagnostic accuracy in the differentiation of an SPN.
Similar content being viewed by others


References
Ost D, Fein AM, Feinsilver SH. The solitary pulmonary nodule. N Engl J Med. 2003;348(25):2535–42.
Winer-Muram HT. The solitary pulmonary nodule. Radiology. 2006;239(1):34–49.
Leef JL, Klein JS. The solitary pulmonary nodule. Radiol Clin North Am. 2002;40(1):123–43.
Klein JS, Braff S. Imaging evaluation of the solitary pulmonary nodule. Clin Chest Med. 2008;29(1):15–38.
Zhuang H, Alavi A. 18-Fluorodeoxyglucose positron emission tomographic imaging in the detection and monitoring of infection and inflammation. Semin Nucl Med. 2002;1(32):47–59.
Rosenbaum S, Lind T, Antoch G, Bockisch A. False-positive FDG PET uptake—the role of PET/CT. Eur Radiol. 2006;16(5):1054–65.
Jeong SY, Lee KS, Shin KM, Bae YA, Kim B-T, Choe BK, et al. Efficacy of PET/CT in the characterization of solid or partly solid solitary pulmonary nodules. Lung Cancer. 2008;61(2):186–94.
Glaziou P, Floyd K, Raviglione M. Global burden and epidemiology of tuberculosis. Clin Chest Med. 2009;30(4):621–36.
Fletcher JW, Kymes SM, Gould M, Alazraki N, Coleman RE, Lowe VJ, et al. A comparison of the diagnostic accuracy of 18F-FDG PET and CT in the characterization of solitary pulmonary nodules. J Nucl Med. 2008;49(2):179–85.
Kim SK, Allen-Auerbach M, Goldin J, Fueger BJ, Dahlbom M, Brown M, et al. Accuracy of PET/CT in characterization of solitary pulmonary lesions. J Nucl Med. 2007;48(2):214–20.
Bakheet SMB, Powe J, Ezzat A, Rostom A. F-18-FDG uptake in tuberculosis. Clin Nucl Med. 1998;23(11):739–42.
Patz EF, Lowe VJ, Hoffman JM, Paine SS, Burrowes P, Coleman RE, et al. Focal pulmonary abnormalities: evaluation with F-18 fluorodeoxyglucose PET scanning. Radiology. 1993;188(2):487–90.
Knight SB, Delbeke D, Stewart JR, Sandler MP. Evaluation of pulmonary lesions with FDG-PET. Chest. 1996;109(4):982–8.
Zhuang H, Pourdehnad M, Lambright ES, Yamamoto AJ, Lanuti M, Li P, et al. Dual time point 18F-FDG PET imaging for differentiating malignant from inflammatory processes. J Nucl Med. 2001;42(9):1412–7.
Riad R, Omar W, Sidhom I, Zamzam M, Zaky I, Hafez M, et al. False-positive F-18 FDG uptake in PET/CT studies in pediatric patients with abdominal Burkitt’s lymphoma. Nucl Med Commun. 2010;31(3):232–8.
Bunyaviroch T, Coleman RE. PET evaluation of lung cancer. J Nucl Med. 2006;47(3):451–69.
Christensen JA, Nathan MA, Mullan BP, Hartman TE, Swensen SJ, Lowe VJ. Characterization of the solitary pulmonary nodule: 18F-FDG PET versus nodule-enhancement CT. Am J Roentgenol. 2006;187(5):1361–7.
Gould MK, Maclean CC, Kuschner WG, Rydzak CE, Owens DK. Accuracy of positron emission tomography for diagnosis of pulmonary nodules and mass lesions: a meta-analysis. JAMA. 2001;285(7):914–24.
Schrevens L, Lorent N, Dooms C, Vansteenkiste J. The role of PET scan in diagnosis, staging, and management of non-small cell lung cancer. Oncologist. 2004;9(6):633–43.
Baldwin DR, Birchall JD, Ganatra RH, Pointon KS. Evaluation of the solitary pulmonary nodule: clinical management, role of CT and nuclear medicine. Imaging. 2004;16(1):22–36.
Bar-Shalom R, Kagna O, Israel O, Guralnik L. Noninvasive diagnosis of solitary pulmonary lesions in cancer patients based on 2-fluoro-2-deoxy-d-glucose avidity on positron emission tomography/computed tomography. Cancer. 2008;113(11):3213–21.
Gould MK, Sanders GD, Barnett PG, Rydzak CE, Maclean CC, McClellan MB, et al. Cost-effectiveness of alternative management strategies for patients with solitary pulmonary nodules. Ann Intern Med. 2003;138(9):724–35.
Jeong YJ, Yi CA, Lee KS. Solitary pulmonary nodules: detection, characterization, and guidance for further diagnostic workup and treatment. Am J Roentgenol. 2007;188(1):57–68.
Lodge MA, Badawi RD, Gilbert R, Dibos PE, Line BR. Comparison of 2-dimensional and 3-dimensional acquisition for 18F-FDG PET oncology studies performed on an LSO-based scanner. J Nucl Med. 2006;47(1):23–31.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Li, Y., Su, M., Li, F. et al. The value of 18F-FDG-PET/CT in the differential diagnosis of solitary pulmonary nodules in areas with a high incidence of tuberculosis. Ann Nucl Med 25, 804–811 (2011). https://doi.org/10.1007/s12149-011-0530-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-011-0530-y