
Abstract
Aim
To evaluate the effect of the 18F-FDG PET-CT respiratory gating (4D) study in the correct documentation of pulmonary lesions with faint uptake in standard PET-CT.
Methods
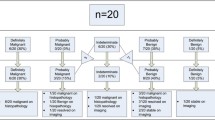
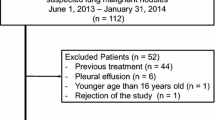
Forty-two pulmonary lesions with a low or no detectable uptake of FDG (SUVmax < 2.5) in 3D PET-CT were prospectively evaluated in 28 patients (19 males and 9 females), mean age 66.5 years (41–81). 22 patients had neoplastic background. A conventional PET-CT (3D) total body scan was performed approximately 60 min after iv injection of a mean dose of 370 MBq. Furthermore, a 4D PET-CT (synchronized with respiratory movement) thorax study was acquired. SUVmax was determined for each lesion in both studies. For the 4D studies, we selected the SUVmax in respiratory period with the highest uptake (“best bin”). We calculated the SUVmax percentage difference between 3D and 4D PET-CT (% difference = SUVmax 4D − SUVmax 3D/SUVmax 3D × 100) and the relation of this value with the size and locations of the lesions. In 4D study, any lesion with SUVmax ≥ 2.5 was classified as malignant. We assessed the changes of lesion classification (from benign to malignant) applying the 4D technique. The final diagnosis was obtained by histological assessment or clinical and radiological follow-up longer than 12 months.
Results
Forty out of 42 lesions showed an increase of SUVmax in the 4D study with respect to 3D. The mean SUVmax in the 3D and 4D PET-CT studies were 1.33 (±0.59) and 2.26 (±0.87), respectively. The SUVmax percentage difference mean between both techniques was 83.3% (±80.81).The smaller the lesion the greater was the SUVmax percentage difference (P < 0.05). No differences were observed depending on the location of the lesion. In 40% of cases, there was a change in the final classification of lesions from benign to malignant. In the final diagnosis, 24 lesions were malignant. 4D PET-CT diagnosed correctly the 52% of them.
Conclusions
The 4D PET-CT study permitted a better characterization of malignant lung lesions compared with the standard PET-CT, because of its higher sensitivity. 4D PET-CT is a recommendable technique in the early diagnosis of malignant lesions.



Similar content being viewed by others

References
Osman MM, Cohade C, Nakamoto Y, Wahl RL. Respiratory motion artifacts on PET emission images obtained using CT attenuation correction on PET-CT. Eur J Nucl Med Mol Imaging. 2003;30:603–6.
Nehmeh SA, Erdi Y, Ling CC, Rosenzweig E, Shoder H, Larson SM, et al. Effect of respiratory gating on quantifying PET images of lung cancer. J Nucl Med. 2002;43:876–81.
Bryant AS, Cerfolio RJ. The maximum standardized uptake values on integrated FDG-PET/CT is useful in differentiating benign from malignant pulmonary nodules. Ann Thorac Surg. 2006;82:1016–20.
Gould MK, Maclean CC, Kuschner WG, Rydzak CE, Owens DK. Accuracy of positron emission tomography for diagnosis of pulmonary nodules and mass lesions: a meta-analysis. JAMA. 2001;285:914–24.
Degirmenci B, Wilson D, Laymon CM, Becker C, Mason NS, Bencherif B, et al. Standarized uptake value-based evaluations of solitary pulmonary nodules using F-18 fluorodeoxyglucose-PET/computed tomography. Nucl Med Commun. 2008;29:614–22.
Kim SC, Machac J, Krynyckyi BR, Knesaurek K, Krellenstein D, Schultz B, et al. FDG PET for evaluation of indeterminate lung nodules: assigning a probability of malignancy may be preferable to binary readings. Ann Nucl Med. 2008;22:165–70.
Pevsner A, Nehmeh SA, Humm JL, Mageras GS, Erdi YE. Effect of motion on tracer activity determination in CT attenuation corrected PET images: a lung phantom study. Med Phys. 2005;32:2358–62.
Goerres GW, Kamel E, Seifert B, Burger C, Buck A, Hany TF, et al. Accuracy of image coregistration of pulmonary lesions in patients with non-small cell lung cancer using an integrated PET/CT system. J Nucl Med. 2002;43:1469–75.
Beyer T, Antoch G, Blodgett T, Freudenberg LF, Akhurst T, Mueller S. Dual-modality PET/CT imaging: the effect of respiratory motion on combined image quality in clinical oncology. Eur J Nucl Med Mol Imaging. 2003;30:588–96.
Lowe VJ, Fletcher JW, Gobar L, Lawson M, Kirchner P, Valk P, et al. Prospective investigation of positron emission tomography in lung nodules. J Clin Oncol. 1998;16:1075–84.
Erdi Y, Nehmeh SA, Pan T, Pevsner A, Rosenzweig KE, Mageras G, et al. The CT motion quantitation of lung lesions and its impact on PET-measured SUVs. J Nucl Med. 2004;45:1287–92.
Nehmeh SA, Erdi YE, Ling CC, Pevsner A, Rosenzweig KE, Yorke E, et al. Four dimensional (4D) PET/CT imaging in the thorax. Med Phys. 2004;31:3179–86.
Larson SM, Nehmeh SA, Erdi Y, Humm JL. PET-CT in non-small-cell lung cancer: value of respiratory-gated PET. Chang Gung Med J. 2005;28:306–14.
Pan T, Mawlawi O, Nehmeh SA, Erdi YE, Luo D, Liu HH, et al. Attenuation correction of PET images with respiration-averaged CT images in PET/CT. J Nucl Med. 2005;46:1481–7.
Hamill JJ, Bosmans G, Dekker A. Respiratory-gated CT as a tool for the simulation of breathing artifacts in PET and PET-CT. Med Phys. 2008;35:576–85.
Cheng N-M, Yu C-T, Ho K-C, Wu YC, Liu YC, Wang CW, et al. Respiration-averaged CT for attenuation correction in non-small-cell lung cancer. Eur J Nucl Med Mol Imaging. 2009;36:607–15.
Lupi A, Zaroccolo M, Salgarello M, Malfatti V, Zanco P. The effect of 18F-FDG-PET/CT respiratory gating on detected metabolic activity in lung lesions. Ann Nucl Med. 2009;23:191–6.
Boucher L, Rodriguez S, Lecomte R, Bénard F. Respiratory gating for 3-dimensional PET of the thorax: feasibility and initial results. J Nucl Med. 2004;45:214–9.
García Vicente AM, Soriano Castrejón A, Talavera Rubio MP, Poblete García VM, Palomar Muñoz A, Cepedello Boiso I, et al. 18F-FDG PET/CT and respiratory synchronization: effect in the detection and classification of pulmonary lesions. Rev Esp Med Nucl. 2009;28(4):181–7.
Cronin P, Dwamena BA, Kelly AM, Carlos RC. Solitary pulmonary nodules: meta-analytic comparison of cross-sectional imaging modalities for diagnosis of malignancy. Radiology. 2008;246:772–82.
Hashimoto Y, Tsujikawa T, Kondo C, Maki M, Momose M, Nagai A. et al. Accuracy of PET for diagnosis of solid pulmonary lesions with 18F-FDG uptake below the standardized uptake value of 2.5. J Nucl Med. 2006;47:426–31.
Chin BB, Green ED, Turkington TG, Hawk TC, Coleman RE. Increasing uptake time in FDG-PET: standardized uptake values in normal tissues at 1 versus 3 h. Mol Imaging Biol. 2009;11:118–22.
Nuñez R, Kalapparambath A, Varela J. Improvement in sensitivity with delayed imaging of pulmonary lesions with FDG-PET. Rev Esp Med Nucl. 2007;26:196–207.
Kim IJ, Kim SJ, Kim YS, Lee TH, Jeong YJ. Characterization of pulmonary lesions with low F18-FDG uptake using double phase F-18 FDG-PET: comparing of visual and quantitative analyses. Neoplasma. 2009;56:33–9.
Cloran FJ, Banks KP, Song, Kim Y, Bradley WC. Limitations of dual time point PET in the assessment of lung nodules with low FDG avidity. Lung Cancer. 2009. doi:10.1016/j.lungcan.2009.05.013.
Nehmeh SA, Erdi YE, Rosenzweig KE, Schoder H, Larson SM, Squire OD, et al. Reduction of respiratory motion artifacts in pet imaging of lung cancer by respiratory correlated dynamic PET: methodology and comparison with respiratory gated PET. J Nucl Med. 2003;44:1644–8.
Nehmeh SA, Erdi YE, Meirelles GSP, Squire O, Larson SM, Humm JL, et al. Deep-inspiration breathhold PET/CT of the thorax. J Nucl Med. 2007;48:22–6.
Nagel CCA, Bosmans G, Dekker ALAJ, Ollers MC, De Ruysscher DK, Lambin P, et al. Phased attenuation correction in respiration correlated computed tomography/positron emitted tomography. Med Phys. 2006;33:1840–7.
Meirelles GSP, Erdi YE, Nehmeh SA, Squire OD, Larson SM, Humm JL, et al. Deep-inspiration breathhold PET/CT: clinical findings with a new technique for detection and characterization of thoracic lesions. J Nucl Med. 2006;48:712–9.
Kawano T, Ohtake E, Inoue T. Deep-inspiration breath-hold PET/CT of lung cancer: maximum standardized uptake value analysis of 108 patients. J Nucl Med. 2008;49:1223–31.
Torizuka T, Tanizaki Y, Kanno T, Futatsubashi M, Yoshikawa E, Okada H, et al. Single 20-second acquisition of deep-inspiration breath-hold PET/CT: clinical feasibility for lung cancer. J Nucl Med. 2009;50:1579–84.
Hamberg LM, Hunter GL, Alpert NM, Choi NC, Babich JW, Fischman AJ. The dose uptake ratio as an index of flucose metabolism: useful parameter or oversimplification? J Nucl Med. 1994;35:1308–12.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
García Vicente, A.M., Soriano Castrejón, A.M., Talavera Rubio, M.P. et al. 18F-FDG PET-CT respiratory gating in characterization of pulmonary lesions: approximation towards clinical indications. Ann Nucl Med 24, 207–214 (2010). https://doi.org/10.1007/s12149-010-0345-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-010-0345-2