
Abstract
Purpose
This study was to evaluate 18F-FDG PET features of progressive massive fibrosis (PMF) and to determine the ability of FDG PET to differentiate pure PMF from PMF-associated lung cancer.
Methods
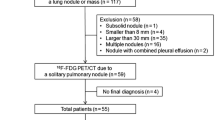
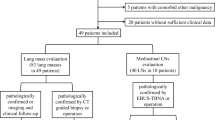
18F-FDG PET and chest computed tomography (CT) scans were performed in 9 patients with pneumoconiosis and PMF. Patients who showed active pulmonary tuberculosis on CT scan were excluded. Pure PMF was confirmed via either fine needle aspiration biopsy (n = 6) or 12 months follow-up CT scan (n = 3). CT features and PET findings were evaluated for distribution of fibrotic masses, consolidations, and nodules on CT scan and mean and maximum standardized uptake values (SUVs) of abnormalities depicted on PET scan.
Results
14 masses were detected from nine patients. On chest CT scan, PMF masses were noted with surrounding small nodules and distortion of parenchyma. The size of the lesions ranged from 1.2 to 6.4 cm in maximum diameter. FDG PET scans identified metabolically active lesions in all patients. Maximal SUV ranged from 3.1 to 14.6 and mean SUV ranged from 1.4 to 8.5.
Conclusion
FDG PET can identify PMF lesions as hypermetabolic lesions even without associated malignancy or tuberculosis. Therefore, it might have a limited role in the diagnosis of PMF with possible concurrent granulomatous inflammation or lung cancer.



Similar content being viewed by others

References
Pathology standards for coal workers’ pneumoconiosis. Report of the Pneumoconiosis Committee of the College of American Pathologists to the National Institute for Occupational Safety and Health. Arch Pathol Lab Med. 1979;103:375–432.
Spencer H. Pathology of the lung: the pneumoconiosis and other occupational lung diseases. Oxford: Pergamon; 1985. p. 413–510.
Williams JL, Moller GA. Solitary mass in the lungs of coal miners. Am J Roentgenol Radium Ther Nucl Med. 1973;117:765–70.
Bergin CJ, Muller NL, Vedal S, Chan-Yeung M. CT in silicosis: correlation with plain films and pulmonary function tests. Am J Roentgenol. 1986;146:477–83.
Soutar CA, Collins HP. Classification of progressive massive fibrosis of coalminers by type of radiographic appearance. Br J Ind Med. 1984;41:334–9.
Nemery B. Metal toxicity and the respiratory tract. Eur Respir J. 1990;3:202–19.
Scatarige JC, Stitik FP. Induction of thoracic malignancy in inorganic dust pneumoconiosis. J Thorac Imaging. 1988;3:67–79.
Scarano D, Fadali AM, Lemole GM. Carcinoma of the lung and anthracosilicosis. Chest. 1972;62:251–4.
Dholakia S, Rappaport DC. The solitary pulmonary nodule. Is it malignant or benign? Postgrad Med. 1996;99:246–50.
Viggiano RW, Swensen SJ, Rosenow EC 3rd. Evaluation and management of solitary and multiple pulmonary nodules. Clin Chest Med. 1992;13:83–95.
Hustinx R, Benard F, Alavi A. Whole-body FDG-PET imaging in the management of patients with cancer. Semin Nucl Med. 2002;32:35–46.
Rohren EM, Turkington TG, Coleman RE. Clinical applications of PET in oncology. Radiology. 2004;231:305–32.
Bandoh S, Fujita J, Yamamoto Y, Nishiyama Y, Ueda Y, Tojo Y, et al. A case of lung cancer associated with pneumoconiosis diagnosed by fluorine-18 fluorodeoxyglucose positron emission tomography. Ann Nucl Med. 2003;17:597–600.
Je SK, Ahn MI, Park YH, Kim CH. Detection of a small lung cancer hidden in pneumoconiosis with progressive massive fibrosis using F-18 fluorodeoxyglucose PET/CT. Clin Nucl Med. 2007;32(3):247–8.
O’Connell M, Kennedy M. Progressive massive fibrosis secondary to pulmonary silicosis appearance on F-18 fluorodeoxyglucose PET/CT. Clin Nucl Med. 2004;29:754–5.
Kavanagh PV, Stevenson AW, Chen MY, Clark PB. Nonneoplastic diseases in the chest showing increased activity on FDG PET. AJR Am J Roentgenol. 2004;183:1133–41.
Jung JI, Park SH, Lee JM, Hahn ST, Kim KA. MR characteristics of progressive massive fibrosis. J Thorac Imaging. 2000;15:144–50.
McCloskey M, Cook N, Cameron D, Summers Q. Progressive massive fibrosis in the absence of lung nodulation. Australas Radiol. 1997;41:63–4.
Katabami M, Dosaka-Akita H, Honma K, Saitoh Y, Kimura K, Uchida Y, et al. Pneumoconiosis-related lung cancers: preferential occurrence from diffuse interstitial fibrosis-type pneumoconiosis. Am J Respir Crit Care Med. 2000;162:295–300.
Matsumoto S, Mori H, Miyake H, Yamada Y, Ueda S, Oga M, et al. MRI signal characteristics of progressive massive fibrosis in silicosis. Clin Radiol. 1998;53:510–4.
Matsumoto S, Miyake H, Oga M, Takaki H, Mori H. Diagnosis of lung cancer in a patient with pneumoconiosis and progressive massive fibrosis using MRI. Eur Radiol. 1998;8:615–7.
Alavi A, Gupta N, Alberini JL, Hickeson M, Adam LE, Bhargava P, et al. Positron emission tomography imaging in nonmalignant thoracic disorders. Semin Nucl Med. 2002;32:293–321.
Fraser R, Pare J. Diagnosis of disease of the chest. Philadelphia: Saunders; 1989. p. 2412–3.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chung, S.Y., Lee, J.H., Kim, T.H. et al. 18F-FDG PET imaging of progressive massive fibrosis. Ann Nucl Med 24, 21–27 (2010). https://doi.org/10.1007/s12149-009-0322-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12149-009-0322-9