
Abstract
Background
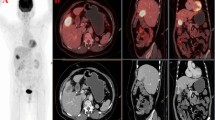
Reports concerning the clinical usefulness of 18F 2-fluoro-2-deoxy-d-glucose integrated positron emission and computed tomography (18F-FDG PET-CT) for patients with gallbladder cancer and cholangiocarcinoma are relatively scarce. The purpose of this study was to assess the diagnostic value of PET-CT in relation to a conventional imaging modality, multidetector row CT (MDCT), for patients with gallbladder cancer and cholangiocarcinoma.
Methods
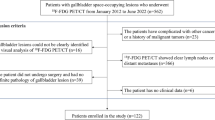
Ninety-nine patients with suspected gallbladder cancer and cholangiocarcinoma who underwent both PET-CT and MDCT for initial staging were included in our study. The results of these two imaging modalities for evaluating primary tumors, regional lymph nodes and distant metastases were compared with the final diagnoses based on pathological or clinical findings.
Results
A maximum standardized uptake value (SUVmax) of 3.65 was found to be the best cutoff value for detecting a malignant tumor. The overall values for the sensitivities, specificities, positive predictive values (PPVs), negative predictive values (NPVs) and the accuracies of PET-CT and MDCT for the detection of a primary tumor were 90.2, 70.6, 93.7, 60.0, 86.9% and 84.2, 70.6, 93.2, 48.0, 81.8%, respectively. PET-CT demonstrated no significant advantage over MDCT for the diagnosis of a primary tumor. PET-CT showed a significantly higher PPV (94.1 vs. 77.5%, P = 0.04) than that found for MDCT in the diagnosis of regional lymph node metastasis. Additionally, PET-CT showed a significantly higher sensitivity (94.7 vs. 63.2%, P = 0.02) than that found for MDCT in the diagnosis of distant metastasis.
Conclusions
PET-CT is valuable for detecting regional lymph node involvement and unsuspected distant metastases that are not diagnosed by MDCT.

Similar content being viewed by others

References
Farley DR, Weaver AL, Nagorney DM. “Natural history” of unresected cholangiocarcinoma: patient outcome after noncurative intervention. Mayo Clin Proc. 1995;70:425–9.
Ruckert JC, Ruckert RI, Gellert K, Hecker K, Muller JM. Surgery for carcinoma of the gallbladder. Hepatogastroenterology. 1996;43:527–33.
Miyazaki M, Ito H, Nakagawa K, Ambiru S, Shimizu H, Okuno A, et al. Does aggressive surgical resection improve the outcome in advanced gallbladder carcinoma? Hepatogastroenterology. 1999;46:2128–32.
Chijiiwa K, Tanaka M. Carcinoma of the gallbladder: an appraisal of surgical resection. Surgery. 1994;115:751–6.
Fong Y, Jarnagin W, Blumgart LH. Gallbladder cancer: comparison of patients presenting initially for definitive operation with those presenting after prior noncurative intervention. Ann Surg. 2000;232:557–69.
Jarnagin WR, Fong Y, DeMatteo RP, Gonen M, Burke EC, Bodniewicz BJ, et al. Staging, resectability, and outcome in 225 patients with hilar cholangiocarcinoma. Ann Surg. 2001;234:507–17; discussion 517–9.
Morimoto Y, Tanaka Y, Ito T, Nakahara M, Nakaba H, Nishida T, et al. Long-term survival and prognostic factors in the surgical treatment for intrahepatic cholangiocarcinoma. J Hepatobiliary Pancreat Surg. 2003;10:432–40.
de Groen PC, Gores GJ, LaRusso NF, Gunderson LL, Nagorney DM. Biliary tract cancers. N Engl J Med. 1999;341:1368–78.
Park MS, Kim TK, Kim KW, Park SW, Lee JK, Kim JS, et al. Differentiation of extrahepatic bile duct cholangiocarcinoma from benign stricture: findings at MRCP versus ERCP. Radiology. 2004;233:234–40.
Cha JM, Kim MH, Jang SJ. Early bile duct cancer. World J Gastroenterol. 2007;13:3409–16.
Hany TF, Steinert HC, Goerres GW, Buck A, von Schulthess GK. PET diagnostic accuracy: improvement with in-line PET-CT system: initial results. Radiology. 2002;225:575–81.
Lardinois D, Weder W, Hany TF, Kamel EM, Korom S, Seifert B, et al. Staging of non-small-cell lung cancer with integrated positron-emission tomography and computed tomography. N Engl J Med. 2003;348:2500–7.
Selzner M, Hany TF, Wildbrett P, McCormack L, Kadry Z, Clavien PA. Does the novel PET/CT imaging modality impact on the treatment of patients with metastatic colorectal cancer of the liver? Ann Surg. 2004;240:1027–34. discussion 1035–6.
Heinrich S, Goerres GW, Schafer M, Sagmeister M, Bauerfeind P, Pestalozzi BC, et al. Positron emission tomography/computedtomography influences on the management of resectable pancreatic cancer and its cost-effectiveness. Ann Surg. 2005;242:235–43.
Kim JY, Kim MH, Lee TY, Hwang CY, Kim JS, Yun SC, et al. Clinical role of 18F-FDG PET-CT in suspected and potentially operable cholangiocarcinoma: a prospective study compared with conventional imaging. Am J Gastroenterol. 2008;103:1145–51.
Antoch G, Saoudi N, Kuehl H, Dahmen G, Mueller SP, Beyer T, et al. Accuracy of whole-body dual-modality fluorine-18-2-fluoro-2-deoxy-d-glucose positron emission tomography and computed tomography (FDG-PET/CT) for tumor staging in solid tumors: comparison with CT and PET. J Clin Oncol. 2004;22:4357–68.
Lim JH. Cholangiocarcinoma: morphologic classification according to growth pattern and imaging findings. Am J Roentgenol. 2003;181:819–27.
Greene FL, Page DL, Flemming ID, Fritz A, Balch CM, Haller DG, et al. AJCC cancer staging manual, 6th ed. New York: Springer; 2002.
Petrowsky H, Wildbrett P, Husarik DB, Hany TF, Tam S, Jochum W, et al. Impact of integrated positron emission tomography on staging and management of gallbladder cancer and cholangiocarcinoma. J Hepatol. 2006;45:43–50.
Jadvar H, Henderson RW, Conti PD. [F-18] Fluorodeoxyglucose positron emission tomography and positron emission tomography: computed tomography in recurrent and metastatic cholangiocarcinoma. J Comput Assist Tomogr. 2007;31:223–8.
Kato T, Tsukamoto E, Kuge Y, Katoh C, Nambu T, Nobuta A, et al. Clinical role of 18F-FDG PET for initial staging of patients with extrahepatic bile duct cancer. Eur J Nucl Med. 2002;29:1047–54.
Acknowledgments
This study was financially supported by grant from the IN-SUNG Foundation for Medical Research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lee, S.W., Kim, H.J., Park, J.H. et al. Clinical usefulness of 18F-FDG PET-CT for patients with gallbladder cancer and cholangiocarcinoma. J Gastroenterol 45, 560–566 (2010). https://doi.org/10.1007/s00535-009-0188-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00535-009-0188-6